

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
As the mean menopausal age of Korean women is 50.2 years and life expectancy of Korean women increase [1], women spend more than a third of their lives menopausal. Menopausal symptoms, such as sleep disorders, vaginal dryness, night sweats, and hot flashes appear during perimenopause and may persist or worsen during late menopause [2]. Although 75.9% of menopausal women experience more than one menopausal symptom, more than half of Korean menopausal women do not actively manage these symptoms [34]. The most common treatment to relieve menopausal symptoms is use of medications such as estrogen. However, hormone replacement therapy (HRT) can increase the risk of cancer and menopausal symptoms may re-emerge following termination of HRT. Therefore, other therapies are also being sought to alleviate menopausal symptoms.
Studies have shown that a balanced diet may attenuate menopausal symptoms and exercise is effective in improving health and alleviating physical and mental symptoms [567]. One possible therapy to attenuate menopausal symptoms is marine healing. Marine healing utilizes marine resources such as sea sand, sea breeze, and seawater to facilitate treatment of various diseases. This therapy is widely sought in Japan and is prescribed by medical staff to patients in Germany [8]. In France and Japan, some costs of marine healing are provided by the state with health insurance. In Germany, climate therapy in the Dead Sea has improved the viability of patients with vitiligo [9]. Mind-body intervention programs using marine resources improved sleep status and mental health in emotional labor employees [10]. One small study in Korean women found that the severity of vasomotor menopausal symptoms in peri- to post-menopausal women was lesser in those that consumed seaweed more frequently [11]. However, no studies have investigated the causal effect of seaweed intake on menopausal symptoms. The purpose of this study was to investigate if a short-term maritime healing program with or without sea mustard (Undaria pinnatifida) intake could relieve menopausal symptoms in women.
MATERIALS AND METHODS
Study design
Healthy women with menopausal symptoms self-selected whether to participate as the marine healing group or as a city control. Participants of the marine healing group were provided meals, housing, and marine healing programs located on the Sinji Myeongsasimni beach in Wando-gun, Jeollanam-do province for 5 days (July 8–13, 2019) (Figure 1). After the program, participants returned to their normal daily routine and were assessed for menopausal symptoms 13 days later. Among participants of the marine healing program, half were randomized to additionally consume U. pinnatifida (sea mustard). Sea mustard was provided in meals during the marine healing program and as a noodle snack after the program. The city control participants did not receive any intervention. Meals and marine healing programs were provided and participants were supervised throughout the program by research staff. All participants provided written informed consent. This study was approved by the Institutional Review Board (IRB) of Chonnam National University (IRB No. 1040198-190408-HR-020-07) and registered with the Clinical Research Information Service (No. KCT0004025).
 | Figure 1Study design. The marine group participated in a 5-day marine healing program. Diet was controlled for these 5 days. Within the marine group, the marine seaweed group additionally consumed sea mustard during the controlled feeding period (day 0–5, 15.4 g [dry weight]/day) and free-living period (8 packets of seaweed noodles per 13 days [180 g/packet]). The city group did not receive any intervention.▲, menopause rating scale survey.
|
Study participants
Healthy women with menopausal symptoms were recruited by posters at public health centers, district offices, apartment complexes, sports centers, and hospitals in Gwangju, Korea, and social media. The inclusion criteria were women who had menopausal symptoms and agreed to consume sea mustard if randomized to the seaweed group. The exclusion criteria were women who did not have menopausal symptoms, had administered antibiotics within 6 months, were smokers, or had severe gastrointestinal diseases. Subjects self-selected whether to participate in the marine healing program or as a city control. Within the marine group, participants were randomly assigned to consume seaweed (marine seaweed group) or control (marine control group) using computer generated random numbers program.
Marine healing program
Diet
Meals were provided according to each participants' energy and nutrient needs predicted by the 2015 Dietary Reference Intakes for Koreans. Most participants consumed 1,600 kcal/day while one participant was provided 2,000 kcal/day. Typical Korean meals consisting of rice, soup, kimchi, a main dish, and side dishes were served. Participants randomized to consume seaweed were provided 15.4 g (dry weight) of U. pinnatifida (sea mustard) per day. Sea mustard was added to the control meal in powder form or substituted for a vegetable of the control meal (for instance, when the marine control received vegetable porridge consisting of rice, carrots, zucchini, and mushroom, the marine seaweed group received sea mustard porridge made of rice and sea mustard). All ingredients were weighed before cooking and foods were weighed to the nearest 0.1 or 1 g before serving. Nutrientsin the provided foods were analyzed by Computer Aided Nutritional analysis program 5.0 for Professionals (The Korean Nutrition Society). Subjects consumed all food provided by the research staff and were monitored at all meals and snacks (1 research staff per 5 subjects) for compliance. If subjects could not consume a specific ingredient provided, the ingredient was replaced to a different ingredient within the same food group.
After the marine healing program, the marine group returned to their normal daily routine. The marine seaweed group was provided seaweed noodles primarily composed of sea mustard (99%; Seabest Korea, Gwangju, Korea). Participants were advised to consume 8 packets (180 g/packet) during the next 13 days. Compliance of seaweed noodle intake was measured by the number of packs of returned seaweed noodles. Participants of the marine control group did not receive any placebo. The city group was asked to continue their usual diet.
Physical and mental relaxation program
The marine group was involved in exercise and mental and physical relaxation programs using sea resources (seawater, sea breeze, sea sand, etc.) at least twice a day for 5 days. The schedule of marine healing programs implemented is presented in Table 1 and Figure 2. All programs were implemented by experienced instructors. Watsu and other massage therapies were performed by one instructor in a seawater swimming pool and indoors, respectively. Participants partook the seawater sauna in a specialized facility. Nordic walking and gyrokinesis were implemented in the Pinus thunbergii forest. The Hangul vocalization program is a patented program and was performed both indoors and on the beach to utilize sea sand, sea breeze, and sound of waves. The local tour included the Jungdo-ri Gugyedeung pebble beach and the Jeollanam-do Wando Arboretum. All programs were supervised by research staff (1 staff per 8–10 participants) to monitor safety and compliance to the programs.
Table 1
Marine healing program schedule

![]()

Menopause Rating Scale (MRS)
Changes in menopausal symptoms were assessed by the validated Korean version of the MRS [12]. The MRS is an 11-item self-reported scale that assesses the degree of discomfort due to menopausal symptoms. Symptoms are classified into 3 categories: somatic (hot flushes or sweating, heart discomfort, sleep problems, joint and muscular discomfort), psychological (depressive mood, irritability, anxiety, physical and mental exhaustion) and urogenital (sexual problems, bladder problems, dryness of vagina). The total score of the 11 items are used to assess the severity of menopausal symptoms as ‘no or little’ (0–4), mild (5–8), moderate (9–16), and severe (≥ 17). Cronbach's α ranged between 0.65 and 0.87 for each question [13]. The marine group conducted MRS surveys at baseline (T1), immediately after the marine healing program (day 6: T2) and 2 weeks later (day 18: T3). The city group completed 2 MRS surveys at baseline (T1) and 20 days later (T3).
Statistical analysis
All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). General characteristics and nutrient intakes were analyzed using Student's t-test and χ2 test. Change in MRS scores between T1 and T2 in the marine group were compared by paired t-test. Group effects (marine control vs. marine seaweed and marine vs. city) were assessed by mixed analysis of variance. Difference in magnitude of change between groups was assessed by analysis of covariance. All statistical significance levels were tested at p < 0.05.
RESULTS
Subject characteristics and dietary intake
A total of 42 women were recruited, of which 22 elected to be in the marine group and 20 participated as the city group (Table 2). Mean age was 53.6 (± 4.6) years (range, 44–65) and mean body mass index was 23.4 (± 3.4). No difference in baseline values were found between the marine control and marine seaweed group. A higher percentage of participants in the city group were employed compared to the marine group (65% vs. 32%, p = 0.03). Mean daily energy intake of participants recommended for the 1,600 kcal/day was 1,673.99 (± 169.05) kcal (Table 3). Fiber and calcium intakes were significantly higher in the seaweed group (p < 0.05) but other nutrients did not differ between groups.
Table 2
Subject characteristics*

Values are mean ± standard deviation or number (%).
*Comparisons between the marine seaweed and marine control, and between the marine and city group were made by Students t-test or χ2 test. The number of participants missing data for age at menarche: n = 1, age at menopause: n = 3, and income: n = 2.
![]()
Table 3
Mean nutrient intakes of the marine control group and marine seaweed group during the 5-day controlled feeding period
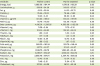
Intake of one subject (2,000 kcal/day) was excluded from the analyses. All other participants were aimed to provide 1,600 kcal/day. Comparisons between the marine control and marine seaweed groups were assessed using Student's t-test.
![]()
Menopausal symptoms
The MRS scores at baseline and pattern of change in scores within the marine group did not differ between those consuming sea mustard and marine controls (Figure 3), and thus the data was combined for the following analyses. Both the marine group and city group had moderate somatic, psychological, and urogenital symptoms at baseline (T1; Table 4). Somatic, psychological, urogenital, and total MRS scores dramatically decreased in the marine group immediately after the marine healing program (from 6.86 ± 3.97 to 4.45 ± 3.20, from 6.59 ± 3.85 to 3.45 ± 3.69, from 4.50 ± 2.82 to 3.05 ± 2.87, and from 17.95 ± 9.08 to 10.95 ± 8.81, respectively). The treatment effect was not evident by T3 (day 18–20) for most values. However, an interaction between time and treatment was found for physical and mental exhaustion (question 7; p = 0.04). No treatment effect was observed for somatic, psychological, urogenital, and total MRS scores. Sleep problems (#3), bladder problems (#9), vaginal dryness (#10), and joint and muscular discomfort (#11) were alleviated with time, resulting in a decrease of somatic, psychological, urogenital, and total MRS scores. Exclusion of those with low baseline MRS scores (all categories ≤ 1; n = 2 per group in the marine and city group) or city controls that went on vacation during the study (n = 3) resulted in a trend for interaction for physical and mental exhaustion (p = 0.06 for both analyses). A trend of interaction also appeared for psychological symptoms when subjects with low baseline MRS scores were excluded (p = 0.08). No difference was found by employment status within the city control group (data not shown).
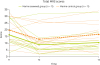 | Figure 3Total MRS scores of participants that participated in marine healing by status of sea mustard consumption and time point. The thick lines represent the means of each group (marine control and marine seaweed).MRS, Menopause Rating Scale.
|
Table 4
Mean MRS scores of participants that participated in marine healing (marine group) and city controls by time point*
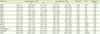
MRS, Menopause Rating Scale.
*Analyses were performed by mixed analysis of variance to compare T1 and T3 of the marine and city group. Within the marine group, paired t-test was used to assessed the difference between T1 and T2; †p < 0.05.
![]()
DISCUSSION
Even a 5-day marine healing program can immediately relieve somatic, psychological, and urogenital symptoms of menopausal women. The effects of marine healing on physical and mental exhaustion lasted for 2 weeks. However, U. pinnatifida did not affect menopausal symptoms during marine healing.
We did not find any effect of U. pinnatifida on somatic, psychological, or urogenital MRS scores which is in line with the previous observational study which also did not find any association between physical, psychosocial, or sexual domains using the Menopause-specific Quality of Life Questionnaire [11]. However, the previous study found that seaweed, fish, and vegetable oil intake was associated with alleviated vasomotor symptoms [11]. Although the MRS used in the present study does not have multiple questions to assess vasomotor domains, one question (#1) assessed night sweats, hot flashes, and flushes. In contrast to the previous observational study, additional intake of U. pinnatifida when participating in marine healing did not alleviate these symptoms. Koreans consume a variety of seaweeds in addition to U. pinnatifida, though this is one of the most popular seaweeds. Therefore, it is possible that other seaweeds may affect vasomotor symptoms of menopause. On the other hand, the balanced diet we provided during the maritime healing program may have facilitated its effect on menopausal symptoms. The National Institute of Aging of the National Institute of Health advises menopausal women to avoid alcohol, spicy foods, and caffeine, as they may cause menopausal symptoms to worsen [14]. Similarly, observational studies in Koreans point to a positive association between alcohol and wheat consumption and severity of menopause symptoms [15]. In Spanish-speaking women, diets including regular hot spicy food intak caffeine e was associated with hot flush frequency [16]. Participants in our study were not served alcohol,, or very spicy items and the amount of wheat-based products was small. Therefore, a well-balanced mild diet, but not U. pinnatifida alone, may reduce menopausal symptoms in Korean women.
Exercise, mind-body practices, and relaxation breathing are known to alleviate menopausal symptoms [1417]. Observational studies resulted in a negative association between strenuous exercise and menopausal symptoms. Even short-term aerobic and resistance exercise interventions can reduce psychological and somatic complaints [18]. Observations indicate that physically active Korean women have fewer severe physical symptoms of menopause [19]. Women in our study participated in mostly aerobic exercises such as walking, Nordic walking, and jogging on the beach. A weekly integrated program of exercise (including stretching and Kegel exercise), laughter therapy, rational emotive therapy, and guided imagery for 6 weeks reduced physical, sexual, and depressive symptoms of middle-aged Korean women [20]. No previous studies on the effect of Watsu or saunas on menopausal symptoms were found. However, small studies have found that Watsu is beneficial in stress relief in pregnant women [21] and fibromyalgia syndrome patients and improves ambulatory function of stroke patients [22]. Our 5-day marine healing program proved to be beneficial for women with menopausal symptoms. However, a major reason for the null effect of marine healing by day 20 for most outcomes is due to the simultaneous decrease of menopausal symptoms in the control group. As vacation or employment status was not associated with MRS in our city controls, we currently are unable to specify the reason for the significant decreases found with time in the control group. Still, the marine healing program alleviated physical and mental exhaustion 2-weeks post participation.
We are the first to investigate the effect of an integrated program of diet, exercise, and mental relaxation with sea resources on menopausal symptoms. Though a balanced diet, physical activity, and relaxation techniques can be implemented elsewhere, the effect of marine resources seem to have enhanced the positive effect on menopausal symptoms. Approximately half of our participants were involved in regular exercise at baseline, and most participants in the marine group self-reported oneself to be health conscious. In addition, the exclusion of city controls that went on vacation during the study minimally affected the results, indicating that marine healing specifically attenuates physical and emotional exhaustion. A 3-day forest camp consisting of forest bathing, walking, landscape viewing, meditating, and natural herbal food intake with meals in postmenopausal women resulted in dramatically increased quality of life perception, which persisted up to 4 weeks [23]. This indicates that natural resources can strongly affect one's stress levels. Among Korean female emotional labor workers, mind-body interventions utilizing marine resources enhanced quality of life, emotional and psychological domains, social relations, and cognitive function for up to 1.5 months post-intervention [10]. Our study design does not allow us to measure the individual effects of diet, exercise, mind-body practices, and environment, but clearly show that even a short marine healing program can benefit women with menopausal symptoms, especially for physical and mental exhaustion.
CONCLUSION
A 5-day program consisting of balanced meals, exercise, and mind-body practices using sea resources such as sea sand, sea breeze, and sea water, immediately alleviates somatic, psychological, and urogenital symptoms of menopause. The benefit of marine healing on physical and emotional exhaustion continued to 2 weeks-post intervention. Thus, marine healing may be an effective method to assist women with menopausal symptoms.
 XML Download
XML Download