

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hypoxemia is occasionally observed in patients with chronic obstructive pulmonary disease (COPD), and it generally worsens as the disease progresses.1 Oxygen therapy is crucial to hypoxic COPD patients. Long-term oxygen therapy (LTOT), defined as supplemental oxygen use for over 15 hr/day, prolongs survival in COPD patients with severe resting hypoxemia.23 LTOT also improves exercise capacity,4 neuropsychiatric function,5 health-related quality of life (HRQoL),6 and pulmonary hemodynamics.7
As home oxygen therapy has become more common, many countries have developed strategies to facilitate its appropriate utilization to maximize its benefits. In the United Kingdom, the British Thoracic Society released guidelines for home oxygen therapy, which contains the indications or restrictions on various modalities of home oxygen therapy as well as guiding the follow-up of patients on oxygen therapy.8 Oxygen registries have been established in Sweden and Denmark for improving the overall quality of LTOT. Since 1987, Swedish LTOT users have been registered in the Swedish National Register of Respiratory Failure, which provides prospective clinical and research data. Using this registry, the national structure for the prescription and management of LTOT have been evaluated.9 Establishment of the Danish Oxygen Register improved survival as well as adherence to LTOT guidelines. It also helped equip more patients with an oxygen concentrator and mobile oxygen, facilitating continuous oxygen use.10 The French government recommended oxygen prescriptions to meet the patient's needs rather than providing oxygen therapy uniformly. This led to increased use of portable oxygen concentrators and decreased use of liquid oxygen tanks, leading to reduced costs for the health care system.11
Despite these efforts, patients still feel that the lack of a patient-centered approach is one of the barriers to optimal oxygen therapy administration. Therefore, strategies must be developed for prescribing appropriate home oxygen therapy to meet individual patients' clinical and lifestyle needs.1213
In Korea, home oxygen therapy has been covered by national health care insurance since 2006. However, adequate management strategies for home oxygen therapy are not well established. This study aimed to explore the current situation of home oxygen therapy and to provide basic data for developing appropriate strategies for managing COPD patients using home oxygen therapy in Korea.
METHODS
Patients and procedures
In this cross-sectional study, we targeted COPD patients using home oxygen therapy. The inclusion criteria were as follows: 1) age > 18 years, 2) diagnosis of COPD according to Global Initiative for Chronic Obstructive Lung Disease guideline,14 3) using home oxygen therapy for at least 1 month, and 4) meeting the indication of home oxygen therapy in Korea (arterial partial oxygen pressure [PaO2] ≤ 55 mmHg or PaO2 ≤ 59 mmHg in the presence of cor pulmonale and/or secondary polycythemia. The exclusion criteria were as follows: 1) disagree with enrollment, 2) using home oxygen therapy for other respiratory diseases mimicking COPD such as bronchiectasis, asthma, and tuberculosis-destroyed lungs, and 3) patients who were in exacerbation state. After patients provided informed consent, face-to-face interviews were conducted by a well-trained interviewer administering a structured questionnaire.
Questionnaire
The questionnaire consisted of four parts. The first part assessed clinical characteristics and HRQoL; it queried gender, age, height, weight, smoking history, comorbidities, grade of respiratory impairment,15 and supportive care from family or other people. The severity of dyspnea was assessed using the modified Medical Research Council (mMRC) scale. HRQoL was evaluated by both the COPD Assessment Test (CAT) score and the EuroQol-5D (EQ-5D), with three levels of severity for each of the five dimensions. The EQ-5D index is a continuous variable wherein 1 represents the best health status, and 0 represent death.16 Severity of respiratory impairment is categorized into three group according to airway limitation. The FEV1 of grade 1 was ≤ 25%, grade 2 was ≤ 30%, and grade 3 was 40% of predicted value, respectively.15 The second part assessed socioeconomic characteristics, including family structure, family function assessed by the family Adaptation, Partnership, Growth, Affection, Resolve (APGAR) score,17 marital status, level of education, monthly income, and financial support. The family APGAR score consists of five closed-ended questions about adaptation, partnership, growth, affection, and resolve. Respondents should select one of three options for each question, which are each scored differently. Total scores of 7 to 10, 4 to 6, and 0 to 3 suggest a highly functional family, a moderately dysfunctional family, and a severely dysfunctional family, respectively.17 The third part of the questionnaire evaluated patterns of home oxygen use; it queried oxygen flow rate, duration of oxygen use, and ambulatory oxygen use. The fourth section evaluated health care utilization, with items querying hospital visit and admission frequency, frequency of emergency room visits, and health care expenditures.
Statistical analyses
All data herein are expressed as arithmetic mean ± standard deviation (SD), where appropriate. Data analysis and descriptive statistics were conducted using SPSS Statistics, version 22.0 (IBM Corp., Armonk, NY, USA). Student's t-test was used to compare continuous variables such as clinical characteristics according to gender. Also, it was used to compare the number of health care utilization and the mean values of variables that might be associated with exercise according to whether the patients use oxygen during exercise or not. Pearson's χ2 test was used for categorical data. It was used in comparison of the number of patients who used health care utilization. Kolmogorov-Smirnov test was used to evaluate the normality of distribution and Mann-Whitney test was used to compare the median values in two groups that were not normally distributed. EQ-5D index was calculated using a formula that used time trade-off method and was proposed for Korean population.16 Results were considered statistically significant if P < 0.05.
RESULTS
Patient characteristics and HRQoL
Although we first asked for consent from 224 patients to enroll in this study, 27 patients refused to answer the questionnaire and 2 patients were excluded because they used home oxygen therapy less than one month. Finally, a total of 195 patients were enrolled in this study, and the demographic and clinical characteristics of the study patients are provided in Table 1. The mean age was 72.6 ± 9.7 years, and 76.4% were men. The age distribution was as follows: 18 patients (9.2%) were under 60 years old, 50 patients (25.6%) were in their sixties, 78 (40.0%) were in their seventies, and 49 (25.1%) were at least 80 years old. 73.8% of patients had history of smoking and all of them were ex-smokers. In terms of comorbidities, essential hypertension (41.0%) was the most common disease, followed by benign prostate hyperplasia (27.2%) and diabetes mellitus without complications (10.8%). Respiratory impairment was diagnosed in 70.3% of the patients.15 The number of grade 1 respiratory impairment was 48 (24.6%), grade 2 was 46 (23.6%), and grade 3 was 43 (22.1%).
Table 1
Clinical and sociodemographic characteristics and health-related quality of life

Data are presented as mean ± standard deviation or number (%).
BMI = body mass index, APGAR = adaptation, partnership, growth, affection, resolve, mMRC = modified medical research council, CAT = chronic obstructive pulmonary disease assessment test, EQ-5D = EuroQol-5D, USD = United States dollar.
aIncludes ex-smokers and current smokers; a smoker is defined as a person who has smoked at least 100 cigarettes in his or her lifetime; bCalculated among ex-smokers and current smokers; cRespiratory impairment grading according to The Act on Welfare of Persons with Disabilities.15
![]()
The mean mMRC was 3.4 ± 0.8, and more than half of the patients (54.4%) had an mMRC score of 4. The mean CAT score was 29.7 ± 6.8. According to the mMRC and CAT, respectively, 97.4% and 99.0% of the COPD patients were dyspneic and symptomatic.14 The overall mean EQ-5D index score was 0.35 ± 0.44 – 0.37 ± 0.43 for men and 0.27 ± 0.46 for women. Less than 10% of the participants were capable of walking (8.7%) and usual activity (7.2%).
Socioeconomic characteristics
The most common family structure was a two-member household shared by a couple (43.6%), and 72.3% of patients were married. 87.7% of the patients had caregivers. Family function was assessed by family APGAR score, and 82.5% of patients' families had family APGAR scores of 7 or more, indicating a highly functional family.17 In terms of education, 52.3% of the patients received junior high school education only. Regarding salary, over half of the patients' (59.0%) monthly income was less than USD 900. However, only 39.5% of patients received financial support from their children or relatives.
Patterns of home oxygen therapy usage
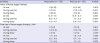
Table 2 summarizes the characteristics of home oxygen therapy. The mean duration of home oxygen therapy was 45.9 months. Patients were prescribed oxygen for means of 12.5 hr/day, 6.6 hr/day, and 8.2 hr/day at rest, during exercise, and during sleep, respectively. The mean values reflecting actual daily hours of oxygen use at rest, during exercise, and during sleep were 12.9, 1.1, and 6.6, respectively. The mean prescribed amounts of oxygen were 1.7 L/min, 2.0 L/min, and 1.7 L/min at rest, during exercise, and during sleep, respectively. The mean amounts of oxygen in actual use were 1.8 L/min, 0.7 L/min, and 1.7 L/min at rest, during exercise, and during sleep, respectively.
Table 2
Patterns of home oxygen therapy usage
![]()
Fig. 1 shows the prescription details regarding oxygen duration and real use at rest and during exercise. Although both mean values were similar, there was a difference in distribution between daily hours of prescription and actual use at rest. Only 32.3% of the patients were prescribed more than 15 hr/day of oxygen, and 54.3% of patients used home oxygen for less than 15 hr/day.

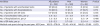
During exercise, 65.6% of patients did not use oxygen at all. mMRC and CAT scores were higher in patients who did not use oxygen during exercise. Additionally, the mean EQ-5D index was higher among patients who used oxygen during exercise (Table 3). After home oxygen therapy, 57.9% of patients felt that their health status improved.
Table 3
Comparison of respiratory symptoms and health-related quality of life according to oxygen use during exercise

Data are presented as mean ± standard deviation.
mMRC = modified medical research council, CAT = chronic obstructive pulmonary disease assessment test, EQ-5D = EuroQol-5D.
![]()
We also asked the patients whether they used ambulatory oxygen or not. 25.6% of patients responded in the affirmative. The main reason for not using ambulatory oxygen was insufficient finances (57.9%). The majority of patients (81.0%) were willing to use ambulatory oxygen therapy if it could be covered by health insurance.
Health care utilization
A total of 62.6% of patients had unscheduled hospital visits due to exacerbations of respiratory symptoms in the previous year (Table 4). The mean number of unscheduled visits was 2.9. Moreover, almost all the patients with unscheduled visits (118/122) experienced hospitalization. The mean number of hospitalizations and emergency room visits were 2.5 and 2.6, respectively. The mean medical cost for COPD was about USD 170/mon/patient.
Table 4
Health care utilization during the previous year
Data are presented as number (%) or mean ± standard deviation.
ER = emergency room.
a1 USD = 1,160 KRW.
![]()
DISCUSSION
This study showed the patterns of home oxygen use among Korean COPD patients on LTOT as well as their clinical and socioeconomic characteristics.
In this study, the proportion of men was about three fold more than that of women. Although the difference of prevalence according to gender is diminishing, prevalence of COPD was still higher in men at the time we collected the data.18 Difference of prevalence could be reflected in this study.
We evaluated the HRQoL of patients using the EQ-5D index. The mean EQ-5D index was 0.35, and this figure was worse than that of the general population in Korea whose EQ-5D index was 0.94.19 Few studies have evaluated HRQoL assessed by the EQ-5D targeting COPD patients on home oxygen therapy. Respiratory impairment was present in 70.3% of patients in this study which required FEV1 would be ≤ 40% of predicted at least.14 Thus, we compared the results of this study with those of other studies on severe and very severe COPD. We found that the overall HRQoL in the present study was worse than that reported by other studies, which found EQ-5D index ranging between 0.5 and 0.8.2021222324 Similarly, the mean CAT score in our study was worse than that of other investigations of severe COPD patients.2122 These results provide insights into the severity of symptoms and HRQoL among COPD patients on home oxygen therapy.
The family APGAR score was used to evaluate family functioning when the family was involved in patient care. In this study, 82.5% of patients' families had family APGAR scores of 7 or more, meaning that they had highly functional families. Taking care of COPD patients has been reported as a moderate burden for family caregivers in Korea, and this was similar to the burden on the family imposed by stroke patients.25 However, overall, family function is relatively stable, and this may have a positive effect on the care received by COPD patients on home oxygen therapy.
There was a discrepancy between the prescribed and actual durations of oxygen therapy use. If we defined compliant as a patient who used oxygen within 1 hour of the prescribed duration of home oxygen therapy,26 35% of patients could be classified as compliant. This figure was not different from that of previously reported compliance rates derived after using a similar definition, ranging from 23% to 60%.2627 Like previous studies, we found that adherence to home oxygen therapy was suboptimal.
During exercise, 65.6% of patients did not use oxygen at all. Patients who did not use oxygen during exercise had more symptoms and worse HRQoL than those who used oxygen during exercise (Table 3). The severe respiratory symptoms and poor HRQoL were probably due to reduced physical activity. 27 As exercise capacity could be improved by providing home oxygen therapy,4 we should encourage COPD patients with home oxygen to use oxygen more continuously. Ambulatory oxygen therapy can facilitate patients using oxygen continuously—even during exercise. However, in this study, only 25.6% of patients used ambulatory oxygen. The high cost was a major reason that the patients did not use ambulatory oxygen. Over half of the patients responded that they could not use ambulatory oxygen because of the cost. This finding was consistent with that of a previous study.28 As ambulatory oxygen therapy has recently been covered by health insurance, more patients are expected to use ambulatory oxygen services just like in Denmark, where ambulatory oxygen therapy is fully covered by insurance.1029
LTOT has been known to confer a survival benefit if patients use supplemental oxygen for more than 15 hr/day.23 It is important not only for patients to adhere to their prescriptions but also for physicians to prescribe appropriately. Our study showed that only 32.3% of patients were prescribed more than 15 hr/day, and 45.7% of patients used oxygen more than 15 hr/day. These figures were much lower than that of previous studies conducted in Korea and Western countries, with previous values ranging from 68.2% to 98%.9283031 Previous reports have 40% to 70% of patients using more than 15 hr/day.32 In Korea, when pulmonologists prescribe home oxygen therapy, they usually only give patients a verbal explanation regarding how to use oxygen, and the spaces on the prescription pad designated for duration and flow of oxygen are often left blank. For that reason, despite most pulmonologists prescribing more than 15 hr/day of oxygen, our patients reported low rates of appropriate oxygen duration prescriptions.
We also evaluated the health care utilization andr medical costs among COPD patients using home oxygen therapy. It is well known that advanced COPD is associated with high costs, much of which can be attributed to hospitalizations.33 In our study, 60.5% of patients reported being hospitalized, and the mean frequency of hospitalization was 2.5 per year. This figure was similar to or larger than corresponding values reported by previous studies.343536 The patients enrolled in this study were spending about USD 300/month for COPD, which was a high cost considering that over half of patients the earned less than USD 900/month. The appropriate use of home oxygen can reduce hospitalizations and mitigate the economic burden imposed on COPD patients.34
This study had several limitations. First, we only relied on patient self-reporting. In terms of oxygen use, we did not ascertain oxygen concentrator clock counter values. Therefore, the findings may be affected by recall bias. In most recent studies, researchers have collected oxygen use data by checking the clock counter available on most concentrators,37 and this is necessary to obtain objective data. Second, there was no spirometry data. As the purpose of the study was to provide basic data regarding home oxygen therapy in Korea, accurate spirometry values were not necessary to obtain this information. Respiratory impairment was present in 70.3% of patients, among whom the required FEV1 would be ≤ 40% of predicted at least.14 This meant that at least 2/3 of patients had severe COPD in our study. Third, after we surveyed the questionnaire, health insurance began covering ambulatory oxygen therapy. Thus, the results of this study could be different from the current situation, especially financial problems.
In conclusion, Korean COPD patients on home oxygen therapy in our study had low adherence to home oxygen therapy, poor HRQoL, frequent hospitalizations, and a high financial burden. This study provided basic data to inform adequate management strategies to improve the quality of home oxygen therapy. Based on these results, a pilot study using education materials and home oxygen note, is in progress.
 XML Download
XML Download