

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Shift work is an arrangement of working hours whereby two or more teams of workers extend the hours of operation beyond those of conventional office hours.1 Shift work is crucial to the 24-h operation of modern societies to meet economic and social demands in terms of cost-effective production and round-the-clock services. It is estimated that nearly one-fifth of the total global workforce works in shifts,2 with this increasing to about 50% for protective and food-preparation services.3 There are various types of shift work, such as three-shift schedule, two-shift schedules, and permanent night work, with various shift patterns of forward or backward, continuous or discontinuous, irregular, or fast rotations being utilized.45
Irregular sleep-wake patterns disrupt the normal circadian rhythm in which wakefulness normally occurs during the daytime. The desynchronization of the circadian rhythm in shift work makes it difficult to sleep during the day and be alert at night. Aside from sleep disturbances, such desynchronization is also associated with negative health outcomes and safety issues in shift workers.678 Approximately 10% of shift workers require medical attention for severe sleep disorders that are directly related to shift work.9
Firefighting and nursing are strenuous occupations associated with high stress and workload levels.1011 These occupations have distinctive characteristics, such as firefighters predominantly being male and nurses predominantly being female, and firefighters work in a 24-h-every-other-day shift schedule with duty periods that vary according to emergency calls received, while nurses are typical shift workers who usually work in a rapidly rotation. A recent study found that 59% of USA firefighters suffered from a sleep disorder.10 The sleep disturbances in firefighters have been reported to be related to psychological distress, excessive alcohol consumption, cigarette smoking, depression, and chronotype.12 The prevalence of sleep disturbances was reportedly three-to-four times higher in nurses working rotating shifts than in the general population.13 Flo et al.14 also reported that the prevalence of shift-work sleep disorders in nurses was 32.4–37.6% depending on the assessment method used, with the prevalence being higher in a three-shift rotation than in other shift schedules: day work, two-shift rotation, night work only, or other schedules involving night work. Fatigue and sleepiness due to the irregular work and sleep schedules of nurses increase the risk of various medical errors or accidents, traffic accidents, and health problems.151617 A longitudinal Norwegian study suggested that predictive factors for the disappearance of shift-work sleep disorders in nurses at follow-up were stopping night shifts, fewer nights worked during the previous year, and lower daytime sleepiness scores at baseline.18
Previous studies of shift workers have largely focused on the differences in sleep disturbances and health problems between shift workers and day workers (DWs), with relatively few researches investigating specific shift-worker jobs.192021 In the present study we compared the following shift schedules in terms of sleep and mood disturbances: firefighters work in a 24-h-every-other-day shift schedule (EOD), nurses working in a rapid rotating three-shift schedule (3S), and dayworkers DW. We also investigated several clinical factors that are possibly associated with sleep disturbances, including age, caffeine consumption, and alcohol consumption, and considered the individual chronotypes of shift workers.
METHODS
Subjects
Two hundred and eighty-eight workers aged 20–50 years were initially recruited consecutively from July to September 2015, of which 12 were excluded due to incomplete questionnaires. The subjects included two types of shift workers (rotating EOD and rapid rotating 3S) plus DW. Each group represents different workforces: the members of the EOD group were recruited from a fire station in the Gyeonggi province of Korea, those in the 3S group were recruited from a university hospital in the same province, and the DW workers were volunteer government officials or nonmedical hospital employees who worked from 9 a.m. to 6 p.m. in either Gyeonggi province or Seoul. EOD worked in a forward rotation shift from 9 a.m. to 9 a.m. (24 h) that involved working every other day. 3S had three work schedules: an 8-h day shift from 7 a.m. to 3 p.m., a 7.5-h evening shift from 2:30 p.m. to 10 p.m., and a 10-h night shift from 9:30 p.m. to 7:30 a.m. The forward rotation schedule involved two day shifts, two evening shifts, one rest day, three night shifts, and two rest days. The Institutional Review Board of Sungshin Women's University approved this study (approval no: SSWUIRB 2015-057).
Questionnaires
The analyzed demographic data included age, education level, working hours, and health habits (alcohol consumption, cigarette smoking, caffeine consumption, and hypnotic medications). Subjects were scored using sleep-related questionnaires.
Morningness-Eveningness Questionnaire
The Korean version of the Morningness-Eveningness Questionnaire (MEQ) consists of 19 items pertaining to habitual rising times and bedtimes, preferred times of physical and mental performance, and subjective alertness after rising and before going to bed.22 Five of the questions are timescales divided into 1-h or 15-min intervals, and the other 14 questions are measured on a 4-point Likert scale. Most of the questions relate to preferred rather than actual times. The MEQ summed scores range from 16 to 86, and in this study they were divided into the following three chronotypes: evening type (16–41 points), intermediate type (42–58 points), and morning type (59–86 points).22 The reliability of the MEQ was indicated by a Cronbach's alpha of 0.72.
Insomnia Severity Index
The Korean version of the seven-item Insomnia Severity Index (ISI) subjectively assesses the severity of insomnia symptoms (difficulty falling asleep, difficulty maintaining sleep, or early morning awakening) as well as their consequences. The ISI includes satisfaction with current sleep patterns, interference with daytime functioning, how noticeable the sleep impairment is to others, and the degree of worry or distress related to the sleep problems during the past 2 weeks. Subjects grade each question from minimal (0 points) to very severe (4 points), and the final score ranges from 0 to 28 points, with higher scores indicating more-severe insomnia.23 The reliability of the ISI was indicated by a Cronbach's alpha of 0.85.
Epworth Sleepiness Scale
The Epworth Sleepiness Scale (ESS) measures the impact of subjective daytime sleepiness.24 The Korean version of the ESS consists of eight items on the likelihood of falling asleep in a particular common daily situation. The score for each item ranges from 0 (would never doze) to 3 (high probability of dozing), with total scores ranging from 0 to 24. A raw total score ≥10 points is considered to indicate excessive daytime sleepiness.24 The reliability of the ESS was indicated by a Cronbach's alpha of 0.80.
Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) is used to determine the levels of anxiety and depression that a patient is experiencing. The HADS is a 14-item scale that generates ordinal data and is divided into 7 items related to anxiety (HADS-A) and 7 related to depression (HADS-D). Each item on the questionnaire is scored from 0 to 3, resulting in a total scores of between 0 and 21 for anxiety and depression.25 The generally accepted cutoff score that indicates the presence of anxiety or depression is 8 points.26 The reliabilities of the HADS-A and HADS-D were indicated by Cronbach's alpha values of 0.88 and 0.82, respectively.
Statistical analysis
Statistical analyses were conducted using the SPSS (Windows version 19.0, SPSS Inc., Chicago, IL,USA). The criterion for statistical significance was a two-tailed p value of <0.05. Continuous data are expressed as mean±SD values, and categorical data are expressed as frequencies and percentages. All continuous variables were analyzed using the Kruskal-Wallis test due to uneven distributions, followed by the Mann-Whitney U-test using Bonferroni correction to adjust the probability. Categorical variables were analyzed using the chi-square test or Fisher's exact test. Correlation analysis was performed by calculating partial Spearman's correlation coefficients adjusted for age and sex.
Additionally, stepwise method multiple linear regression analysis was performed to predict the sleep disturbances, depressive mood, and anxiety symptoms experienced by subjects after adjusting for demographic variables (age and sex), individual chronotype (MEQ score), habitual factors (alcohol consumption, smoking, and caffeine consumption), and shift type.
RESULTS
Participant characteristics
The questionnaires were completed by 276 participants: 60 EOD (21.7%), 77 3S (27.9%), and 139 DW (50.4%). 3S were younger (28.70±5.13 years) than EOD (42.80±9.38 years) and DW (40.10±8.30 years) (p<0.001), and females predominated (p<0.001). While alcohol consumption and smoking were predominantly seen in DW, caffeine consumption was high in all workers. No hypnotic drug use was seen in EOD, but 13% of 3S used hypnotic drugs for sleep (p<0.001). Working overtime was reported in 3S and DW, but not in EOD. The actual work hours for DW were 10.50±1.77 h for a designated 9 h of work, and 3S also exhibited longer working hours of 8.90±0.85, 8.70±0.85, and 11.30±0.80 h for their 8-h day, 7.5-h evening, and 9.5-h night shifts, respectively. The estimated working time per week was 84.00±12.10 h for EOD, 48.73±7.40 h for 3S, and 51.5±8.9 h for DW (Table 1).
Sleep and mood disturbances, and individual chronotypes
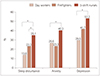
Sleep disturbances as evaluated by the ISI questionnaires were worse in shift workers. Post-hoc analyses also revealed that both EOD and 3S had significantly greater severities of insomnia symptoms than did DW (p<0.001) (Fig. 1). The severities of clinically significant insomnia symptoms (ISI score >14) were also greater in both EOD and 3S than in DW. The ISI score was highest in 3S, but the difference compared to EOD was not statistically significant. The daytime sleepiness as evaluated by the ESS questionnaires was high in all groups regardless of work schedules, and did not differ significantly between the groups (Table 2).
Mood disturbances of depressive mood and anxiety symptoms were assessed using the HADS. 3S showed a significantly higher prevalence of depressive mood and anxiety symptoms compared to DW in post-hoc analysis (p=0.014 and p=0.007, respectively). The prevalence rates of clinically significant depressive mood (HADS-D score ≥8) and anxiety symptoms (HADS-A score ≥8) in 3S were 53.2% and 40.3%, respectively. Depressive mood and anxiety symptoms were markedly worse in 3S than in EOD (Table 2).
Individuals were categorized into morning, intermediate, and evening chronotypes using the MEQ. The intermediate chronotype was the most common in all groups, comprising 58.3%, 64.9%, and 71.9% of EOD, 3S, and DW, respectively. 3S was remarkable for the high prevalence (32.5%) of evening chronotype but very low prevalence (2.6%) of morning chronotype (Table 1).
Analyses of correlations between sleep disturbances and other variables
Considering the presence of significant differences between groups in age and sex, a partial Spearman correlation analysis was performed after adjusting for age and sex. The chronotypes in EOD and 3S were not correlated with other variables. On the other hand, in the DW group correlation analysis revealed that the MEQ score was negatively correlated with depressive mood based on the HADS-D score (rho=−0.227, p=0.028) (Supplementary Table 1 in the online-only Data Supplement).
However, there were significant correlations between ISI and depressive mood and anxiety symptoms for both EOD (rho=0.57 and p<0.05, and rho=0.57 and p<0.05, respectively), and 3S (rho=0.37 and p<0.05, and rho=0.33 and p<0.05, respectively) (Supplementary Table 1 in the online-only Data Supplement).
Stepwise multiple regression analyses of the effects of other variables on ISI, HADS-D, and HADS-A scores
The stepwise multiple linear regression analysis was conducted to identify the ISI, HADS-D, HADS-A scores in shift workers that were closely related to demographics (age and sex), individual chronotype (MEQ score), habitual factors (alcohol consumption, smoking, and caffeine consumption), and shift type. Insomnia symptoms were affected by the sex, chronotype, EOD shift, and 3S shift, with these predictors accounting for 16.5% of the ISI score. 3S is a response variable for anxiety symptoms, and accounts for 0.038% of the HADS-A score, while the MEQ score is a response variable for depressive mood that accounts for 0.035% of the HADS-D score (Table 3).
DISCUSSION
This study found that shift workers suffered more insomnia symptoms than did DW regardless of their shift schedules. There are only a few reports on the effects of different shift schedules on sleep disturbances, and the reported related factors have largely been inconclusive. Insomnia symptoms were reported to be similar among jobs involving night, day, and rotating shifts.927 On the other hand, it has been suggested that the percentage of shift workers suffering from insomnia varies with the type of night work and specific work schedules.27 The fewer insomnia symptoms in firefighters in the present study may be explained by distinguishing the shift schedule of a rotating EOD shift. Regarding job-specific factors, the work of firefighters is determined by the frequency of incoming emergency calls, with more emergency calls leading to shorter rest periods. Rest time during work might partially compensate the circadian misalignment and sleep disturbances in firefighters.
Our study suggested that the severity of mood disturbance is associated with the shift-work schedule. The shift-work nurses reported significantly greater depressive mood and anxiety symptoms compared to firefighters. This finding indicates that while mood disturbances are more prevalent in shift workers, they might also be affected by the different shift schedules. Such a relationship has previously been found for mood disturbances.28 However, the findings for the overall association between mood symptoms among shift workers have been inconsistent.29 This variation might be mainly attributable to differences in study populations and shift-work-specific factors such as the shift type, experiencing night shifts, and the duration of shift work, as well as the questionnaires used for assessments.
The two shift schedules (EOD and 3S) analyzed in this study can be predictors of insomnia symptoms. 3S is also a predictor of anxiety symptoms, with minimal accountability. This indicates that shift schedules can affect the presence or severity of sleep disturbances and anxiety symptom.
Excessive daytime sleepiness is another common sleep symptom in shift workers.30 Our study found that excessive daytime sleepiness is present regardless of the work schedule, including in DW. Considering social and behavioral factors, Koreans work for a mean of 2,024 h per year, which is in the top 3 of 35 OECD countries.31 Moreover, Koreans sleep for only a mean of 462 minutes per night, which is the lowest among 28 OECD countries.32 Together these statistics indicate that long working hours and short total sleep times is likely to have contributed to the excessive daytime sleepiness that was present even in DW.
The chronotype in shift workers is related to mood symptoms in DW but not in shrift workers. Chronotype in DW indicates that the eveningness chronotype is related to a greater depressive mood after adjusting for age and sex in DW. It has generally been accepted that workers with the evening chronotype are better adapted to shift work, although contrary results have been reported recently, with the evening chronotype being associated with poor sleep quality and shift-work disorder in nurses performing shift work.3334 The chronotype in shift workers was found even more recently to exert different effects on each type of shift schedule, with the earlier chronotype being associated with a shorter sleep duration during night shifts, higher levels of social jet lag, as well as more sleep disturbances, and with a similar pattern for the later chronotype during early shifts.35 It should be noted that there MEQ score is a response variable for depressive mood that accounts for 0.035% of the HADS-D score in shift workers. Although, it is only a weak correlation between eveningness chronotype in shift workers with depressive mood, and so further assessments involving large samples and control groups for sex, age, shift type, and a single occupation group are needed.
The prevalence of the evening chronotype was higher in shift-work nurses, with only two cases (2.6%) of the morning type. This is largely explainable by age factors. More than 70% of the Korean nurses working in hospitals have a working career of shorter than 10 years.36 Considering that younger shift-work nurses and the evening chronotype are much commonly seen in younger subjects, the higher prevalence of the evening chronotype may be greatly affected by age.37
The correlation analysis performed in our study only revealed significant associations of insomnia symptom severity with depressive mood and anxiety symptoms in all groups. About half of the included shift-work nurses and firefighters reported having a depressive mood. Psychiatric morbidities are commonly reported in shift workers.938 Individuals who developed shift-work sleep disorders reported exhibited larger increases in depression and anxiety symptoms.39 The present study found positive correlations between the severity of insomnia symptoms and depressive mood and anxiety symptoms in both shift workers and DW, but the correlations were much stronger in shift workers. We cannot confirm the cause and causality of these two correlations, but we suggest that they are bidirectional effects. A bidirectional relationship between mood disturbance and insomnia has been reported in sleep disturbances,40 which suggests that shift workers with worse insomnia symptoms have worse depressive mood and anxiety symptoms.
Sleep patterns in firefighters are probably disrupted by changes in the shift duration and unpredictability of emergency calls. Aside from sleep disturbances, psychosomatic considerations also include binge drinking, smoking, depression, and poor social relationships.10 Some of these factors are interrelated, such as depressed firefighters being more likely to be sleep deprived and exhibit hazardous drinking behaviors.1012 However, some of these poor health behaviors may be an acceptable norm of the social situation in which relief is required from the job demands.10 The present firefighters showed poor health behaviors of greater alcohol consumption and smoking compared to the shift-work nurses. Although age- and sex-related factors need to be considered, the mood disturbance in young female nurses may be related to a lack of adequate coping mechanisms to relieve depression and anxiety.4142 Overall, anxiety symptoms are much more prevalent in shift workers than DW, but the underlying cause may differ according to certain job-specific factors. For example, those experienced by firefighters might be more related to the frequency of emergency calls and poor health behaviors, while those of shift-work nurses might be more related to their vulnerability to mood disturbance with poor coping behaviors.
This study was subject to some limitations. First, the study compared the two-shift systems of two distinct workforces. Considering the unique characteristics of each shift system, further studies are needed to compare different shifts in a single workforce. Second, the age and sex distributions differed, with young females predominating among shift-work nurses and middle-aged males predominating among firefighters, which is due to nurses and firefighters being highly distinct occupations. Third, our study relied upon subjective reports and questionnaires. Clinical evaluations and diagnoses of underlying medical conditions, sleep disorders, and mental disorders were not performed, which might have obscured the effects of shift schedule on sleep and mood symptoms.
In conclusion, We found that sleep disturbances are more common in shift workers than in DW. Depressive mood and anxiety symptoms were worse in shift-work nurses then firefighters, indicating that reported sleep and mood disturbances may vary depending on shift schedules. The eveningness chronotype may have relationship to the depressive mood in shift workers. These findings indicate that health promotion and intervention programs need to consider strategies tailored to different shift schedules when attempting to improve sleep and mood disturbances.



 XML Download
XML Download