

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Of the various methods for recovering damaged areas due to tooth loss, implant treatment has become standard in the field of dentistry. The concept of implant osseointegration was introduced by Brånemark in 1952, and dental implant treatment became common in fully and partly edentulous patients in 1965.1 In 1978, it spread globally through the Toronto Convention, and the fields of application have rapidly increased since then. Implant treatment was previously aimed at the recovery of masticatory function, but, with the more recent emphasis on aesthetic recovery, patient satisfaction with implants is similar to that with natural teeth.23
For the long-term success of the implant, the biological reaction occurring between the implant fixture and the bone during healing and the biomechanical bite force delivered to the surrounding bones through the prosthesis should be considered.4 The various causes of implant failure include mechanical problems, such as loosening and fracture of abutment screws and prosthesis and abutment fracture due to metal fatigue;5678910 and biological problems such as plaque accumulation, osseointegration loss, and osteolysis.11121314 In general, after implant placement, osseointegration increases over time; however, if bony tissues are weak, osteogenesis of the implant interface is reduced, occasionally leading to osseointegration failure. In such cases, when the prosthesis is installed, osseointegration interface separation may occur due to torsion force by tightening torque and loosening torque.15
The clinical survival rate of the implant strongly correlates with stability after insertion. The stability of the implant is assessed by various methods. Typically, the stability is assessed through a biomechanical analysis with hard tissue interface and an interface histological analysis with soft and hard tissues. Biomechanical analysis with hard tissue interface is mainly conducted through physical means. Percussion reaction testing16 is a simple method that involves hitting the top of an implant with a metal object and listening to vibration sound; the results cannot be quantified and it is difficult to detect decrement of sound quality or amplified resonant frequency. Tooth mobility measurement [Periotest (Siemens AG, Benssheim, Germany)] and Dental Fine Tester17 use an exclusive handpiece; the reliability of the measured value decreases according to the positions of the abutment and handpiece. The reverse torque test161819 detects abnormalities by applying counterclockwise torque at 20 Ncm to the implant. This is effective for detecting implant osseointegration failure but causes irreversible deformation in juveniles. Measurements of cutting force, insertion torque, and cutting resistance on insertion16 do not harm the area of implant placement but assessing bony tissues only on insertion has the disadvantage of being difficult to reproduce. Resonance frequency analysis202122 is nondestructive testing of the relationship between the implant and the surrounding bone using electrical vibration. It has a high degree of reproducibility and reliability, but the equipment is expensive and the prosthesis should be removed.
Interface histological analysis with soft and hard tissues is conducted through various imaging methods. Radiologic examination172324 is commonly used, but standardization is difficult and the limitation of 2D interpretation is a disadvantage. Micro-CT can be used to obtain 3D images of the implant and bone interface, but the examinee is exposed to radioactivity. Histological and histomorphometric analyses are quantitative methods for testing the bones and implants, allowing simultaneous observation of the implant and the surrounding soft and hard tissues; however, as destructive tests, they have limited clinical utility. The pull-out and push-out test162526 has been used for measuring the shear bond strength of the cylinder-type implant, and the degree of micro-level implant osseointegration can be quantified as biomechanical bond strength.
To investigate the stability of the connection between implant fixture and abutment, various methods for measuring the loosening torque of an abutment screw have been introduced. Loosening torque, one of the indicators of joint stability, is a measure of the full load remaining immediately before loosening of the abutment screw, affected by the fitness of the implant prosthesis.27 Elshahawy et al.28 measured the turning force of the loosening of the abutment screw, and Faulkner et al.29 used the Periotest for this purpose. Haack et al.30 measured the full load through the transformation of the screw length, comparing the initial length of the abutment screw and its length after loosening. In addition, Martin et al.31 used a strain gauge to measure full load and loosening torque. Gross et al.32 obtained the value of loosening torque by measuring microleakage of dye at the part of the connection between the abutment and the fixture. This method is simple and appropriate for clinical use, but there was a problem of result distortion due to temperature or corrosion.
The loosening torque can be measured using a torque driver and torque gauge. The devices that apply tightening torque and loosening torque to the implant abutment screw are divided broadly into two types: manual and electronic. The manual devices are further classified as torque wrenches or torque drivers. The existing manual torque wrenches developed by implant companies include a torque-limiting device and a torque-indicating device. The torque-limiting device breaks the handle head component if the input torque value exceeds a critical level. The torque-indicating device has a part in which a graduated arc is marked, which can control the size of the tightening force during use. Manual torque drivers include various forms and methods; for example, a contra-angle torque device has a device that can control the tightening force in the existing contra-angle handpiece.33
Manual torque drivers are mainly used in the early tightening process, and experienced clinicians are able to apply appropriate torque values; however, because it is prone to error due to the problem of uniformity according to the user,3435 it is not recommended for use in the final abutment screw tightening.36373839 On the other hand, the electronic torque driver effectively provides even torque, so it has the advantage of not being affected by the environment of use.4041 Recently, keeping pace with technological advances in dentistry, manufacturers have developed new electronic torque drivers, and the demand is increasing. With the electronic torque driver, the torque value the practitioner wants is evenly applied to the abutment screw in a digital format, and the torque value can be checked through the LCD screen. Its accuracy and convenience are better than those of the manual devices.
This study was aimed to evaluate the loosening torque that may affect the implant fixture. In this manner, the torque delivered to the implant fixture can be checked when the abutment screw is loosened at the torque recommended by the manufacturer. There are many previous studies that measured loosening torque and removal torque,42434445464748 but few studies have measured the delivery of the loosening torque applied to the abutment screw to the implant fixture in vitro. The measurement of the loosening torque of the general torque driver can be done as follows: Tightening is performed, and the abutment screw fastened to the implant fixture with the torque driver tip fixed on the torque gauge is manually rotated to measure the loosening torque. However, in this study, the loosening torque was directly applied to the abutment screw fastened to the implant fixture with an electronic torque driver and the torsion force affecting the implant fixture was checked, simultaneously measuring the torque delivered to the implant fixture with a digital torque gauge.
This study was aimed to quantify the torsion force delivered to an implant fixture when an abutment screw is removed through the method of measuring the loosening torque with high reliability in a biomechanical analysis with vital hard tissue interface, using three kinds of electronic torque drivers (W&H, SAESHIN, and NSK) and a digital torque meter (Mark-10, Inc.). The general method of measuring the removal torque49505152535455565758 reflects the degree of osseointegration according to the general characteristics of the implant; however, this study was conducted without calculating interface shear strength, using the same implant system for the three kinds of electronic torque driver.
This objective of this study was to evaluate the loosening torque that may affect the implant fixture and to assess the accuracy of different electronic torque drivers (W&H, SAESHIN, and NSK). The null hypothesis of this study was that there would be no difference in the measured value of torque delivered to the implant fixture when the abutment screw is loosened, among three kinds of electronic torque driver.
MATERIALS AND METHODS
Fig. 1 shows the overall overview of this study. Three kinds of electronic torque driver systems were used: W&H (IA-400, W&H Co. Ltd., Burmoos, Austria), SAESHIN (TRAUS-MCE30NN, SAESHIN Inc., Daegu, Republic of Korea), and NSK (ISD-900, NSK Co., Tokyo, Japan) (Fig. 2); and a digital-type torque meter: MGT12 (MARK-10. Inc., Copiague, NY, USA) (Fig. 3). Using the fixture and abutment kit (AnyOne, MegaGen, Daegu, Republic of Korea), a uniform implant system allowed objective, quantitative comparison of the numerical data obtained using the three different electronic torque drivers.
A jig that could fix an electronic torque driver and a digital torque meter in the exact location was used (Fig. 3). A total of 27 implant fixtures, abutments, screws, and torque driver tips were used in the experiment. In the MGT12, an implant fixture is fixed with a 3-jaw chuck, and the driver tip of the electronic torque driver is fastened into the hexagonal furrow at the top of the abutment screw to adjust axes X, Y, and Z of the jig. At the same time, the electronic torque driver is fixed by the exclusive holder (Fig. 3, Fig. 4). If the joint between the implant fixture and the electronic torque driver accurately align, the abutment screw can be tightened or loosened.
Tightening torque was applied two times and loosening torque was applied one time. The tightening torques of all the electronic torque drivers were 15 Ncm, 25 Ncm, and 35 Ncm. The calibration of drivers was made for the accuracy of an electronic torque driver, and the trueness and repetitive reproducibility of the tightening torque values were tested by using a digital torque gauge. After fastening, the initial tightening torque was applied and after 10 minutes, the same tightening torque was applied; five minutes later, the loosening torque was applied. This process was repeated 10 times per specimen and the loosening torque measurements were recorded, for a total of 270 repetitions (30 times per torques [15, 25, and 35 Ncm] and 90 per electronic torque drivers [NSK, W&H, SAESHIN]) (Fig. 1). A new screw was used for each measurement. All processes of this experiment were conducted by the same investigator (K.S.).
The loosening torque can be measured by digital torque meter, as in Fig. 4. As shown in Fig. 4, if the MGT12 fixes the implant fixture, the 3-jaw chuck is the part where the load is generated when the loosening torque is applied after applying the tightening torque. In this setting, the force applied to the MGT12 is not solely the force applied to the abutment screw; rather, it is the delivered force passing through the implant fixture. From a clinical perspective, the 3-jaw chuck of MGT12 is analogous to the alveolar bone connected to the implant fixture, and the loosening torque applied in this manner can be defined as the stability of osseointegration (that is, the torque delivered to the implant fixture combined with the alveolar bone). From a physical perspective, the loosening torque of the abutment screw generated by the electronic torque driver is larger than the torsion force as energy is lost in the process of delivery to the implant fixture, but the amount of energy lost is negligible, so the loosening torque and torsion force were considered the same.
All statistical processes were analyzed using SPSS for Windows 23.0 (SPSS Inc., Chicago, IL, USA). First, the normal distribution of the data was examined through the Shapiro-Wilk test. For the loosening torque of all electronic torque drivers, the one-way ANOVA (α = .05) was performed if there was a homogeneity of the variances and the Tukey test was conducted post hoc. If there was no homogeneity of the variances, the Kruskal-Wallis test was performed and a pairwise test was conducted post hoc.
RESULTS
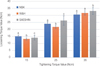
Table 1 and Fig. 5 show the results of loosening torque of different electronic torque drivers. There were statistically significant differences in target torque among the three kinds of electronic torque driver (P < .001). The values obtained with the W&H are significantly decreased compared to all target torques. Overall, there were significant differences among the three kinds of drivers at the target torques of 15 Ncm and 25 Ncm. In the system comparisons, the measured value was closest to the target torque in the following order: NSK > SAESHIN > W&H (P < .05). At the target torque of 35 Ncm, the SAESHIN driver (33.1 ± 2.4 Ncm) showed the closest measured value, while there was no significant difference between the NSK (30.6 ± 1.3 Ncm) and W&H driver (31.7 ± 1.6 Ncm) (P > .05).
DISCUSSION
This study applied tightening torque to a screw fastened to an implant fixture with three kinds of electronic torque drivers at the target torque values of 15 Ncm, 25 Ncm, and 35 Ncm, then applied the loosening torque accordingly, and measured the final delivered torque between the implant fixture and the MGT12 device. The torque measured in this experiment was delivered to the test components in the following order: abutment screw → implant fixture → MGT12. This is clinically equivalent to the loosening torque of the electronic torque driver delivered in the following order: abutment screw → implant fixture→ alveolar bone, thereby affecting the osseointegration of the implant fixture with the alveolar bone. In the study published by T. Paepoemsin et al.,49 it was reported that the force of the removal torque was approximately 80% – 90% of the tightening torque recommended by each manufacturer. In our study, the torque delivered to the implant fixture was delivered at the level of approximately 93.7% of the loosening torque.
The results of this study show the feasibility of the method for checking the impact on the implant fixture when the loosening torque is applied to the abutment screw tightened at the target torque. In an in vitro test conducted by Stüker et al.,50 for the tightening torque at 30.07 ± 0.28 Ncm, the removal torque was up to 18.75 ± 1.89 Ncm. Further, in an in vitro study conducted by Ghanbarzadeh et al.,51 for a one-piece abutment type, the removal torques were 20.25 ± 4.46 Ncm and 13.16 ± 2.18 Ncm for the tightening torques of 28.8 ± 4.61 Ncm and 16.8 ± 1.73 Ncm, respectively. Meanwhile, in an in vitro test conducted by Saliba et al.,52 for the tightening torque of 32 Ncm, the removal torque was as high as 38.62 ± 6.43 Ncm. As shown in Table 1, except for the removal torque result as high as 26.3 ± 3.4 Ncm for the tightening torque at 25 Ncm with the SAESHIN electronic torque driver, all had loosening torques lower than the tightening torque.
The tightening torque affects the loosening torque, and the loosening torque is finally delivered to the osseointegration site as a torque between the implant fixture and the alveolar bone. In animal testing using rabbits conducted by Hwang et al.,53 there was a difference in the removal torque according to the time of implant fixture insertion, and the removal torque measured at week 5 was approximately 16.06 ± 6.17 Ncm. In the study reported by Koh et al.,54 when the removal torque was measured on implant fixtures in mongrel dogs, the removal torque was 71.2 ± 2.5 Ncm at week 12, which was the highest value. In animal testing using mice conducted by Yi et al.,55 the removal torque was 30 Ncm at week 2 and 70 Ncm at week 6. Buser et al.56 measured the removal torque of Osseotite implants at weeks 4 and 12, and the values were 62.6 Ncm and 95.7 Ncm, respectively. The longer the implant healing period, the higher the level of osseointegration becomes; therefore, in the early phase, when the removal torque is similar to or lower than the applied abutment tightening torque, it is necessary to pay close attention when loosening the abutment screw. In addition, because osseointegration is poor in some individuals, it is necessary to take precautions, for example, by increasing the healing period, increasing the coherence, or reapplying the tightening torque. Even if the removal torque between the implant fixture and the alveolar bone is higher than the loosening torque, the loosening torque is an element in contrast to the removal torque, so it may have a direct impact on osseointegration. Thus, it is advisable to reduce the frequency of loosening torque addition.
According to results of this study, the tightening torque and loosening torque did show a slight difference (Table 1). The differences in target torques of 15 Ncm were 0.1, −1.8, and −0.9 Ncm in NSK, W&H, and SAESHIN, respectively. The differences in 25 Ncm were −1, −3.2, and 1.3 Ncm in NSK, W&H, and SAESHIN, respectively. The differences in 35 Ncm were −4.4, −3.3, and −1.9 Ncm in NSK, W&H, and SAESHIN, respectively. At most difference values, the loosening torque was lower than the target torque (tightening torque). Previous study evaluating the accuracy of tightening torques in torque-limiting devices showed lower tightening torques (mean difference of −1.7 to −9.9 Ncm) relative to target torque in all 5 type of torque-limiting devices.57 Therefore, the lower tightening torque compared to the target torque may cause the lower loosening torque. Low loosening torque can affect stability over time in the oral cavity.57 Therefore, calibration according to the manufacturer's manual is required for accurate tightening torque.58 Further study is needed on how low tightening torque affects loosening torque.
The present study has a number of limitations. First, the loosening torque was measured by referring to the torque setting on the electronic torque driver as the target torque without actually measuring the tightening torque. The instrument was calibrated before the experiment, but its use in previous studies may cause low tightening torques,57 so further research is needed. Second, the loosening torque was measured by fixing the implant fixture to a 3-jaw chuck on the digital torque gauge. Different results can be obtained with implant fixtures placed in the bone in the oral cavity. Finally, it has not been tested in oral conditions. Many intraoral conditions (functional load, humidity, and temperature) cause the screw to loosen.5960 Therefore, the loosening torque before applying the oral condition in this study should be regarded as a relatively high loosening torque. Therefore, further studies require results evaluated under oral conditions.
CONCLUSION
Within the limitations of this in vitro study, all three electronic torque drivers had significant differences in loosening torque values (P < .001). The tightening torque and loosening torque did show a slight difference, and most of the loosening torque was lower than the tightening torque. The most accurate loosening torques showed SAESHIN (33.1 ± 2.4 Ncm) at 35 Ncm, and NSK (15.1 ± 0.9 Ncm and 24.0 ± 1.4 Ncm) at 15 Ncm and 25 Ncm. Since the loosening torque may vary depending on the tightening torques and electronic torque drivers, periodic calibration of the electronic torque driver is recommended.





 XML Download
XML Download