

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Liver cirrhosis is a global health and economic burden, causing significant mortality.1 One of the severe complications in patients with cirrhosis is bacterial infection.2 Bacterial infection is a major cause of acute decompensation in patients with cirrhosis and has been shown to be a trigger for developing acuteon-chronic liver failure in acute decompensated cirrhosis patients, which is a key prognostic determinant and is significantly associated with mortality.34
Spontaneous ascitic infection (SAI) is defined as an ascitic fluid infection without an obvious intra-abdominal contiguous source of infection and is one of the most common infections in patients with cirrhosis.5 Patients with SAI can be classified into two groups: 1) Culture-negative neutrocytic ascites is diagnosed based on an ascitic fluid polymorphonuclear leukocyte (PMN) count ≥250/mm3 with a negative culture.6 For these patients, antibiotic treatment is based on the physician's experience. 2) Culture-positive SAI includes spontaneous bacterial peritonitis (SBP) and bacterascites. The prognosis and severity of liver insufficiency in patients with SBP and bacterascites are highly comparable, and the 30-day mortality rates of these two types of patients are reported as 31.5% and 32%, respectively.78
Early SAI diagnosis contributes to effective antibiotic therapy and improved survival.9 However, successful empirical antibiotic therapy must be based on local epidemiologic data. Previous studies have reported that gram-negative bacteria (GNB), mainly Enterobacteriaceae, are the major causative organisms of ascites.10 While third-generation cephalosporins have been used as the first-line treatment for SBP for several years,11 recently, an increase in multidrug-resistant (MDR) agents, such as extended spectrum β-lactamase (ESBL)-producing Enterobacteriaceae, have been observed in healthcare-associated and nosocomial infections, leading to failure of antibiotic strategies based on third-generation cephalosporins or quinolones and poor outcomes.12 Therefore, the European Association for the Study of the Liver (EASL) lately updated their recommendations of empirical antibiotic therapy for patients with SBP.13 However, because of various antibiotic prescription patterns in different regions and microbiological changes over time, the prevalence of antibiotic-resistant pathogens and the pathogen spectrum substantially differ geographically,314 and more evidence is required to support the application of empirical antibiotic management based on the EASL guidelines for cirrhotic patients with SBP to other regions. Thus, further studies with a larger sample size on bacteriological and drug resistance of culture-positive SAI are extremely urgent.
Cirrhotic patients with SBP are nearly 1.5-fold more likely to die within 28 days than those with non-SBP infection.15 Two epidemiological studies of SBP have shown that delay in diagnostic paracentesis and inadequate treatment were independent predictors of mortality associated with SBP.1617 However, few studies have evaluated the specific risk factors for SAI mortality in patients with culture-positive acute decompensated cirrhosis.
Therefore, this study aimed to assess possible changes in the pathogen spectrum and in drug resistance in patients with acute decompensated cirrhosis with culture-positive SAI based on site of infection acquisition and to identify independent risk factors of 28-day mortality after the first culture-positive SAI episode.
MATERIALS AND METHODS
Study design
We retrospectively studied patients admitted to 11 different teaching hospitals diagnosed with acute decompensated cirrhosis with culture-positive SAI from January 1, 2012 to May 30, 2018. The clinical history, physical examination, and laboratory and microbiological results were recorded in a pre-established electronic chart. For patients who presented with multiple culture-positive SAI during the study period, only the first episode was considered for analysis. The study was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology, and the ethical committees of each center (IORG No: IORG0003571).
Definitions
Diagnosis of liver cirrhosis was established by ultrasonographic findings, CT, MRI, and biopsy.12 Acute decompensation was defined as acute development of one or more major complications of liver disease, including acute development of large ascites (within less than 2 weeks; ultrasound ascites volume ≥150 mL), acute hepatic encephalopathy, acute gastrointestinal hemorrhage, and bacterial infection.4 Definition of organ failure was based on the chronic liver failure consortium organ failure score.4 SAI was classified as nosocomial if the infection was diagnosed beyond 48 h of admission; as healthcare-associated if diagnosis was made within 48 h of admission in patients requiring hospitalization for at least 2 days or paying more than two visits to the emergency department in the previous 90 days prior to infection or receiving chemotherapy/hemodialysis in the previous 30 days preceding the infection; and as community-acquired in all other cases.18 SBP was defined as an ascitic fluid PMN count ≥250/mm3 with a positive culture result. Bacterascites was defined as a positive bacterial culture with ascitic fluid PMN count <250/mm3. Definitions of blood stream infections, urinary tract infections, and skin and soft tissue infections were based on other studies.19 Resistant microorganisms were defined as MDR if they demonstrated non-susceptibility to at least one agent in three and as extensively drug resistant (XDR) in case of non-susceptibility to at least one agent in all but two or fewer antimicrobial categories.20
Microbiology
Identification and susceptibility tests of the isolated pathogens were carried out using the Vitek 2 automated system (BioMerieux, Craponne, France). All antibiotic susceptibilities were tested according to the Clinical and Laboratory Standard Institute guidelines.21 Results of the antimicrobial susceptibility tests were available within 48–72 h after the ascitic fluid culture showed positive results.
Statistical analysis
Categorical variables are presented as frequencies or percentages and were tested for significance with χ2 or Fisher's exact test. Parametric quantitative variables are presented as means±standard deviation and were tested for significance with Student's t-test. Non-parametric quantitative variables are presented as median and interquartile ranges and were tested for significance with the Mann-Whitney U or Kruskal-Wallis test. To identify independent risk factors for 28-day mortality, a Cox proportional hazards regression model was applied. Variables showing a statistically significant association with the outcome in univariate analysis (p<0.1) were entered into multivariate analysis using stepwise backward selection (entry p<0.05; drop p>0.1) based on likelihood ratios for entering and dropping variables. In all statistical analyses, p values <0.05 were considered statistically significant. Analyses were performed using SPSS statistical software, version 23.0 for Macintosh (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics
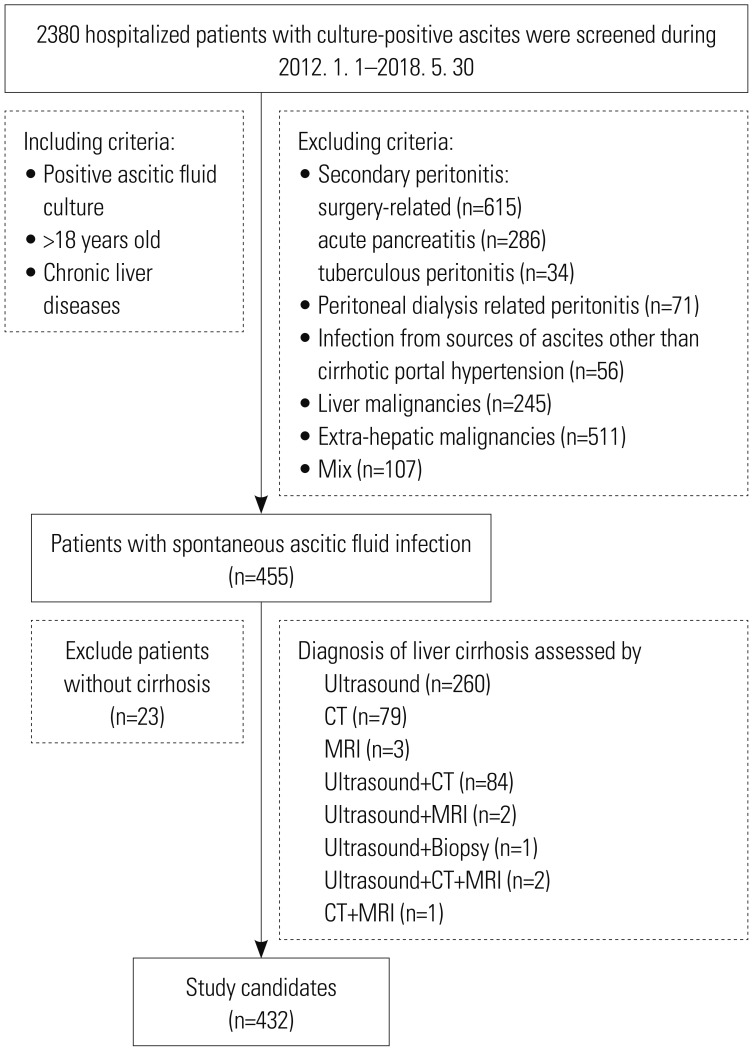
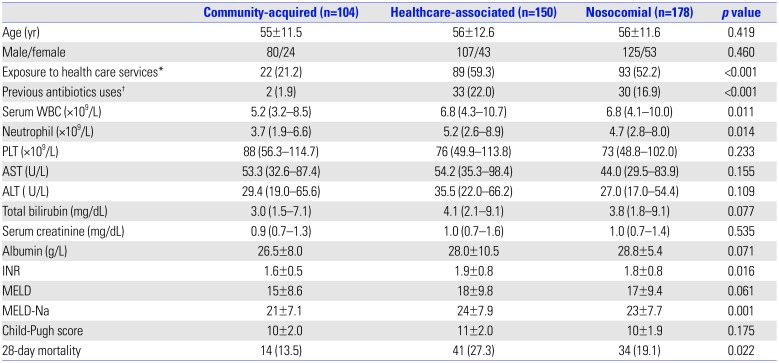
A total of 2380 hospitalized patients with all culture-positive ascites were screened from 11 different teaching hospitals between 2012 and 2018. Only 432 SAI episodes were identified in patients with culture-positive acute decompensated cirrhosis and enrolled in this study. The flowchart of patient enrollment is shown in Fig. 1. Based on the infectious sources, cirrhotic patients with SAI were classified as community-acquired (104/432, 24.1%), healthcare-associated (150/432, 34.7%), and nosocomial (178/432, 41.2%). Health care services and previous antibiotics use were more common in patients with healthcare-associated and nosocomial infections than in those with community-acquired infections (p<0.001). Serum white blood cell (WBC) counts, neutrophil counts, international normalized ratios (INR), and Model for End-Stage Liver Disease Sodium (MELD-Na) scores were higher in patients with healthcare-associated and nosocomial infections than in those with community-acquired infections (p<0.05). In these patients, 28-day mortality rates in patients with community-acquired, healthcare-associated, and nosocomial infections were 13.5, 27.3, and 19.1%, respectively (p=0.022) (Table 1).
Microorganism characteristics
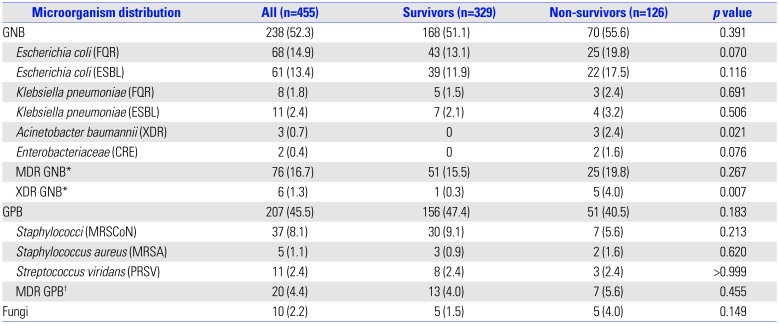
A total of 455 strains were isolated from the 432 ascitic fluid specimens: 52.3% were GNB, 45.5% gram-positive bacteria (GPB), and 2.2% fungi. The prevalence of GPB infections was significantly higher than GNB infections in patients with HBV-related cirrhosis (p=0.019). A tendency toward a higher mortality was observed in patients with GNB infections than in those with GPB infections during hospitalization; however, no difference was observed in 28-day mortality between the two groups (p=0.406) (Supplementary Table 1, only online). GPB infections increased from 37.2% to 54.3%, whereas GNB infections decreased from 60.7% to 43.4% between 2012–2015 and 2016–2018. Fungi were isolated almost equally in the two intervals. We also assessed the trends of ESBL-producing Escherichia coli and Klebsiella pneumoniae, fluoroquinolone-resistant (FQR) E. coli and K. pneumoniae, methicillin-resistant Staphylococcus aureus (MRSA), and penicillin-resistant Streptococcus viridans (PRSV). Results showed that the percentage of MRSA increased from 0.4% to 0.7%, while ESBL-producing and FQR pathogens (E. coli and K. pneumoniae) decreased from 10.8% and 11.6% to 5.0% and 5.0%, respectively. The prevalence of PRSV in the two intervals was almost the same (Fig. 2).
GNB infections were classified as MDR and XDR in 16.7% (76/455) and 1.3% (6/455), respectively, and MDR GPB infections comprised 4.4% (20/455). No pan-drug resistant GNB and XDR GPB were identified during the study. XDR GNB infections were significantly and positively correlated with non-survivors (p=0.007). Similarly, MDR organisms were isolated more frequently from non-survivor groups with GNB (p=0.267) and GPB (p=0.455) infections (Table 2).
We further investigated the distributions of GNB and GPB between SBP and bacterascites groups. The results showed that GNB were the major pathogens in the SBP group (71.6%), whereas GPB were predominant in the bacterascites group (57.3%), and the differences in GNB or GPB distributions between them were statistically significant (p<0.001). The prevalence of MDR/XDR strains in GNB infections was much higher in the SBP group than in the bacterascites group (p=0.002). Interestingly, in patients with bacterascites, the percentage of Enterococcus spp. isolates were higher in nosocomial infections than in healthcare-associated and in community-acquired infections. However, Streptococcus spp. were detected more common in the community-acquired subgroup than in the healthcare-associated and nosocomial subgroups (p<0.05). Other bacteria distributions among the three subgroups were not statistical significance (Supplementary Table 2, only online).
The majority of GNB infections were caused by E. coli (26.2%) and by K. pneumoniae (7.5%). GPB included Staphylococcus spp. (17.1%), Enterococcus spp. (12.7%), Streptococcus spp. (10.1%), and others. Candida species accounted for 2.0% (9/455) of all strains (Supplementary Table 3, only online). ESBL-producing E. coli and K. pneumoniae were isolated in 72 (15.8%) out of 455 strains and presented less frequently in patients with community-acquired infections (12.1%) than in those with healthcare-associated (17.2%) and nosocomial infections (16.8%). Carbapenem-resistant GNB infections were more frequent in the healthcare-associated and nosocomial groups than in the community-acquired group (p=0.005) (Supplementary Table 4, only online).
Antibiotic susceptibility analysis
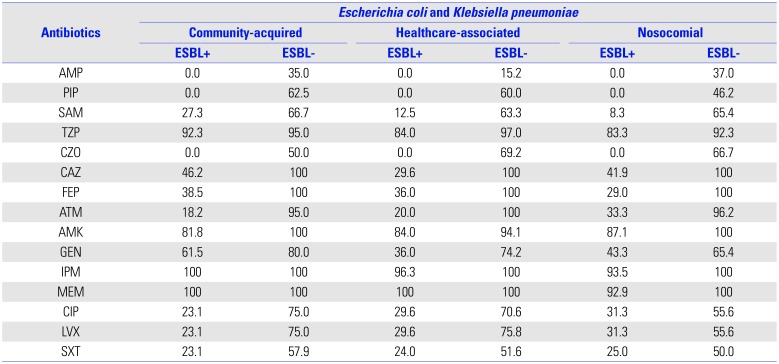
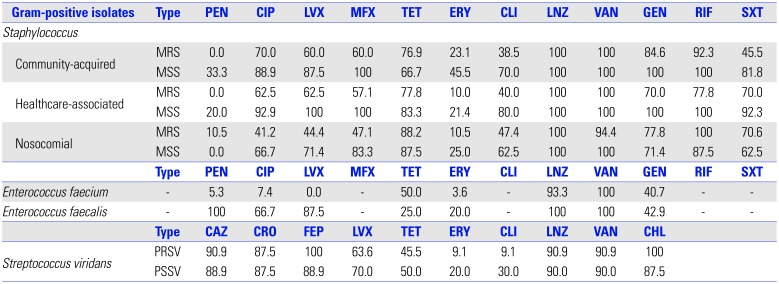
Antibiotic susceptibility of GNB, including E. coli and K. pneumoniae, was investigated with respect to susceptibility to 18 different antibiotics covering seven main groups. The E. coli and K. pneumoniae isolates were highly sensitive to meropenem, imipenem, piperacillin/tazobactam, and amikacin, regardless of their ESBL status. Similar results were observed among community-acquired, healthcare-associated, and nosocomial infections; however, non-ESBL-producing agents also showed high sensitivity to third-generation cephalosporins and aztreonam (Table 3).
Antibiotic susceptibility of GPB, including Staphylococcus, Streptococcus viridans, and Enterococcus, was determined. The susceptibility of MRSA to fluoroquinolone antibiotics, erythromycin, clindamycin, sulfamethoxazole, and trimethoprim was weaker than that in methicillin-sensitive isolates. However, methicillin-resistant isolates showed good sensitivity to vancomycin and linezolid among community-acquired, healthcare-associated, and nosocomial infections. PRSV were highly susceptible to other antimicrobials, except for erythromycin, clindamycin, tetracycline, and levofloxacin. In addition, similar to other GPB, both Enterococcus faecium and Enterococcus faecalis were also sensitive to vancomycin and linezolid (Table 4).
Predictors of 28-day mortality in patients with acute decompensated cirrhosis with culture-positive SAI
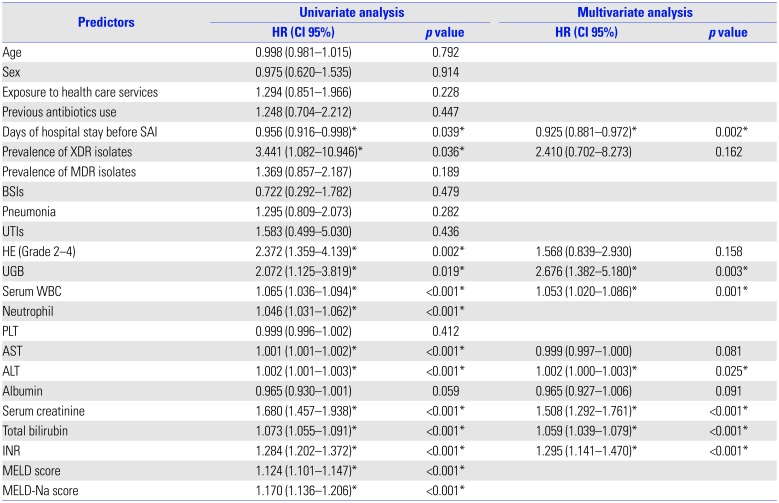
decompensated cirrhosis with culture-positive SAI In univariate analysis, days of hospital stay before culture-positive SAI, prevalence of XDR isolates, severe hepatic encephalopathy (HE) (grade 2–4), upper gastrointestinal bleeding (UGB), WBC count, neutrophil count, aspartate transaminase (AST), alanine aminotransferase (ALT), serum creatinine, total bilirubin, INR, and Model for End-Stage Liver Disease score (MELD) and MELD-Na scores were significantly correlated with outcomes of patients with acute decompensated cirrhosis who developed culture-positive SAI. Multivariate analysis demonstrated that mortality variables were independently associated with days of hospital stay before culture-positive SAI, UGB, WBC count, INR, ALT, serum creatinine, and total bilirubin (Table 5).
DISCUSSION
The prevalence of MDR pathogens and antibiotic strategies were identified in patients with acute decompensated cirrhosis with culture-positive SAI in our multicenter retrospective study. To the best of our knowledge, this is the most comprehensive and largest contemporary epidemiological survey for this group of patients in China.
Our study indicated that GNB remain the primary pathogens; meanwhile, an increasing prevalence of GPB in SAI was observed. E. coli and K. pneumoniae represented the highest GNB infections, and Staphylococcus was the dominant GPB. These results were different from several single-center studies, which demonstrated Streptococcus spp. and Enterococcus spp. as the most frequently isolated GPB.2223 Historically, GNB have been isolated in the majority of patients with HBV-related acute decompensated cirrhosis complicated with SAI.2224 However, in this study, GPB were found to be the predominant pathogens. Particularly, an increasing rate of infections caused by GPB and resistant microorganisms had been demonstrated in culture-positive cases of SAI.812 The prevalence of GPB in our study was lower than that reported (55%) in a recent study;12 however, the increasing trend of GPB infections in culture-positive SAI patients with acute decompensated cirrhosis remains obvious and may be attributed to an exposure to healthcare services and previous antibiotics uses before admission, especially a widespread use of prophylactic antibiotics against GNB in patients with culture-positive SAI. Thus, antibiotics used to manage GPB infections should also be considered in future empirical therapies.
An increase in MDR and XDR bacteria in patients with SBP has been reported.25 As shown in our study, the prevalence of MDR and/or XDR pathogens in patients with culture-positive SBP or bacterascites were 29.6% and 18.2%, respectively. These percentages were higher than those reported among patients with SBP,192627 but lower than that reported (25%) among patients with bacterascites by Oey, et al.8 These results emphasized an urgent need to control the increase of drug resistant bacteria in patients with SAI. Additionally, our results indicated that MDR organisms are more prevalent in nosocomial and healthcare-associated patients with SAI than in community-acquired patients. The prevalence of ESBL-producing organisms in community-acquired infections was much higher than that reported,28 which may be attributed to the extensive use of third-generation cephalosporins in China. Furthermore, patients with healthcare-associated infections had a higher 28-day mortality than patients with community-acquired SAI. Thus, attention should be paid to patients with healthcare-associated and nosocomial SAI.
Third-generation cephalosporins, piperacillin-tazobactam, and carbapenems are recommended in the recent EASL guidelines for the treatment of patients with decompensated cirrhosis with SBP.13 However, the increase in XDR and MDR strains challenge the recommended antibiotics from the guidelines. Our findings showed that ESBL-producing E. coli and K. pneumoniae accounted for 15.8%. A significant number of ESBL-producing strains exhibited low sensitivity to third-generation cephalosporins and/or quinolones, especially pathogens in community-acquired infections. In the present study, ceftazidime, cefepime, aztreonam, and amikacin were recommended for first-line antibiotic treatment for non-MDR GNB infections. Considering the high mortality, piperacillin/tazobactam and carbapenems should be considered for MDR GNB infections in community-acquired SAI and healthcare-associated or nosocomial SAI, respectively, which is in accordance with EASL guidelines. However, unlike the ESAL guidelines that recommend carbapenems combined with glycopeptides or daptomycin or linezolid, vancomycin or linezolid should be considered for GPB infections, regardless of drug-resistance status and type of infections.
Previous studies have reported on independent risk factors in patients with SBP;129 however, no study has evaluated the specific risk factors for culture-positive SAI in patients with acute decompensated cirrhosis. In our series, severe HE, UGB, WBC count, serum creatinine, and INR were independently associated with 28-day all-cause mortality, and these results emphasized the importance of the timely treatment in complications. More importantly, reducing days of hospital stay before SAI, which meant early diagnosis and treatment, was also closely related to 28-day mortality.
Our study had several limitations. First, our study aimed to analyze the microbiological characteristics of patients with culture-positive SAI, thus culture-negative patients with SAI were excluded from our study. Second, we included Staphylococcus because this strain could be isolated from both the blood and ascitic fluid samples obtained from one patient. Furthermore, exogenous contamination related to invasive procedures, such as traumatic paracentesis, was unlikely to account for any of the culture-positive SAI cases, and no effective methods to distinguish contaminants from pathogens because SAI may be caused by Staphylococcus with low virulence in susceptible patients. Finally, a few clinical results, such as AST and ALT, were missing in patient records, but did not significantly impact the results.
In conclusion, GNB were the most common pathogens, with a growing proportion of SAIs caused by GPB and MDR/XDR GNB. Healthcare-associated and nosocomial infections showed a high prevalence of MDR organisms and exhibited differences in 28-day mortality, compared to community-acquired infections. Carbapenems, piperacillin/tazobactam, and amikacin were more suitable for the treatment of culture-positive SAI with GNB infections, whereas vancomycin and linezolid were the best choices for GPB infections. All identified independent risk factors could be utilized to develop a multiple clinical risk evaluation system to help clinicians identify the highest-risk subsets of patients.

 XML Download
XML Download