

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Iron (Fe) is one of the most critical minerals in the human diet, which plays a vital role in the human body, including red blood cell production, DNA replication, muscle growth, oxygen transport, and other metabolic responsibilities [1]. The dietary iron can be categorized into 2 main groups - heme and non-heme iron. Although both iron groups are found in foods, the animal-based foods (including meat, seafood, and poultry) are the primary source of the heme iron, whereas the plant-based foods (including legumes, fruits, and vegetables) are considered the primary source of non-heme iron [2]. Heme iron has higher bioavailability than non-heme iron [3], because non-heme iron absorption can be influenced by other dietary components such as phytates, tannins, ascorbic acid, and copper [45].
During pregnancy, iron requirements increase to meet biological needs of the mother and fetus [6] (e.g., from 0.8 mg/day in the first trimester to 3–7.5 mg/day during the third trimester [2]). Previous reports indicate that more than 90% of pregnant women consume dietary iron less than the recommended amount (0.8 mg/day) [7], though deficiency rates differ according to socio-economical status, geographical region, and race [89]. Low levels of iron intake not only deplete the maternal iron store but also increase the possibility of iron deficiency (ID) and its comorbidities [10]. Therefore, iron supplementation is necessary in pregnant mothers [6].
Iron deficiency encompasses 75% of all anemias during pregnancy [10], which jeopardizes both mother and offspring's health [11]. Studies have demonstrated that ID correlates with increased risk of infant mortality and morbidity [10], neurodevelopmental disorders that involve the infant's future life [12], and high susceptibility of both mother and infant to infection [1314].
Researchers also discovered that ID is associated with higher risks of preterm birth (PB) [15], small for gestational age [16], and low birth weight (LBW) [17] but these adverse pregnancy outcomes may be easily prevented by the iron supplementation throughout the pregnancy [18]. Qiu et al. [19] investigated that high maternal intake of dietary heme iron before and during the first trimester of pregnancy raises the risk of gestational diabetes mellitus (GDM), although the effect of none-heme iron consumption on GDM was not clarified. Also, Brannon and Taylor [20] reviewed that high consumption of dietary iron during pregnancy can be as harmful as its low intake by elevating the possibility of disorders such as neurodegenerative diseases, PB, gastrointestinal health, and GDM.
There are still many controversies regarding the impact of maternal dietary iron on pregnancy outcomes and pregnancy-related complications. Furthermore, the primary focus of many studies was the effect of maternal total supplementation on the risk factors of the adverse pregnancy outcomes without considering the impact of heme and non-heme iron separately [111516].
We investigated the associations between maternal dietary iron intake (heme, non-heme, and total iron) during the first trimester of pregnancy with pregnancy outcomes (birth weight, birth height, and birth head circumferences) and pregnancy-related complications (pre-eclampsia, gestational hypertension, GDM, intrauterine growth restriction [IUGR], and nausea and vomiting in pregnancy [NVP]) among pregnant women of Isfahan, Iran. Our findings will provide some guidelines when performing the instructive and educative programs for pregnant mothers to decrease pregnancy-related complications and normalize the pregnancy outcomes by boosting the vulnerable pregnant mother's diet.
MATERIALS AND METHODS
Study design and participants
This prospective observational study was conducted among pregnant women during the first trimester. Eight-hundred and twelve pregnant women were selected randomly by the multistage cluster random sampling method from 20 various health centers across Isfahan city in the middle part of Iran during 2015–2016. Qualified criteria consisted of singleton pregnant women during the first trimester without any medical complication, use of medicine, and not following a particular diet. Exclusion criteria were twin pregnancies, smoking, history of abnormal pregnancy, supplementation usage, and no eagerness to follow-up during the study.
Consent forms were received from all participants. This study protocol was approved by the research council (research project No. 193053) and the research ethics committee of Isfahan University of Medical Sciences (research ethics No. IR.MUI.REC193053).
Data collection
Assessment of dietary intake
In order to assess the dietary intake of participants, pregnant women answered a validated 117-item food frequency questionnaires (FFQ) in the first visit, at 8–16 weeks. The validity and reliability of FFQ has been previously reported [21]. Participants reported the intake of each food item over the past 12 months, according to the standard, modified units, and serving sizes and frequency (on a daily, weekly, or monthly basis). The pregnant mothers reported their dietary intake based on 9 different choice categories. From “never or less than once a month” to “12 or more than per day”. We transformed all the consumed serving sizes from domestic measurements to grams. We computed nutrients and energy intakes by the Nutritionist IV software (version 7.0; N-Squared computing, Salem, OR, USA), designed for Iranian foods. We measured the nutrient values based on the energy-adjusted method.
Determination of iron
We used fundamental component analysis to determine the iron food items using in maternal dietary intake during early pregnancy by classifying them into 3 food groups, 1) heme-iron sources, 2) non-heme iron sources, and 3) total iron intake (that includes both heme and non-heme iron sources). Heme food sources include processed meat (sausages), eggs, poultry (chicken), fish (fish, tuna), and red meat (all kinds of meat, minced meat). Non-heme food sources consisted of leafy vegetables (raw vegetables, cooked vegetables, celery, spinach, and lettuce), green vegetables (green peas, green beans, and cucumber), nuts (peanuts, almonds, pistachios, hazelnuts, roasted seeds, and walnuts), and legumes (beans, peas, lima beans, broad beans, lentils, and soy). Total iron included all food items of both heme and non-heme food sources.
Assessment of GDM
GDM is abnormal glucose homeostasis identified by high fasting plasma glucose (more than 95 mg/dL), and 1-hour plasma glucose more than 140 mg/dL after consuming 50 g of glucose. This test was performed during the second trimester (between 24–28 weeks of pregnancy) [2].
Assessment of pre-eclampsia
The presence of hypertension and proteinuria, simultaneously, can be categorized as pre-eclampsia. Hypertension is a blood pressure with minimum 140 mmHg for systolic blood pressure (SBP) and a minimum of 90 mmHg for diastolic blood pressure (DBP). Pre-eclampsia was diagnosed when the above mentioned criteria was fulfilled twice when performed at least 4–6 weeks apart after the 20th week of pregnancy in women with normal blood pressure prior to pregnancy. Proteinuria is recognized as a urine protein concentration >300 mg/L from 24-hour urine samples [2].
Assessment of gestational hypertension
SBP > 140 mmHg or DBP > 90 mmHg, assessed twice after sitting for 15 minutes during or after the 20th week of amenorrhea or during 8–16 weeks of pregnancy [2].
Assessment of IUGR
Intrauterine growth restriction was defined as the newborn's birth weight being under the tenth percentile of the World Health Organization (WHO) newborn's growth chart or being malnourished according to the infant's nutritional assessment [2].
Assessment of other variables
The neonatal birth date, gestational age, anthropometric measurements such as birth weight, height, and head circumference recorded. These anthropometric measurements were defined according to the WHO standards including LBW: birth weight below 2,500 g, normal birth weight: birth weight above 2,500 g and below 3,900 g, low birth height (LBH): height below 47 cm, average height: height between 47 cm and 55 cm, and low birth head circumference: head measurement under 33 cm, average head circumference: head measurement between 33 cm and 37 cm [22]. We collected maternal anthropometric measurements (height, weight), maternal demographic data (education, occupation), and also recorded maternal clinical data (delivery status, IUGR, history of PB, abortion, and stillbirth) by using standard self-reported questionnaires. The participant’s weight was measured by a balanced digital scale to the nearest 100 g, with light clothes and barefoot conditions. A tape measure measured the participant's height in standing position. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. We also utilized the General Practice Physical Activity Questionnaire to evaluate the participant's physical activity level [23] that classifies the participant's physical activity into the 4 levels based on hours/week.
Statistical analysis
As we indicated before, by fundamental component analysis, we categorized the primary iron food sources and participants were categorized into tertiles by iron intake. Outcome emasures were evaluated across tertiles by 1-way analysis of variance (ANOVA). We used the Pearson χ2 test to assess differences among dietary iron intake tertiles for nominal data. In order to assess the relationships between quantitative data and iron intake tertiles, we used the ANOVA test. We utilized multivariable logistic regression models to compute odds ratio (OR), which the crude model was adjusted for energy intake (kcal), and the adjusted model was controlled for energy intake, age, economy, physical activity, and BMI. All statistical tests were 2-sided and p < 0.05 was considered statistically significant. SPSS 20.0 software (SPSS, Inc., Chicago, IL, USA) was utilized for all statistical analyses.
RESULT
The dietary iron intake (heme non-heme, and total iron) of 812 pregnant mothers (mean maternal age = 29.4 ± 4.85 years old) was categorized into tertiles [total iron (T1, 3.33–21.15; T2, 21.15–38.96; T3, 38.96–56.77 mg/day), heme iron (T1, 1.3–244.20; T2, 244.20–487.10; T3, 487.10–730 mg/day), and non-heme iron (T1, 2.5–300.8; T2, 300.8–599.1; T3, 599.1–897.4 mg/day)].
The mean total iron intake was 13.32 ± 5.72 mg during the first trimester of pregnancy and 13.44 ± 5.13 mg/d during the third trimester (Table 1). The participant's mean hemoglobin (Hb, 12.91 ± 1.06 g/dL) and hematocrit (HCT) levels (38.96 ± 2.55 g/dL) were both in the normal range of pregnant mothers during the first trimester of pregnancy (e.g., reference range: Hb, 11.0–14.3 g/dL and HCT, 31%–41%), which indicates that our population study was not at the risk of anemia. Other blood test results were within normal range [2].
Table 1
Baseline characteristics of included participants
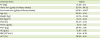
Values are presented as mean ± standard deviation.
BMI, body mass index; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; Hb, hemoglobin; RBC, red blood cell; HCT, hematocrit.
![]()
Prevalence of pregnancy-related outcomes (birth weight, birth height, and birth circumferences) differed across tertiles of dietary iron intake (heme, non-heme, and total iron). Total maternal iron intake during the first trimester of pregnancy was negatively associated with birth height (crude: p = 0.001, adjusted: p = 0.006) (Table 2). Greater total iron intake was associated with shorter birth height. When adjusting for BMI, physical activity level, economic status, age, and energy intake, maternal total iron intake was reversely correlated with the birth weight (adjusted p = 0.02).
Table 2
Mean neonatal birth weight, birth height, and birth head circumferences (pregnancy outcomes) among tertiles of maternal heme, non-heme, total iron intake

![]()
The cross-tabulated data (analyzed by the Pearson χ2 analysis) demonstrated that IUGR may be associated with non-heme iron intake (p = 0.004) (Table 3). The percentage of mothers that did not experience IUGR were highest in T2 of non-heme iron intake. Also, we found that the socio-economic status (such as income level, occupation, and educational status) of mothers is associated with maternal total iron consumption. Mothers with low socio-economic status had a lower intake of total iron than mothers with average or higher socio-economic status (p value < 0.001).
Table 3
Distribution of maternal characteristics, neonatal outcomes, and pregnancy complications according to tertiles of maternal iron consumption during early pregnancy

Number of participants in tertile (% of population in tertile). The p value calculated by χ2 test.
BMI, body mass index; IUGR, intrauterine growth restriction; NVP, nausea and vomiting in pregnancy; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBS, fasting blood sugar; T, tertile of consumption.
![]()
In the multivariate-adjusted ORs infant head circumference was positively associated with maternal total iron intake during the early pregnancy (p = 0.01,OR=7.57 CI= 1.86-30.71), while no association was found among other pregnancy outcome parameters (birth weight and birth height) or form of maternal dietary iron intake during the early pregnancy (Table 4).
Table 4
Odds ratios with 95% confidence intervals for pregnancy outcomes and pregnancy-related complications according to tertiles of maternal dietary iron consumption during early pregnancy

Adjusted models were adjusted for BMI, physical activity, age, economic, and energy intake. P value calculated by logistic regression.
FBS, fasting blood sugar; DBP, diastolic blood pressure; SBP, systolic blood pressure; NVP, nausea and vomiting in pregnancy; IUGR, intrauterine growth restriction; BMI, body mass index; T, tertile of consumption.
![]()
We also found that all types of maternal dietary iron intake (heme, non-heme, and total iron) tended to be negatively correlated with the risk of pre-eclampsia. In other words, dietary iron (heme, non-heme, and total iron) consumption may have a protective effect on the risk of the pre-eclampsia, one of the pregnancy-related complication's parameters (heme iron, crude p = 0.05, OR=0.68 CI= 0.42-1.12; non-heme iron, adjusted p = 0.02,OR=0.53 CI= 0.29-0.99; total iron, adjusted p = 0.05,OR=0.4 CI= 0.18-0.78) (Table 4).
IUGR was associated with a high intake of non-heme iron in both the crude and adjusted models (p = 0.01, crude; p = 0.01, adjusted) (Table 4). We also observed a meaningful association between the risk of fasting blood sugar (FBS) and high intake of maternal heme iron during the first trimester of pregnancy (crude p = 0.05; adjusted p = 0.04). When adjusted, DBP was also positively associated with total iron consumption (p = 0.05). In addition, maternal BMI was positively associated with both total iron and non-heme iron only in the unadjusted model (total iron, p = 0.03 and non-heme iron, p = 0.03).
DISCUSSION
Our study showed that maternal total iron intake during the early pregnancy is positively related to the birth head circumferences and reversely associated with other pregnancy-related outcome parameters, including birth weight, and birth height. Although, previous studies investigated that maternal ID communicates with a high-risk of infant's LBW [1718]. These controversial results depend on the health status of the population studied. In fact, in both studies [1718], most of the participants were stricken with the ID anemia, while our research participants were almost healthy, and their average intake of the total iron amount was higher than standards (Table 1).
Brannon and Taylor [20] demonstrated that a high intake of total iron is connected with the high possibility of the infant's growth retardation, which correlates with the prevalence of LBW, LBH, and other neurological disorders. High intake of iron increases the concentration of Hb and serum ferritin (SF) in the pregnant mother's blood that is both correlated with adverse pregnancy outcomes (LBW and LBH). Moreover, high Hb level causes the impaired plasma volume expansion, which not only stimulates the inflammatory responses but also increases the susceptibility to infections [24].
We also found that the maternal total iron intake directly associates with the offspring's birth head circumferences. Cerami et al. [1] demonstrated that low dietary iron during the early pregnancy grows the chance of infant's low birth head circumferences. Overall, iron is a critical cofactor for many vital neuro-reactions, including neurotransmitter's production, genome-related reactions, neuro-cell maturation procedure, and electron transition process that regulates all the brain's metabolism [25]. The dietary iron restriction decreases the brain's growth by interrupting all the iron-related mechanisms. Therefore, the brain's growth retardation will be present by the infant's low birth head circumferences [26].
Furthermore, Allen [27] demonstrated that the maternal dietary iron limitation causes hypoxia (low level of blood oxygen), and hypoxia stimulates the stress hormones secretion (such as norepinephrine, and cortisol). These stress hormones will increase the risk of oxidative stress in the placenta that interferes with the fetal neurodevelopmental mechanism and consequently decreases the offspring's birth head circumferences. Despite the total iron, we could not find any meaningful associations among both heme iron and non-heme iron and pregnancy-related outcomes separately.
According to our discoveries, non-heme iron can directly be associated with a high-risk of IUGR. Maged Fakher et al. [28] presented that mothers with low levels of SF are in a high-risk of bearing IUGR babies, which is so prevalent in the developing countries and families with low socio-economic status [29]. According to our study, pregnant mothers with a low level of socio-economic status consumed low levels of total iron than others (Table 3).
Moreover, studies show that developing communities' people supply their iron requirements mainly from the non-heme iron [29]. So, these findings can somehow approve that a pregnant mother consuming large amount of non-heme iron increases the risk of IUGR in their infants, although the possible biological mechanism is still unknown.
We explained the result by focusing on the function of both insulin and insulin-like growth factor-1 (IGF-1) hormones in the placenta. Insulin is one of the vital hormones that modulate the fetal growth. Fowden and Forhead [30] demonstrated that low levels of placenta's insulin correlate with a high-risk of IUGR. Also, IGF-1 is an essential hormone that provides both amino acids and glucose needs of the fetus across the placenta. So, low levels of IGF-1 can be either communicated with the fetus growth retardation and, therefore, high possibility of IUGR [31]. Studies demonstrated that the plant-based diet (vegan, Lacto-Ova vegetarian) is correlated with low levels of IGF-1 and insulin hormone secretion in the body [32]. As we mentioned before, the primary food source of none-heme iron is mainly plant-based foods, including legumes, fruits, and vegetables. Moreover, diaries and eggs contain mainly non-heme iron [2]. So, a diet of a pregnant mother with a high volume of non-heme iron may somehow resemble the Lacto-Ova vegetarian diet. However, she may use both heme and non-heme food sources. Nevertheless, the total calorie intake will be reduced due to high dietary fiber intake, which can decrease the secretion of insulin, and IGF-1 hormone in the fetus placenta blood circulation and finally elevate the risk of IUGR in the infant.
Our study represented that heme iron, non-heme, and total iron (in the condition of adjusting some participant's features) are negatively associated with the risk of pre-eclampsia. This result indicates that in some conditions, a high intake of maternal dietary intake (hem, non-heme, and total iron) during the first trimester of pregnancy can have a protective effect against pre-eclampsia. Whereas Kim et al. [33] investigated that during pre-eclampsia, the level of both serum iron and SF will increase. So, high iron intake, without anemia diagnosing, will increase not only the risk of pre-eclampsia but also the oxidative-stress reactions induced by the high levels of free iron [34]. It is essential to know that Kim et al. [33] demonstrated that the harmful effect of high iron supplementation on the risk of pre-eclampsia, in addition to the high dietary iron intake.
Furthermore, Kim et al. [33] found that pre-eclampsia is also correlated with low levels of serum zinc, calcium, and selenium. So, these microminerals can be easily found from all types of dietary iron (heme, non-heme, and total iron) [2]. So, increasing these dietary iron consumption, instead of supplementation, can prevent the pre-eclampsia. However, we cannot generalize our study result because of not finding meaningful associations in all of the conditions.
Our last finding declared that high levels of heme iron during the first trimester of pregnancy might be associated with a high-risk of maternal FBS. This result can prove the impact of heme iron consumption on the risk of GDM. Also, Qiu et al. [19] demonstrated that high heme iron during early pregnancy increases the incidence of GDM. Iron is a strong pro-oxidant, and high body iron levels can destroy the pancreatic β-cell function and impairs glucose metabolism by increasing the risk of insulin resistance in the body [9]. Wilson et al. [35] hypothesized that iron and insulin could have a synergist relationship with each other. Because high intake of iron stimulates the insulin hormone secretion in high volume to accelerate the iron cellular absorption through the increased ferritin receptors. So, it can be concluded that a high volume of insulin hormones due to high iron intake increases the possibility of insulin resistance and, finally, diabetes mellitus.
CONCLUSION
Maternal total iron is directly associated with the infant's birth head circumferences. While, high intake of total maternal iron during the early pregnancy of healthy pregnant mothers (without anemia and ID) can be communicated with both an infant's LBW and LBH. So, adequate iron consumption is recommended during the early pregnancy to improve pregnancy-related outcomes.
There is also a significant association between high intake of maternal non-heme iron during the first trimester of pregnancy and high-risk of IUGR. Also, the maternal heme iron intake may be associated with a high-risk of FBS, which elevates the possibility of GDM. So, for reducing these pregnancy-related complications, adequate intake of the non-heme food sources is necessary.
 XML Download
XML Download