

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Adult skeletal Class II patients can be treated with upper molar distalization or premolar extraction as a camouflage treatment. Extraction is advantageous for patients with significant crowding and protrusion. However, in cases with severe crowding and retrusive lips, extraction treatment should be carefully evaluated to avoid worsening the patient's profile. If extraction is not an acceptable option to relieve the crowding and proclined incisors, expansion or distalization of the arch should be considered.
Historically, the use of headgear was one of the many successful methods for correction of Class II malocclusion; this approach mainly distalizes the maxillary molars to correct dental discrepancies.12 However, in many cases, patients refuse to wear headgear because of esthetic and social concerns, and the success of this approach primarily depends on patient compliance,3 since a lack of compliance can cause anchorage loss and unsatisfactory treatment results. Dangerous facial injuries are another potential disadvantage of headgear usage.45 These disadvantages have necessitated the development of other approaches for intraoral molar distalization.
To address this requirement, many intraoral appliances such as push-coils,6 pendulums,78 magnets,910 distal jets,1112 superelastic nickel-titanium (NiTi) wires,13 and molar sliders have been developed for maxillary molar distalization.14 Although these are extremely useful when they are used for distalization, they are associated with a number of potential disadvantages, including extrusion and rotation of molars, anchorage loss with anterior teeth, and tipping.
More recently, temporary anchorage devices (TADs) have been used to prevent these side effects. In comparison with buccal TADs, palatal TADs offer several advantages such as a lower risk of contacting the roots of adjacent teeth and a wide range of actions not limited by the interradicular space.15 This report presents the findings for a 25-year-old male patient with severe crowding and retrusive lips and a missing lower incisor who was treated with total arch distalization using a palatal anchorage plate.
DIAGNOSIS AND TREATMENT PLANNING
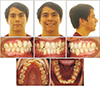
A 25-year-old man visited the clinic with a primary complaint of upper and lower crowding and a missing lower tooth. His pre-treatment facial profile photographs indicated a convex profile with retrusive lips. An intraoral examination indicated severe and moderate crowding in his maxillary and mandibular arch, respectively. He also had an anterior crossbite on the upper lateral incisors and a Class I molar relationship. His maxillary dental midline was 2 mm to the right while his mandibular dental midline was not an issue because of the missing tooth. He did not show any functional shift, and there were no symptoms of temporomandibular disorder. We estimated the width of the missing incisor based on the width of the other incisors. His anterior Bolton ratio was 72% (mandibular deficiency or maxillary excess) (Figures 1 and 2).
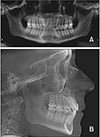
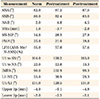
The initial radiographic evaluation confirmed the missing incisor and the fact that no third molars were present. It also showed that there were no pathological findings. Lateral cephalometric analysis indicated a skeletal Class II pattern with a hypodivergent growth pattern (ANB = 4.8°, Wits appraisal = −3.7 mm, and SN-MP = 28.5°). His maxillary incisors were retroclined and his mandibular incisors were proclined (U1-SN = 100.2°, IMPA = 102.9°) (Table 1 and Figure 3).
A treatment plan involving extraction of the maxillary first premolars or maxillary premolars and one mandibular incisor was suggested, but the patient refused it (Figures 4, 5, 6, 7). Therefore, we proposed molar distalization using a palatal anchorage plate with TADs to create sufficient space for his lingually displaced maxillary lateral incisors while still maintaining the Class I molar relationship.
TREATMENT OBJECTIVES
The following treatment objectives were established: (1) relieve crowding in both arches, (2) correct anterior crossbite, (3) maintain Class I molar relationship, (4) obtain optimal overjet and overbite, (5) obtain a stable occlusal relationship, and (6) enhance dental and facial esthetics.
TREATMENT PROGRESS
The patient was first referred to a general dentist for treatment of dental caries. Orthodontic treatment was initiated by bonding preadjusted appliances with 0.022-inch (in) slots on both arches for leveling and alignment. The maxillary arch was leveled with archwires, starting with a 0.016-in NiTi archwire and going up to 0.019 × 0.025-in NiTi wires. Under local anesthesia, 8-mm length and 2-mm diameter miniscrews (Jeil Medical, Seoul, Korea) were placed in the three holes of a modified C-palatal plate (MCPP), two posterior and one offset anteriorly, slightly lateral to the midpalatal suture. A stainless steel palatal wire (1 mm in diameter) with anterior hooks was soldered to the maxillary first molar bands, and approximately 250 g of distalizing force was applied between the hooks and the MCPP lever arms on each side via elastomeric chains.1617
Elastomeric chains were connected from the plate to the hooks on the upper palatal bar and retied every two weeks with a 0.017 × 0.025-in stainless steel archwire for a total distalization period of 18 months. Class III elastics were then used for retraction of the mandibular dentition to achieve a Class I molar relationship. After distalization, the crowding was resolved and the MCPP was removed. A panoramic radiograph was then taken and brackets were repositioned to ensure root parallelism. Interproximal reduction of the maxillary and mandibular canine-to-canine was performed to help reduce black triangles and to reduce the maxillary incisor proclination caused by the open coil spring that was used to create space for the blocked-out laterals. Finishing and detailing were performed in conjunction with up-and-down elastics on 0.016 × 0.022-in stainless steel arch wires. Fixed retainers were attached to the anterior teeth, and removable retainers were also delivered to provide secure stability. The total treatment period was 21 months (Figures 8, 9, 10, 11).
RESULTS
Post-treatment facial photographs showed improved smile esthetics and a satisfactory overbite and overjet. The patient's Class I canine molar relationships were maintained. A post-treatment panoramic radiograph confirmed acceptable root parallelism despite a dilacerated maxillary right central incisor. There were no significant signs of bone resorption.
Post-treatment lateral cephalometric analysis and superimposition indicated no significant skeletal changes (ANB = 4.5°, SN-MP = 27.9°) compared to the pretreatment status. The maxillary incisors showed normal inclination (U1-SN = 103.0°), and the mandibular incisor inclination had improved (pre-treatment IMPA = 102.9°, post-treatment IMPA = 99.3°). The patient's maxillary molars were distalized successfully with 4.2° of distal tipping measured from the Frankfort horizontal. There was no significant extrusion. The patient reported no temporomandibular joint pain or discomfort during or after orthodontic treatment. His American Board of Orthodontics cast-radiograph evaluation score was 14 (Figures 12, 13, 14, 15, 16, 17, 18).
DISCUSSION
The esthetic and social concerns associated with headgear use for molar distalization have motivated many clinicians to consider other molar distalization techniques.467891011121314 Intraoral distalization appliances are a plausible alternative but can cause an unavoidable, adverse, reciprocal mesial movement of the anterior teeth and premolars during distal movement of the molars. After regaining the space with molar distalization, the anterior teeth and premolars that initially moved forward should be retracted. However, the molars that were already distalized are used as anchorage for retraction of the anterior teeth, which causes them to move anteriorly and thus reduce the efficiency of the distalization.18
Skeletal anchorage systems have been employed as an alternative treatment modality in orthodontics over the past two decades.192021 One of the most important applications of skeletal anchorage systems is molar distalization. The major advantages of using TADs for distalization, in comparison with conventional treatment that uses headgear or intraoral appliances, are the lack of esthetic impairment and preservation of the anchorage during distalization of the molars.
Park et al.22 found that all maxillary teeth showed intrusion and distal tipping during molar distalization with buccal miniscrews. These effects were attributed to the limited control over retraction force vectors. However, with MCPPs, superior control over the force vectors can be obtained through several notches on the plate, which makes it more versatile. The extent of intrusion and tipping is controlled by engaging elastics in the appropriate notches.23 Furthermore, they allow teeth to be moved farther without requiring relocation of the miniscrews.
Distalization of the entire maxillary dentition requires the application of a 450 to 500 g force. Since a single miniscrew cannot withstand such heavy forces,24 MCPPs are anchored with three miniscrews. Considering a 2.5-mm-high screw tube and 8-mm-long miniscrew, the net length of the miniscrew that is embedded in palatal bone is 5.5 mm. Ryu et al.25 reported that the palatal bone thickness in the permanent dentition is 5.5 mm in the midpalate and 5.9 mm in the posterior palate, making penetration of the nasal cavity unlikely. The palatal approach might also be a crucial component in achieving bodily movement without extrusion of the molars.26 Yu et al.27 reported that the rate of distal tipping and extrusion in palatal plate cases was lower than that with buccal miniscrews. According to the reported case, the distal tipping was about 4°.
The thickness of palatal bone and soft tissue can usually support TADs in adults and adolescents. The most appropriate regions in the palate for TAD placement have been adequately described in previous studies.2528 Recently, the treatment effects of palatal plates in distalization of the maxillary dentition in adults and adolescents was evaluated comprehensively by Kook et al.29 MCPP can be an effective appliance for maxillary distalization without significant side effects for patients who refuse to undergo extraction treatment.
CONCLUSION
The palate is a safe site for TAD installation because of its appropriate characteristics such as bone quantity and quality and soft tissue thickness. The application procedure is minimally invasive and short in duration. Molars can be distalized efficiently without loss of anchorage or any significant tipping. No cooperation is required other than good oral hygiene with MCPP. This is a simple and effective nonextraction approach for distalization of the maxillary dentition with a relatively true bodily movement of the maxillary first molars.















 XML Download
XML Download