

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A schwannoma is a benign neoplasm of the nerve sheath derived from Schwann cells1. We present a rare case of schwannoma on the scalp that was difficult to diagnose despite various preoperative radiologic examinations.
CASE REPORT
A 47-year-old woman who visited our clinic presented with a 35-year history of a subcutaneous mass protruding from the left occipital scalp (Fig. 1A). She underwent surgical excision 35 years ago, and she remembered that the diagnosis was lipoma. The patient reported that she initially had no symptoms but started experiencing pain two years previously, which gradually worsened. The patient underwent ultrasonography and computed tomography (CT) of the brain at a local hospital. Multiple low echoic lesions were observed. The radiologist suggested that the tumor could be an epidermal cyst. Therefore, she was referred to our clinic for surgical removal. We received the patient's consent form about publishing all photographic materials.
We performed further radiologic examination using magnetic resonance imaging (MRI) before surgery. MRI revealed a heterogeneously enhancing mass with multilocular lesions extending to the posterior neck space. In addition, a heterogeneous hyperintense signal on T2-weighted images, isointense signal on T1-weighted images, and internal microhemorrhages were observed. The radiologist suggested that the tumor could be a type of vascular tumor, such as a vascular malformation.
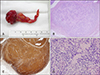
Because of these inconsistent preoperative radiologic findings, exploratory surgery was performed for accurate diagnosis and treatment. We made a zigzag incision on the scalp and elevated the flaps for sufficient visual field to remove the mass. We successfully excised the tumor (Fig. 1B, C). The specimen was a multilobulated mass of measuring 7.0×2.7×1.0 cm3. Histologic examinations revealed an encapsulated, well-circumscribed mass that included alternating hypercellular (Antoni A) and hypocellular (Antoni B) areas of myxoid stroma. Immunohistochemically, the lesion was positive for S-100 protein and vimentin and negative for epithelial membrane antigen and cluster of differentiation 34 (Fig. 2). Finally, the tumor was diagnosed as a schwannoma. After the surgery, the patient was free of pain and had no neurologic complications. In addition, the patient satisfied with cosmetic outcome since there was no conspicuous alopecia. There was no recurrence at 12 months follow-up (Fig. 1D).
DISCUSSION
A schwannoma is one of the most common benign nerve sheath tumors2. Reports have indicated that 25%~45% of extracranial schwannomas develop on the head and neck3. However, schwannoma development on the scalp is rare456. According to a study analyzing 22 patients with extracranial non-vestibular head and neck schwannomas, 76% were unilateral neck masses7.
A pathologic examination is the gold standard for diagnosing a schwannoma. However, a preoperative radiologic examination is helpful. According to the literature, the usefulness of CT is limited for schwannomas as it only correctly diagnosed 14% of cases8. In CT scans, schwannomas may show low to intermediate attenuated cystic masses; therefore, it cannot easily be differentiated from other common scalp cystic lesions. MRI is a more accurate imaging tool for schwannoma as 20 out of 25 cases (80%) were diagnosed as schwannoma8.
We retrospectively reviewed the MRI findings and found the following characteristic features of benign nerve sheath tumors that can also be seen in schwannomas (Fig. 3). First, “low signal margin” can be seen as a low signal rim surrounding the mass. It corresponds to the epineurium covering the schwannoma9. Second, “target sign” can be seen on T2-weighted images as a peripheral high signal rim and central low signal intensity within the mass. This pattern corresponded histologically to peripheral myxomatous and central fibrous tissues with high collagen content10. A previous report suggested that the target sign is more commonly seen in a neurofibroma (58%), which is also one of the common benign nerve sheath tumors, but can also be detected in a schwannoma (15%)11. Third, “entering-and-exiting-nerve sign” can be seen as a high signal situated longitudinally to a fusiform mass on T2-weighted images911. Finally, “fascicular sign” can be seen as multiple small ring-like structures within the lesion with peripheral higher signal intensity. Fascicular appearances are significantly suggestive of schwannomas (63%) than neurofibromas (25%)12. These features can be helpful clues in diagnosing schwannomas.
In South Korea as well as in other countries, dermatologists deal with various skin tumors, and cases of surgical treatments by dermatosurgeons increase. Therefore, it is necessary to make a proper diagnosis through preoperative clinical and radiologic examinations because it may influence treatment options or surgical methods. Clinical findings are often insufficient to distinguish schwannoma from other common tumors. Therefore, it is necessary for dermatosurgeons to understand the typical imaging findings of common scalp tumors. Commonly benign tumors of the scalp that require a differential diagnosis from schwannoma include epidermal cyst and lipoma. Differential clinical, histologic, and radiologic characteristics of schwannoma with epidermal cyst and lipoma are summarized in Table 1131415161718. Imaging studies can be helpful in the differentiation of benign tumors from malignant soft tissue tumors in head and neck areas such as liposarcoma, fibrosarcoma, malignant fibrous histiocytoma, rhabdomyosarcoma, etc. Large size (generally ≥5 cm), extracompartmental extension, poorly defined margins, broad interface with underlying fascia, intratumoral hemorrhage or necrosis, invasion of bone or neurovascular structures, heterogenoues MRI signal intensity, high signal intensity on T2-weighted MRI images and marked, primarily peripheral enhancement are suggestive imaging features of malignant soft tissue tumors in the head and neck1920.
The surgical approach of cutaneous schwannoma needs more consideration because complications such as neurologic deficits by peripheral nerve damage can develop. If neurologic complication of surgery is present, observation or partial removal is recommended. In our case, the patient did not report any neurologic complication after surgery.
Here, we report a rare case of scalp schwannoma with a review of MRI findings. Adequate understanding of characteristic MRI findings of schwannoma will be helpful for clinicians to diagnose and manage this tumor properly.



 XML Download
XML Download