

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Placenta previa can cause profuse maternal hemorrhage and markedly increase the risk of blood transfusion.12 When massive bleeding is expected, a discussion among multidisciplinary experts, including maternal-fetal medicine specialists, anesthesiologists, and transfusion medicine physicians, is needed regarding the management of the patient.34 Owing to the nature of placenta previa, bleeding during cesarean section occurs immediately after placental separation.
The preoperative preparation of women with placenta previa is important, given the risk of rapid and massive blood loss.5 Intravenous access with a large-bore cannula is recommended, and central venous access should be considered.3 However, as the insertion of a central venous catheter is associated with various complications,6 the application must be carefully decided. Blood products should also be immediately available when needed. It takes time to prepare blood products; especially for fresh frozen plasma, an hour may be needed for thawing.7 If massive hemorrhage is anticipated, cross-matched blood products should be available in the operating suite before surgery is initiated.3 However, since unused prepared blood needs to be discarded, it is necessary to predict the amount of blood transfusions.
In recent decades, obstetric massive transfusion protocols have been shifting to the direction of early administration of fresh frozen plasma, platelets, and cryoprecipitate.8 Pacheco et al.8 recommended that when bleeding continues after the transfusion of 4 units of packed red blood cells (PRBCs) within a short period, the surgeon or anesthesiologist should consider activating the massive transfusion protocol. The ability to predict whether a situation requiring activation of a massive transfusion protocol would arise will be helpful in the preoperative preparation for a cesarean section. This study aimed to develop a prediction model for the transfusion of ≥5 units of PRBCs during cesarean section in pregnancies complicated by placenta previa.
Go to : 
MATERIALS AND METHODS
Study design and data source
We conducted a retrospective cohort study including 287 women with placenta previa who delivered between September 2011 and April 2018 at Wonju Severance Christian Hospital, a tertiary hospital. We reviewed the clinical records including maternal demographics, clinical findings, ultrasound findings, and blood bank data. These data were used to develop the model in our study. For the external validation set, we obtained data (n=50) from another tertiary hospital (Samsung Medical Center, Seoul, Korea).
Clinical factors
Clinical factors, including maternal age, abortion history, cesarean section history, gestational age at delivery, whether the operation was carried out as an emergency surgery, and whether bleeding had started before the operation, were evaluated. The number of abortion history was counted only if a dilatation and curettage was performed. Preoperative hemoglobin and hematocrit values were checked. The amount of PRBCs transfused during operation was measured. The primary outcome was transfusion of ≥5 units of PRBCs during operation.
Ultrasound factors
A diagnosis of placenta previa was made when the placenta covered the internal orifice of the cervix after 32 weeks' gestation. If placenta previa was suspected while performing routine prenatal ultrasonography, transvaginal ultrasonography was always performed to verify the exact location of the placenta. If diagnosed in the second trimester of pregnancy, it was verified again after 32 weeks. A diagnosis of total placenta previa or partial placenta previa was made when the internal orifice of the cervix was completely or partially covered, respectively. When the lower margin of the placenta was located at the edge of the internal orifice of the cervix, the condition was diagnosed as marginal placenta previa. We diagnosed low-lying placenta when the lower margin was located within 2 cm of the internal orifice of the cervix. Lacuna was defined as a lake-like irregular area of low echogenicity within the placental parenchyma.9 We graded intraplacental lacunae as follows: 0, no lacuna was detected; 1+, 1–3 generally small lacunae were present; 2+, 4–6 larger or more irregular lacunae were present; and 3+, many lacunae detected throughout the placenta, some appearing large and irregular in shape.9 We checked for the presence of a hypoechoic area between the myometrium and the placenta. The vascularity of the placenta was classified as normal or hypervascular on color Doppler imaging. We examined whether or not the placenta was located on the anterior wall of the uterus.
Statistical analysis
To compare the characteristics of women who received massive transfusion and those who did not receive transfusion, Mann-Whitney U-test was used for continuous variables, based on the normality assumptions from Kolmogorov-Smirnov test. Meanwhile, chi-square test or Fisher's exact test was used to compare categorical variables.
Univariate and multivariable logistic regression analyses were used to test the association between massive transfusion and maternal age, degree of previa, history of abortion, gestational age at delivery, emergency surgery, preoperative bleeding, preoperative hemoglobin, preoperative hematocrit, lacunae, hypoechoic layer, placental hypervascularity, and anterior placentation.
Hosmer-Lemeshow goodness-of-fit test was used to assess the suitability of the models. The discrimination of the model was measured using the area under the receiver operating characteristic (ROC) curve (AUC). The calibration of nomogram was assessed graphically.
Analyses were performed using SAS program (version 9.4; SAS Institute Inc., Cary, NC, USA) and R Statistical Package (version 3.5.1; Institute for Statistics and Mathematics, Vienna, Austria; www.R-project.org).
Ethical approval
The Institutional Review Board of Yonsei University Wonju Severance Christian Hospital (approval no. CR318045) approved this study on July 3, 2018 and waived the requirement for a written informed consent. For the external validation, we obtained Institutional Review Board approval from Samsung Medical Center (approval no. SMC 2013-12-021).
Go to :
RESULTS
Of 287 women whose information were included in the data used to develop the model, 266 (92.7%) did not receive massive transfusion and 21 (7.3%) received massive transfusion during cesarean section. Total previa was observed in 20 (95.2%) women with massive transfusion and in 83 (31.2%) women without massive transfusion, and previa showed a statistically significant difference according to the massive transfusion (p<0.001) (Table 1). Abortion history, lacunae, lack of a hypoechoic layer, and anterior placentation were all significantly associated with massive transfusion (p<0.05). There were nine cases of cesarean hysterectomy in this cohort, and no cases in which embolization was performed.
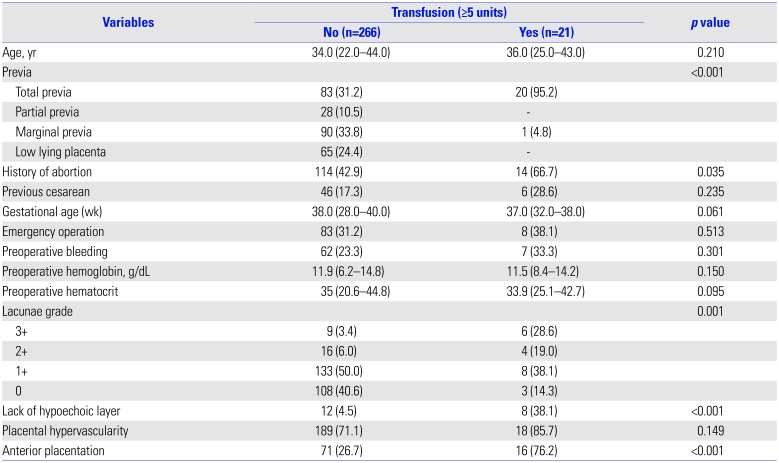
Table 1
Comparison of the Clinical Factors from Data Used to Develop the Model (n=287)
![]()
Prediction model of massive transfusion
Table 2 summarizes the results of univariate and multivariable logistic regression analyses of clinical and ultrasound factors in the data used to develop the model. We selected variables with p values <0.25 and applied them to the prediction equation to build the model step by step. The p value of Hosmer-Lemeshow test was >0.05 for the two models, indicating that the models were suitable.
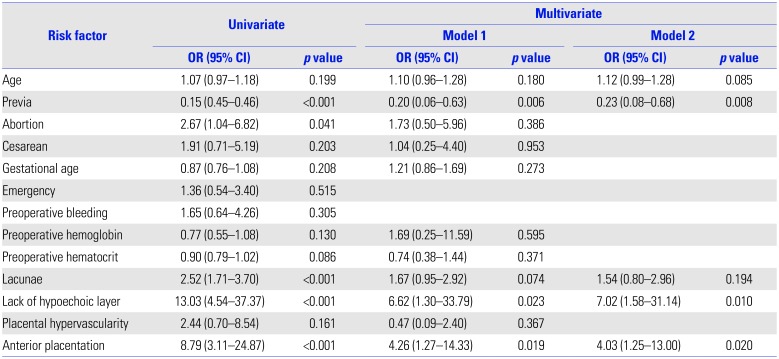
Table 2
Results of Univariate and Multivariate Logistic Regression Analyses Testing the Association between Massive Transfusion and Clinical Characteristics
![]()
The overall predictive accuracy of model 1, as measured using the bootstrap-corrected ROC curve, was 0.938 [95% confidence interval (CI) 0.90–0.96], whereas that of model 2 was 0.922 (95% CI 0.89–0.95), both of which were similar. Comparison of AUC of the two prediction models showed that both models had good discrimination ability (Table 3, Fig. 1). ROC curve comparison of the two models was not statistically significant (p=0.253). Therefore, model 2 was selected as the final model, considering the number of variables.


Table 3
Comparison of the Prediction Models by Multivariate Logistic Regression Analysis
| Model | Number of prediction variable | AIC | AUC | SE | 95% CI |
|---|---|---|---|---|---|
| Model 1 | 11 | 114.580 | 0.938 | 0.019 | 0.90–0.96 |
| Model 2 | 5 | 107.409 | 0.922 | 0.026 | 0.89–0.95 |
AIC, Akaike's information criterion; AUC, area under the receiver operating characteristic curve; SE, standard error; CI, confidence interval.
Model 1: Age, previa, history of abortion, previous cesarean, gestational age, preoperative hemoglobin, preoperative hematocrit, lacunae, hypoechoic layer, placental hypervascularity, and anterior placentation. Model 2: Age, previa, lacunae, hypoechoic layer, and anterior placentation.
![]()

In the external validation, discrimination was good with an AUC value of 0.833 (95% CI 0.701 to 0.924) for model 2.
Nomogram of massive transfusion
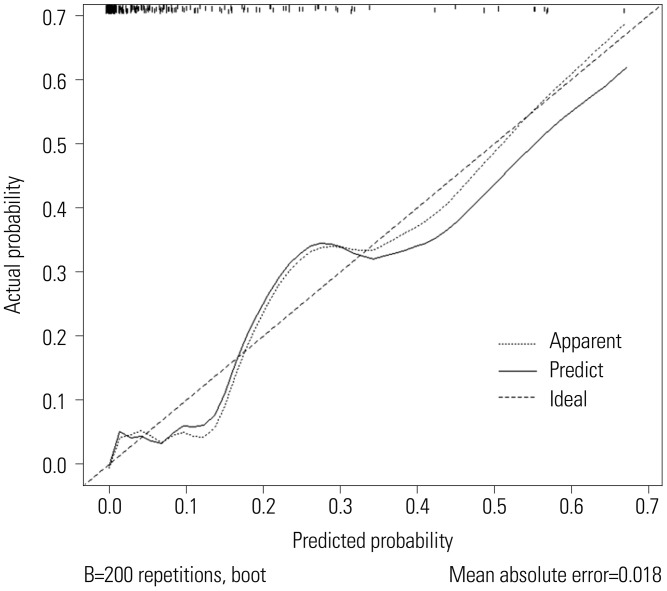
A nomogram was constructed based on model 2 with the data used for model development (Fig. 2). Nomogram calibration plots indicated good agreement between predicted and observed outcomes, exhibiting close approximation between predicted and observed probability (Fig. 3).

The nomogram consisted of five rows, from which the probability of massive transfusion for each patient can be calculated. The first row (points) in the nomogram contains the point assignment for each variable. Rows 2 through 6 represent the variables included in the model. For an individual patient, each variable is assigned a point value based on clinical characteristics. To determine the point assignment, a vertical line is made between the appropriate variable value and the point line. For example, total previa (previa, 1) confers about 100 points. The assigned points for all five variables were summed, and the total was found in row 7 (total points). A vertical line was made between the total point and corresponding value in the final row (probability of transfusion, five units).
Go to :
DISCUSSION
We developed a prediction model for transfusion of ≥5 units of PRBCs during cesarean section in pregnancies complicated by placenta previa. Placenta previa is associated with maternal complications such as antepartum bleeding, intrapartum and postpartum hemorrhages, blood transfusion, hysterectomy, septicemia, and thrombophlebitis.10 These morbidities can increase, especially when placenta accreta is also present, and even result in death.1
There are several clinical risk factors for placenta accreta. Advanced maternal age and previous cesarean birth are associated with an increased risk of placenta accreta.11121314 Uterine curettage is associated with an increased likelihood of developing an abnormally invasive placenta.12 Shamshirsaz et al.15 showed that women with morbidly adherent placenta requiring urgent delivery have worse outcome than women with a planned delivery. In their study, fewer units of PRBCs and fresh frozen plasma were transfused in the planned delivery group.15
Ultrasonography is the primary tool for the evaluation of potential presence of placenta accreta.1617 Placenta previa is associated with an increased risk of placenta accreta.1112 Hypervascularity is positively associated with a morbidly adherent placenta.18 Anterior placentation is also associated with placental invasion.1819 Considering the definition of placenta accreta (i.e., the placenta is attached to the myometrium without an intervening decidua), it is important to check for the presence of a retroplacental hypoechoic area. Loss of the normal hypoechoic retroplacental myometrial zone is highly predictive of a morbidly adherent placenta.1820 Patients with placenta previa and a lacunar pattern within the placenta have a higher risk of having an abnormally implanted placenta.21 Finberg and Williams9 defined four lacunar grades depending on the number, size, and shape of lacunar spaces within the placental parenchyma. The presence of grade ≥2+ lacunae is strongly associated with variants of placenta accreta, such as placenta increta and percreta.22 In our study, the degree of placenta previa, anterior placentation, loss of the normal hypoechoic retroplacental myometrial zone, and high-grade lacunae were associated with the risk of transfusion of ≥5 units of PRBCs during operation.
In placenta previa, prenatal diagnosis relying solely on prenatal ultrasound still lacks clinical correlation.23 A variety of models for predicting perioperative complications in women with placenta previa have been presented.242526 Pivano et al.24 made a scoring system to predict the risk of emergency cesarean section in women with antepartum bleeding and placenta previa. Tanimura et al.25 developed a scoring system for predicting adherent placenta in women with placenta previa. Choi et al.26 identified history of abortion, prior cesarean section, and total previa as strong antepartum risk factors associated with peripartum cesarean hysterectomy in women with placenta previa. Several studies have attempted to predict massive peripartum bleeding in cases of placenta previa.2728 However, it is difficult to accurately estimate blood loss during cesarean section.29 There have been attempts to predict the amount of transfusion during cesarean section with more objective measurements.3031 Yoon et al.30 made a scoring model that predicts the occurrence of blood transfusion, and not a specific amount of blood transfusion. Kim et al.31 developed a scoring system that predicts transfusion of ≥8 units of PRBCs within 24 h after delivery only in women with total placenta previa.
The traditional definition of a massive transfusion (i.e., ≥10 units of RBCs within a 24-h period) has been modified to better reflect the true coagulation biochemistry.3233 Holcomb et al.34 showed that increased plasma- and platelet-to-RBC ratios improved outcomes in massively transfused trauma patients. The combination of early recognition and intervention may be more important than a specific administration ratio of blood products.835 When bleeding continues after transfusion of 4–5 units of RBCs within a short time, activation of massive transfusion protocol should be considered.83637 Based on the aforementioned rationale, we identified our primary outcome as transfusion of ≥5 units of PRBCs during cesarean section. Our scoring model differed from others in that it focused on prediction for massive transfusion based on recent criteria.
We attempted to create an easy-to apply predictive model for clinical use. For this purpose, the predictive model should only consist of variables that are usually available in real-world clinical situations. The fewer the variables, the more widely available the model can be. We constructed two predictive models. As there were no significant differences between the overall prediction accuracy of the two models, we adopted the model with fewer variables. To facilitate the calculation of the probability of massive transfusion in clinical setting, we constructed a nomogram using the prediction equation (Fig. 2).
To determine the generalizability of a prediction model across different patient profiles, external validation is necessary.38 Most of the published studies about prediction models for transfusion in placenta previa performed validation with a different time group from the same cohort.31 Our prediction model was validated using data from another institution. We quantified the performance of the prediction models by assessing discrimination with AUC values, which showed good discrimination, as well as calibration, which exhibited close approximation between predicted and observed probability.39
This study was limited by the nature of retrospective cohorts. The acquisition of some clinical variables relied solely on the review of medical records. In the case of abortion history, data regarding complete abortion were not obtained; therefore, only dilatation and curettage history was included. When blood transfusion was decided, the anesthesiologists were already aware of the risk factors of bleeding. If there were well-known risk factors such as previa, history of cesarean section, or abortion, the decision could have been biased toward transfusions.
In conclusion, we constructed an externally validated prediction model for massive transfusion reflecting recent criteria during cesarean section in women with placenta previa. In order to obtain a reproducible result using this prediction model, it is recommended that the grade of lacunae and presence of retroplacental hypoechoic layer, as well as the classification of previa and placental location, are accurately verified during prenatal ultrasound. This scoring model would provide practical help in determining the need to prepare an appropriate amount of blood products and the optimal timing of blood transfusion.
Go to :
 XML Download
XML Download