

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebrospinal fluid (CSF) volume depletion is a disorder mainly caused by the leakage of spinal CSF. The annual incidence of spontaneous spinal CSF leakage has been estimated at 5 per 10,000,1 while that of other types of CSF volume depletion is unknown. Females are affected more commonly than males, peaking at around 40 years of age.1 Patients with CSF volume depletion present with various symptoms, including orthostatic headache, neck pain, dizziness/vertigo, visual disturbance, tinnitus, nausea, numbness, back pain/lumbago, fatigability, and memory disturbance.2
The etiologies of CSF volume depletion include a true hypovolemic state, traumatic CSF leakage, iatrogenic CSF leakage, and spontaneous CSF leakage. The causes of traumatic CSF leakage include motor vehicle collisions, sports injuries, falls, brachial plexus avulsion injuries, and nerve root avulsions.2 The causes of spontaneous CSF leakage include a preexisting dural sac weakness frequently associated with meningeal diverticula, a trivial trauma in the setting of preexisting dural weakness, and spondylotic spurs or herniated discs, while in some cases the cause is completely unknown.2
Headache is the most common clinical symptom experienced by patients with CSF leakage, but occasionally headache may be completely absent. Such headaches are mostly orthostatic, and the latency of headache onset or resolution from a change in posture commonly varies with chronicity. Such headaches are often aggravated by Valsalva-type maneuvers. Not all orthostatic headaches may be due to intracranial hypotension.23 Sagging of the brain is thought to be the main cause of orthostatic headaches due to CSF leakage. Dilatation of the cerebral veins and venous sinuses might also be contributory mechanisms.4
CSF leakage is also associated with various manifestations other than headache, with one or more such manifestations being the dominant clinical feature in some cases.5678 Various manifestations other than headache include nausea with or without emesis, cochleovestibular manifestations,9 visual symptoms, numbness or paresthesias, recent memory disturbance, and trouble with bowel or bladder control.101112 The CSF opening pressure (OP) is usually low and in rare cases even negative, but is occasionally within normal limits.2
Radioisotope (RI) cisternography is performed with the intrathecal (IT) injection of indium-111 by lumbar puncture, whose dynamics are followed by sequential scanning for up to 24 hours. The early appearance of radioactivity in the bladder represents fairly common indirect evidence that the injected RI has entered the venous system rapidly. In addition, the presence of parathecal activity is often considered to be direct evidence of CSF leakage, pointing to the approximate site of the leak.2 Meningeal diverticula may appear as foci of parathecal activity and sometimes might not be reliably distinguished from actual sites of leakage.2
CSF leakage appears in head magnetic resonance imaging (MRI) as a decrease in the size of the ventricles, descent of the cerebellar tonsils, the collection of subdural fluids, sinking of the brain, hyperemia of the pituitary gland, diffuse pachymeningeal enhancement, and enlargement of cerebral venous sinuses.213 Performing spinal MRI at a high rate can detect abnormalities such as epidural CSF collection on fat-suppressed heavily T2-weighted images and distention of the epidural veins.14 Computed tomography (CT) myelography is considered the most-accurate approach for demonstrating the exact site of spinal CSF leakage.5 In addition, it can show meningeal diverticula, dilated nerve root sleeves, and extra-arachnoid fluid collections.2
An epidural blood patch (EBP) is now considered the treatment of first choice for spinal CSF leakage in those patients who have not responded to initial conservative management.215 The efficacy of an EBP is reported to be approximately 30%,16 and many patients often require more than one of them, with some even requiring several.2
We have newly diagnosed and treated 118 patients with CSF leakage with an EBP during the past 3 years. An EBP was applied after spinal CSF leakage had been definitively detected based on radiological findings. Predictors of a positive response to an EBP for spontaneous spinal CSF leakage have been reported in a few articles,1718 while those of a positive response to an EBP for traumatic spinal CSF leakage have not been reported previously. The aim of the current study was to elucidate factors predicting the response to an EBP. Here we report the predictors of a positive response to an EBP for both spontaneous and traumatic spinal CSF leakage.
METHODS
Patients and variables
This study was approved by the Institutional Review Board of the International University of Health and Welfare Atami Hospital in 2018. All patients provided informed consent after the study had been explained to them (IRB No. 2018-2). The 118 enrolled patients with newly diagnosed spinal CSF leakage were treated with EBP at the Neurosurgical Section of the International University of Health and Welfare Atami Hospital. The inclusion criteria were 1) newly diagnosed as spinal CSF leakage based on neuroradiological signs and 2) received the first EBP at this hospital between July 2015 and December 2017. Exclusion criteria were 1) >7 years from the onset to EBP application or 2) having undergone EBP previously. Spinal CSF leakage was defined based on neuroradiological demonstration according to the standard diagnostic criteria.4
We examined the following factors in the included patients: age, sex, etiology, symptoms, CSF OP, rate of RI remaining after 24 hours, neuroradiological findings (MRI, CT, and RI cisternography), period from the onset to EBP application, and response to the EBP. The neuroradiological studies comprised spinal MRI, CT myelography, RI cisternography, and single-photon-emission CT (SPECT) with indium-111. RI cisternography was performed immediately after the IT injection of RI, 6 hours later, and 24 hours later. SPECT scanning and CT myelography were performed 24 and 3 hours after the IT injection, respectively. Lumbar puncture was performed in the decubitus position using a 70- or 90-mm-long 25-gauge pencil needle for the IT injection of RI and CT myelography contrast medium, and the CFS OP was measured at the same time. Any epidural CSF leakage of RI or CT myelography agent at the puncture site was excluded from the amount of epidural CSF leakage. The symptoms examined included headache (orthostatic or not), nuchal pain, back pain, vertigo/dizziness, nausea, photophobia, fatigability, numbness of extremities, and memory disturbance.
A targeted EBP was applied using a 20-gauge Tuohy needle via a midline approach under X-ray fluoroscopy system guidance with the patient in the prone position. The epidural space was identified using the loss-of-resistance technique for a lumbar EBP and using the hanging-drop technique for a cervical or thoracic EBP. Accurate localization was confirmed by ensuring the spread of the injected contrast medium over the targeted epidural space. Autologous blood mixed with contrast medium was slowly injected until the patient began to complain of radicular pain, back pain, headache, or nausea, with a maximum of 30 mL delivered. After the procedure, the localization of the epidural autologous blood was confirmed by CT (Fig. 1). The patient then remained in the supine position for at least 2 hours.
At 3 months after the application of the EBP, the responses to it were classified into four categories: excellent, good, fair, and stationary/worse. An excellent response was when the symptoms disappearing immediately and/or dramatically after the EBP application, a good response was when the symptoms had mostly (≥50%) recovered at 3 months after the EBP application, a fair response indicated that symptoms had partially (<50%) recovered at 3 months after the EBP application, and stationary/worse outcome was when the symptoms remained stationary or had worsened at 3 months after the EBP application. The correlations between the response to an EBP and other factors were analyzed statistically. In addition, differences of the responses to EBPs between spontaneous and traumatic CSF leaks were analyzed statistically.
RESULTS
The ages of the 118 patients ranged from 8 to 82 years, with a mean age of 36.7 years, and they comprised 66 females and 52 males. The etiologies of CSF leakage were traumatic for 64 patients, spontaneous for 47, and iatrogenic for 7. The traumatic events causing CSF leakage were classified into 46 motor vehicle collisions (9 involving a bicycle/motor bicycle, 26 being rear-end collisions while driving, 8 being frontal or side collisions when driving, and 3 being collisions while walking), 13 falls/head blows, and 5 sports injuries. Iatrogenic events were categorized into four lumbar punctures, two spinal therapies, and one dental treatment (Table 1). The interval from the onset to EBP application ranged from 0.5 to 84 months, with a median of 20 months. The rate of RI remaining after 24 hours after the IT injection ranged from 1.3% to 47.6%, with a mean of 21.4%. The CSF OP ranged from 0 to 16 cm H2O, with a mean of 7.6 cm H2O.
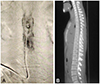
Regarding symptoms, whole headache was found in 97 patients (82.6%), with orthostatic headache found in 87 of these 97 (89.7%). Fatigability occurred in 56 patients (47.5%) patients, vertigo/dizziness in 54 (45.8%), nausea in 34 (22.0%), photophobia in 26 (22.0%), numbness in 26 (22.0%), back pain/lumbago in 27 (22.9%), memory disturbance in 25 (21.2.%), and nuchal pain in 46 (39.0%) (Table 2). Spinal MRI revealed epidural CSF collection in 56 patients (47.5%; Fig. 2, Table 2). There were CT myelography findings of epidural CSF leakage in 113 patients (95.8%; Fig. 3, Table 3), and RI cisternography findings of epidural CSF leakage in 105 (89.0%; Fig. 4, Table 3). The responses to EBPs were categorized as excellent in 21 patients (17.8%), good in 48 (40.7%), fair in 24 (20.3%), and stationary/worse in 25 (21.2%).
Our analysis of the relationships between positive responses to EBPs and the above variables revealed that the variables that significantly (p<0.05) predicted a positive response to an EBP were age <40 years (p=0.005), <1.5 years from the onset to EBP application (p<0.001), <20% RI remaining after 24 hours (p=0.002), RI cisternography findings with epidural CSF leakage except for spinal puncture sites (p=0.030), MRI findings with epidural CSF collection on fat-saturated T2-weighted images (p=0.034), CSF OP <7 cm H2O (p=0.019), orthostatic headache (p=0.015), nausea (p=0.013), nuchal pain (p=0.041), and photophobia (p=0.019). The investigated factors that did not significantly predict a positive response to an EBP were etiology (p=0.680), sex (p=0.060), CT myelography findings with epidural CSF leakage except for spinal puncture sites (p=0.460), whole headache (p=0.120), back pain (p=0.380), vertigo/dizziness (p=0.120), fatigability (p=0.360), memory disturbance (p=0.090), and numbness of extremities (p=0.700) (Table 2). Regarding the differences of the responses to EBPs between spontaneous and traumatic CSF leaks, the rate of RI remaining (p=0.017), CSF OP (p=0.006), and orthostatic headache (p=0.008) were more significant predictors in traumatic CSF leaks than in spontaneous ones. In contrast, the interval from the onset to EBP application (p<0.001) was a more significant predictor in spontaneous CFS leaks than in traumatic ones. There were no differences in the responses to EBPs for the other variables between spontaneous CFS leaks and traumatic ones.
DISCUSSION
An EBP has been recommended as the treatment of choice for patients who have not responded to initial noninvasive treatments such as hydration and bed rest.15 The effect of EBP is twofold: 1) an immediate effect related simply to volume replacement by compressing the dura mater; and 2) a subsequent latent effect related to sealing of the CSF leakage.1920 The success rate with a first EBP has been reported to be at least 30%.21 However, many patients require more than one EBP or other treatments such as epidural saline/fibrin glue infusion and IT fluid infusion.2223242526 In the present study we aimed to elucidate predictors of a positive response to an EBP based on clinical characteristics, subjective symptoms, and neuroradiological signs, which revealed that these predictors were age, interval from the onset to EBP application, rate of RI remaining after 24 hours, epidural CSF collection in MRI, epidural CFS leak in RI cisternography, orthostatic headache, nuchal pain, photophobia, and nausea. Our finding that being younger and having a shorter interval from the onset to EBP application were significant predictors suggests that spinal CSF leakage should be treated early. The remaining activity in RI cisternography has similar significance to early bladder activity in RI cisternography as a predictor of a positive response to an EBP. Early bladder activity and the rapid disappearance of radioactivity from the CSF space are indirect findings for CSF leakage.27 The rate of remaining RI is inversely related to the RI clearance rate, and the rate of RI remaining expressed as a percentage might provide a more-exact assessment than early bladder activity in RI cisternography. Epidural CSF collection in MRI and epidural CFS collection in RI cisternography represent direct evidence of spinal CSF leakage. Those signs were found to be predictors, while epidural CSF collection in CT myelography found in most of the present cases was a somewhat ambiguous sign and might be useful only for diagnosing CSF leakage rather than predicting an EBP response. Regarding subjective symptoms, orthostatic headache, nuchal pain, photophobia, and nausea were significant predictors, whereas the other symptoms—which are probably not specific to those patients—were not. However, a previous study18 found that the severity of the symptom (but not the symptom alone) was related to a positive response to an EBP.
Predictors of a positive response to an EBP in cases of spontaneous CFS leakage have been reported recently. Comparing between patients treated only once with EBP and those treated twice or more revealed that early bladder activity in RI cisternography and brain sagging are significant predictors, whereas the other variables were not.17 In the current study, brain MRI findings were excluded from the analyzed variables because these have already been reported.18
Comparisons between responders and nonresponders to a first EBP showed that a greater injected blood volume, anterior epidural CSF collection length, and midbrain–pons angle in MRI were significant predictors of a positive treatment response to the first EBP;19 whereas the other variables were not. Similarly, as for several symptoms, tinnitus was found to be a weak predictor, whereas the other investigated symptoms were not significant predictors. Regarding MRI signs, epidural CSF collection and anterior CSF collection were weak predictors, whereas the other MRI signs were not significant predictors.18
Those previous studies were based on comparisons between two groups: responders to the first EBP and nonresponders to the first EBP or patients who required two or more EBPs.1718 In contrast, our study was not based on comparisons between two groups, instead analyzing between two categories of variables and four groups of responses to EBPs. We found that age, interval from the onset to EBP application, rate of RI remaining after 24 hours, epidural CSF leakage in RI cisternography, epidural CFS collection in MRI, orthostatic headache, nausea, nuchal pain, and photophobia were significant predictors of a positive response to an EBP, whereas the CSF OP and all of the symptoms investigated were not identified as predictors. Being younger (age <40 years) was found to be a predictor of a positive response to an EBP, whereas this was not the case in the previous two studies.1718 The reason for this discrepancy is unknown, but it might be due to the difference in the age range of the patients, since the ages of our patients ranged from 8 to 82 years, whereas in the previous studies they ranged from 24 to 66 years17 and from 24 to 67 years.18 Our study identified that an interval of <1.5 year from the onset to EBP application was a predictor of a positive response to the EBP, whereas the interval from the onset to diagnosis was not a predictor in a previous study.18 The result of our study suggests that applying an EBP within approximately 1.5 years of the onset could close a CSF leak. The median interval from the onset to EBP application in our study was 20 months, which was slightly long, probably because diagnoses of CSF volume depletion and CSF leakage are not well known, and so a relatively long time passed before patients suspected of CFS volume depletion were referred to our hospital. The mean interval of approximately 1.5 months from the onset to diagnosis in the previous study was much shorter than that in our study. This difference might have affected the ability to identify the interval as a predictor of a positive response to an EBP.
The limitations of this study include its retrospective design, the small number of patients with spinal CSF leakage, and the possibility of bias among the included patients. There were several differences in the responses to EBPs between spontaneous and traumatic CSF leaks, but the reasons for these differences are unclear. Further studies should be performed that are not affected by these limitations.
In conclusion, this study found that the significant predictors of a positive response to an EBP for CSF leakage were <1.5 years from the onset to EBP application, age <40 years, CSF OP <7 cm H2O, epidural CSF leakage in RI cisternography, epidural CSF collection in MRI, <20% RI remaining after 24 hours, orthostatic headache, nuchal pain, photophobia, and nausea. These 10 variables should be taken into account before making a decision to treat spinal CSF leakage.






 XML Download
XML Download