

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Urticaria is a common disease affecting 15%~25% of the population with at least once in their lifetime1. Chronic urticaria (CU) is defined as spontaneous urticaria that lasts over six weeks without improvement2. It is important to distinguish acute and CU because they clearly show different pathophysiology, cause, and prognosis3. CU is a common disabling disorder occurring in 0.1% to 1% of the population, with an average duration of 3~5 years in adults45. In some patients, its duration exceeds 20 years67. CU can exert a considerable influence on the well-being of patients and it has a negative impact on the quality of life8.
Acute urticaria has treatable causes frequently. In contrast, it is difficult to identify the etiologic factors responsible for CU1. Recent diagnostic guidelines for CU have been recommended thorough history-taking and only a very limited amount of laboratory tests9. Most physicians agree laboratory tests such as complete blood count (CBC), chemistry panel, complement levels, and skin prick test or patch test are not that helpful for diagnosis or finding the etiologic factors. However, most clinicians conducted them routinely for the evaluation of CU, especially due to patient's will to find causes of CU2. Understanding of the natural course of CU is important for bringing precise knowledge to patients and preventing needless anxiety for patients. However, data on the natural history and prognostic variables of CU are scarce2.
The aim of this study involving CU patients was to investigate the natural course and prognosis of CU in a number of patients of CU in Korea.
MATERIALS AND METHODS
Patient selection
This study included Korean CU patients who attended the Department of Dermatology, Hallym University, Kangnam, Kangdong, and Hallym Sacred Heart Hospital between March 2008 and July 2015. The protocol was approved by the Institutional Review Board of Kangnam Sacred Heart Hospital (IRB no. 2016-01-04). The medical records of the 985 patients were evaluated initially. CU was defined as the presence of hives that disappear within 24 hours for more than 6 weeks. Only the patients who had had follow- ups more than 6 months after diagnosis were includeed. A total of 985 patients were contacted by telephone to inquire regarding their current disease status, such as CU persistence or remission. If a patient had been free of urticarial symptoms for at least 6 months without medication, he/she was considered to be in remission. We could trace 329 patients by telephone. All of the patients were reached by telephone by the second attempt. We gathered a detailed medical history including age, sex, past medical history and family history of urticaria and atopy (atopic dermatitis [AD], allergic rhinitis, asthma), duration of urticaria, accompanying symptoms, trigger or aggravating factors, severity and subtypes, method and response of treatment, and clinical courses using medical records. Severity of CU was determined by using the step 4 medication according to European Academy of Allergy and Clinical Immunology (EAACI)/Global Allergy and Asthma European Network (GA2LEN)/Électricité de France (EDF)/World Allergy Organization (WAO) 2009 guideline. It has four steps of treatment using oral medications and it is used in other studies done for predicting prognosis and when making the decision to treat CU patients10. Patients with mild CU were treated with antihistamines, whereas most patients with moderate to severe CU were on antihistamines most of the time and frequently needed short courses of corticosteroids. Dermographism, cold urticaria, cholinergic urticaria, and pressure urticaria were determined by history taking, physical examination and provocative tests. To evaluate dermographism, firm stroking of the skin was performed, inducing linear itchy wheals within minutes. The test for pressure urticaria was performed using sandbags joined by a rope each placed over one shoulder for 15 minutes, which resulted in a palpable wheal at the application site 2~8 hours later. Diagnosis of cold urticaria was made by application of an ice cube in a thin plastic bag to the skin of the forearm for 20 minutes, which caused whealing to occur within 15 minutes at the test site, upon rewarming the skin. For assessment of cholinergic urticaria, the patient was asked to run on the spot to the point of perspiration. A positive response was defined by subsequent pruritic erythematous punctuate whealing, within 5~15 minutes. Solar urticaria was diagnosed by a phototest and confirmed by exposure to natural sunlight.
Laboratory investigations
Most patients underwent the following laboratory work up: CBC, chemistry panel, and complement levels including complement (C) 3, C4, and the 50% haemolytic complement activity. Anti-nuclear antibody (ANA), thyroid function test (TFT), anti-thyroglobulin and thyroid microsomal antibodies, and total immunoglobulin E (IgE) were conducted in some patients.
Increased eosinophils were defined as over 500/mm2 and elevated total IgE was determined as over 100 IU/ml.
Statistical analysis
We used a Kaplan–Meier analysis with numbers at risk table to determine as a function of time the proportion completely cleared for the total group and subgroups. A log rank test was used to analyze the relationships between prognostic factors and the cumulative probability of complete remission of CU. The influence of the presence of AD on remission was evaluated by univariable Cox regression analyses.
The results were expressed as means±standard deviations. The chi-square test for nominal variables and the Student's t-test for continuous variables were used to determine the significance of differences. Significance levels for all analyses were set at p<0.05. All statistical analyses were conducted using PASW Statistics ver. 18.0 (IBM Corp., Armonk, NY, USA).
RESULTS
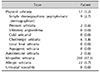
Patient characteristics (Table 1)
The response to the telephone interview was 33.40% (329 of 985 patients were traced). A total of 329 patients (144 male and 185 female) were evaluated, with an average age of 46.50 years (range, 9~87) and an onset age of 38.98 years (range, 1~87). The average duration of symptoms was 6.34 years and its range was 0.16~38 years. Personal history of atopy was reported in 153 patients (46.5%). The frequencies of AD, allergic rhinitis, and asthma were 7.0, 31.6, and 7.9%, respectively. Almost half of the patients accompanied dermographism (161 patients, 48.9%) and 29 patients (8.8%) showed angioedema. In all, 19 patients (5.8%) showed a family history of CU and a total of 31 patients (9.4%) had a family history of atopy. A large percentage of the patients mentioned that food or temperature change is related with their aggravated urticaria (15.0 and 10.2%) and some of them mentioned that factors such as psychological stress (4.1%) and fatigue (3.7%) aggravated their urticaria. In terms of severity, 236 patients (71.7%) were scored as mild CU using the step 1 and 2 medications, whereas 70 patients (21.3%) were scored as suffering from moderate CU, and prescribed the step 3 medication; 23 patients (7.0%) were scored as severe CU using the step 4 medication according to the EAACI/GA2LEN/EDF/WAO 2009 Guideline.
Duration, remission rate, and recurrence rate of CU
After telephone interviews, 39.2% of patients were resolved to be CU-negative. The mean duration of symptoms was 6.34 years (range, 0.16~38 years). Depending on the period, 10.8%, 18.8%, and 32.9% of the patients recovered in 1, 2, and 5 years, respectively. A 6.4% of patients reported that their CU recurred.
Types of CU (Table 2, Supplementary Table 11112131415)
Patients were divided by the type according to etiology (cause), such as idiopathic urticaria, allergic urticaria, cholinergic urticaria, pressure urticaria, and so on. Chronic idiopathic urticaria accounted for 87.5%.
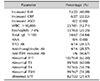
Laboratory analyses (Table 3)
Most patients presented a normal chemistry panel and CBC. In all, elevated erythrocyte sedimentation rate (erythrocyte sedimentation rate>20 mm/h) was found in 12 patients (12/25, 48.00%). C-reactive protein was elevated in 6 patients (6/27, 22.22%). White blood cells (WBC) were elevated in 23 patients (WBC >10,000, 23/181, 12.71%). Thirty-three patients had eosinophilia (Eosinophils >4%, 33/163, 20.25%), and 34 patients had elevated total IgE level (total IgE >100 IU/ml, 34/62, 54.84%). A test for ANA was performed only for 4 patients and none of them had abnormalities. Over half of the patients showed abnormalities in a TFT, including abnormal T3, T4, and thyroid stimulating hormone (TSH). However, positive results for thyroid peroxidase (TPO) antibody (Ab), anti-thyroglobulin Ab, and anti-TSH receptor Ab were found in 4, 4, and 1 patient, respectively (4/14, 28.57%; 4/14, 28.57%; 1/6, 16.67%).
The association of CU remission with clinical characteristics and laboratory findings (Table 4, 5)
A total of 329 patients were evaluated for the duration of symptoms with a Kaplan–Meier analysis; 10.8%, 18.8%, and 32.9% of the patients recovered in 12, 24, and 60 months, respectively. The same analysis was performed concerning gender, age groups (<18 years and ≥18 years, <60 years and ≥60 years), and the severity and subtype of CU (Fig. 1A~F).
The median recovery time was 11.0 months for females and 24.0 months for males (p=0.098). The median recovery times for the patients with CU and <18 years of age compared to those with CU and ≥18 years of age were 6.1 and 17.3 months, respectively (p=0.929). The median recovery times for the patients with CU and <60 years of age and those with CU and ≥60 years of age were 11.3 and 19.9 months, respectively (p=0.879). There were no differences in prognosis and remission rate with respect to the severity of CU (p=0.489) and the type of CU (p=0.662). The median recovery times for the patients with dermographism compared to those without it were 11.3 and 13.7 months, respectively (Fig. 2A, p=0.368). The presence of angioedema was found in association with CU severity (Table 6, p=0.030), however it was not significantly associated with CU duration (Fig. 2B, p=0.573).
The median recovery time was 22.3 months for patients with a history of AD and 16.4 months for patients without it. The presence of AD showed significant differences (p=0.026, Fig. 3A). Regarding AD, the relative hazard ratio (0.036) (95% CI 0.127~0.931, p=0.036) using Cox's proportional hazards model. The median recovery times for the patients with a personal history of allergic rhinitis and those without it were 9.0 and 14.0 months, respectively (Fig. 3B, p=0.177). In the case of asthma, each result was 13.7 and 12.0 months (Fig. 3C, p=0.791). The median recovery time of CU were not significantly different according to eosinophil count, total IgE, and WBC count (p=0.764, p=0.734, and p=0.421, respectively; Fig. 4A~C).
DISCUSSION
We determined the natural history and prognostic factors of CU in Korean patients. In our study, 10.8%, 18.8%, and 32.9% of the patients recovered in 1, 2, and 5 years after the onset of CU, respectively. The mean duration of CU was 6.3 years. The presence of AD was significantly associated with a poor CU prognosis. The coexistence of angioedema was significantly related to CU severity. Reported studies of the natural history of CU found that 30%~80% patients recovered 1 to 5 years after the onset of symptom259161718192021. Humphreys and Hunter reported that symptoms were present for more than 5 years in 5% of patients in the UK16. Quaranta et al.17 investigated 86 patients with chronic idiopathic urticaria among whom 27 patients (31%) resolved, 48 patients (56%) continued to have symptoms, and 11 patients (13%) had unknown natural cause, after a 3-year period in the U.S.A.5. Toubi et al.5 reported CU lasted over 1 year in more than 70% of patients in Israel. In a follow-up after 3 months, 43% of patients were still suffering from CU, and at around 96 months, 14% of patients were still suffering from it. In Sweden, among 330 adult patients with CU, the median duration of the symptoms was between 2 and 4 years18. In another adult study with 153 patients in the Netherlands, the recovery rates were 34% and 49% for 5 and 10 years, respectively2. In Korea, Kim et al.22 reported that the mean duration of CU was 3.76 years in 641 adults. Kang and Shin3 found a remission rate of CU within 1 year of disease onset was 84.8% in Korean children with CU. Park et al.23 found that 33.4%, 53.0%, and 71.2% of Korean children with CU recovered within 6, 12, and 24 months of disease onset. Our findings were that 10.8%, 18.8%, and 32.9% of Korean patients with CU were in remission at 1, 2, and 5 years, respectively. The previously published studies showed variable results with natural history of CU. This might be because the race and the study population are different. Results on the natural history of CU are inevitably influenced by the make-up of the study population2. Additionally, the justification of CU remission may be different, depending on the studies.
Until now, many studies have tried to identify predictors of CU prognosis. In the study of van der Valk et al.2, the severity and duration of disease at the first visit proved to be important prognostic factors. Patients with severe disease and longer lasting diseases have a worse prognosis compared with patients with milder disease2. Regarding types of urticaria, dermographism showed the best prognosis and cold urticaria the worst. The presence of angioedema did not significantly affect differences in prognosis2. In our study, there were no differences in remission rate with respect to the presence of angioedem (p=0.573), the severity of CU (p=0.489), and the type of CU (p=0.662). However, angioedema was found to be associated with CU severity (p=0.030).
CU often is associated with multiple disorders, such as atopy, infection, autoimmune diseases, neoplastic disorders, and metabolic diseases2425. In our study, the personal history of AD was confirmed as a predictable factor for the prognosis of CU. Patients with a history of AD showed a worse prognosis in CU than those without it. The median recovery time depending on the history of allergic rhinitis or asthma showed no significant difference. In previous studies, CU was strongly associated with the history of childhood eczema2426. In study among more than 4,000 children up to 2 years of age with AD, urticaria was most common concomitant disease27. In addition to high prevalence and coincidence, probable common or similar pathogenesis could be involved25. Ye et al focused on the shared cutaneous features of chronic idiopathic urticaria (CIU) and AD19. Severe pruritus, perivascular inflammatory infiltration, and epidermal involvement were observed in two common skin diseases19.
In our study, 7.9% (26/329 patients) of the subjects were elderly (≥60 years of age). A previous Korean study reported 4.5% were elderly in the 837 patients with CU4 From 1598 patients with CU in Israel, there were 9.4% elderly subjects (elderly CIU group)28. Magen et al.28 suggested that despite the small percentage of CU patients defined as elderly, it is important to identify the specific clinical features of this group due to the aging of the population. CU in the elderly population is characterized by fewer wheals, lower rates of concomitant symptomatic dermographism, lower rates of angioedema, and lower autologous serum skin test (ASST) positivity28. However, Ban et al.4 reported CU disease activity and severity were not significantly different between the elderly and nonelderly. Our study also showed that elderly CU patients did not display any differences in prognosis.
According to classification based on etiologic factors, almost all of our patients had chronic idiopathic urticaria (87.5%) or allergic urticaria (6.7%) and the others were relatively rare. In particular, the number of physical urticaria or autoimmune urticaria cases is low, likely because detecting them with detailed questions and provocation tests in the clinic was difficult92129.
The following aggravating factors were mentioned in our study by patients: food (15.0%), temperature change (10.2%), psychological stress (4.1%), fatigue (3.7%), and others (exercise, drugs, pressure, and unknown). According to a systematic review, aggravating factors mentioned by patients in questionnaires were stress (16%~40%), pressure on the skin/dermographism (13%~52%), heat (23%~31%), exercise (15%~22%), analgetic drugs (8%~15%), coldness (13%), and consumption of alcohol (4%~9%)30. Our results were consistent with previous reports of worldwide CU groups3132, and food comprised a large proportion of aggravating factors in Korea.
There were some limitations in our study. This study may not be comparable with studies involving patients visiting a general practitioner or a dermatology unit in a general hospital because patients who visited university hospitals, and thus who might have a very refractory progress of CU were included. Also, laboratory tests such as ASST and multiple allergen simultaneous test were not done for all patients and a small number of test results were positive.
In conclusion, spontaneous remission occurs in 10.3%, 21.2%, and 32.6% of Korean patients with CU within 1 year, 2 years, and 5 years, respectively. A personal history of AD was found to be associated with CU remission. The presence of angioedema was significantly related to CU severity. However, clinical parameters such as severity, dermographism or angioedema, and laboratory parameters such as eosinophil percentage or total IgE levels did not significantly affect the remission of CU. Informing the patients about their prognosis and the natural history of CU based on these results may be helpful.








 XML Download
XML Download