

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Fractional flow reserve (FFR) is currently the gold standard for detecting lesion-specific myocardial ischemia.123 Prior studies have demonstrated that ischemia-causing lesions detected using FFR portend poor prognosis.1 Furthermore, FFR-guided percutaneous coronary intervention (PCI) has shown survival benefits over invasive coronary angiography (ICA)-guided PCI alone.23
Coronary computed tomography angiography (CTA) is a noninvasive method for accurate detection and exclusion of high-grade coronary stenoses, hence it may serve as a gatekeeper for invasive catheterization.4567 However, CTA tends to overestimate the severity of coronary artery stenosis, resulting in low specificity and positive predictive values (PPVs).89
Non-invasive CTA-derived FFR, which applies computational fluid dynamics (CFD) onto three-dimensional (3D) coronary lumen geometry derived from CTA, has demonstrated high diagnostic accuracy, as well as improved specificity and PPVs, according to three prospective multicenter trials.101112 Ultimately, this novel technique allows for comprehensive anatomic and physiologic diagnosis of coronary artery disease (CAD).13 However, current non-invasive FFR techniques have several major limitations when applied to day-to-day clinical practice: The required simulation has to be performed outside of the hospital because it necessitates a supercomputer, therefore requiring transfer of patient data potentially leading to exposure of personal patient information.14 Furthermore, the processing time can take several hours, and the service can be expensive.1415161718
Therefore, we aimed to develop a new non-invasive on-site vFFR computing system derived from CTA that would allow for instantaneous utilization in clinical practice that is timelier and cost efficient. This technique uses a novel parallel computing method with a completely automated lumen segmentation algorithm without the need for a supercomputer.
MATERIALS AND METHODS
Study population
We consecutively enrolled clinically stable adult patients from September 2015 to February 2016 at Severance Cardiovascular Hospital who underwent clinically indicated ICA within 30 days following CTA with no intervening coronary events. Institutional Review Board (Severance Hospital, IRB Number 1-2017-0031) approval was obtained for this retrospective study and informed consent was waived. Patients were excluded if they met any of the following criteria: history of coronary artery bypass graft surgery; prior PCI with suspected instent restenosis; old myocardial infarction; complex congenital heart disease; prior pacemaker or defibrillator; prosthetic heart valve; significant arrhythmia; body mass index greater than 40; or evidence of active clinical instability or life-threatening disease.
CTA data acquisition
CTA images were acquired using two 64-slice multi-detector row computed tomography systems (Somatom Sensation 64, Siemens Medical Solutions, Forchheim, Germany) with prospective or retrospective electrocardiographic gating. All patients with a heart rate of 65 beats per minute or higher received 100 mg of atenolol orally prior to the CT, unless contraindicated. In addition, all patients received a 0.3-mg sublingual dose of nitroglycerin just prior to scanning, unless contraindicated. Bolus tracking was used for contrast injection. The scan parameters for the machines were as follows: 64×0.6-mm section collimation and a 330-ms rotation time. Depending on body habitus, tube voltages and currents were adjusted as follows: 80, 100, or 120 kVp and 150–500 mAs. The median radiation dose was 3.92 mSv [95% confidence interval (CI) 2.56 to 5.65], with 9 patients receiving less than 1 mSv.
Invasive FFR measurement
Fractional flow reserve was measured in vessels deemed clinically indicated for evaluation. After administration of nitroglycerin, a pressure-monitoring guidewire was advanced distal to a lesion. Hyperemia was induced by administration of intravenous or intracoronary adenosine at a rate of 140 mg/kg/min, and FFR was calculated by dividing the mean distal coronary pressure by the mean aortic pressure during hyperemia. FFR at a threshold of ≤0.80 or ≤0.75 were considered hemodynamically significant leading to ischemia.
Fully automated lumen segmentation algorithm
We reconstructed patient-specific coronary geometry automatically using in-house software on CTA images (Fig. 1A). The fully automatic segmentation was performed with the following four steps: at first, aorta and ostia were detected by our algorithm, which uses a Bayesian formulation in a pairwise fashion using anatomical and geometrical information.19 The detected points were used as seeds for coronary artery tracking. Second, the centerlines of the left and right coronary arteries (RCA) were extracted starting from the detected ostia by our vessel tracking method based on stochastic geometric processes using an active branch search.20 The tracking method could better find the branches, any stenotic lesions, and seemingly disconnected vessels that may be occluded by atherosclerotic plaque by modeling the statistical branch occurrence and the vessel disconnection. Third, luminal boundaries for all vessels were automatically delineated every cross-sectional plane based on the image gradient and prior CT information on the number of plaques. Finally, we generated the surface mesh of the coronary structure with the estimated luminal boundaries. The connections of bifurcated vessels were processed smoothly using a mesh merging method that merged the vessel mesh and the divaricating branch mesh.21
Computational fluid dynamics for vFFR
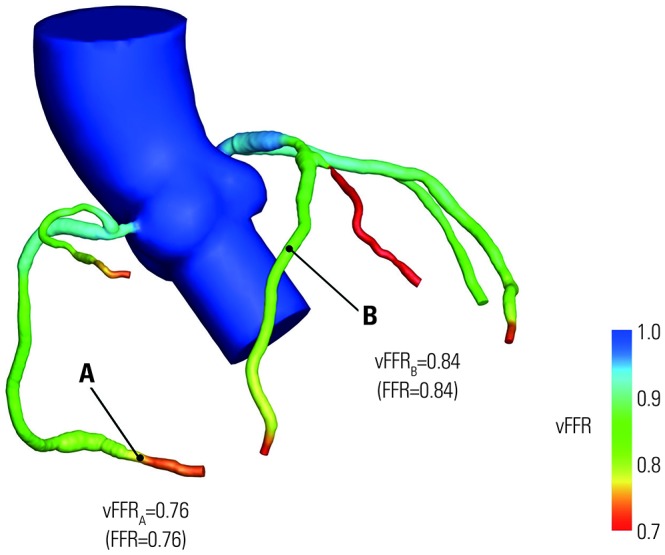
To calculate vFFR, 3D blood flow dynamics were simulated using the CFD technique for patient-specific coronary geometry (Fig. 1B). The continuity and Navier-Stokes equations for unsteady incompressible Newtonian fluid flow were solved with appropriate boundary conditions. A fully implicit four-step fractional method with a regular Crank-Nicolson scheme for time advancement and a P2P1 finite element method for spatial discretization were employed. In order to accommodate the specific time-varying pressure-flow characteristics of coronary flow, which is affected by intramyocardial pressure subject to cyclic contraction of the left ventricle and microcirculation in coronary distal networks, zero dimensional lumped parameter network (LPN) models were integrated into the 3D CFD model at all coronary outlets in a fully implicit manner. The patient-specific total resistances and capacitance for the distal coronary bed in a resting condition, as well as a hyperemic condition (i.e., the maximum flow condition resulting from the minimal microvascular resistance), were determined as described by Sankaran, et al.22 and Sharma, et al.23 The distribution of flow rates between left anterior descending artery (LAD) and left circumflex artery (LCX) was determined according to the total volume of the corresponding vessel tree. Flow division into further distal branches was approximated by allometric scaling laws based on the coronary lumen cross-sectional area.24 The aortic pressure and flow rate were acquired by solving the LPN models with constraints that matched the systolic and the diastolic blood pressure of the individual patients.
To expedite simulation time, a parallel computing procedure based on a domain decomposition method was applied (Fig. 1B).25 The P2P1 unstructured mesh of the whole computational domain was decomposed into multiple subdomains using a k-way partition method,26 and the computing work for each subdomain was equally distributed to corresponding processors. Simulations were carried out on a parallel cluster system (two nodes, 40 cores), where each node comprised two CPUs (E5-2680V2, 2.8 GHz, 25 MB L3 cache) and 64 GB RAM, with an Infiniband interconnect network between nodes.
Statistical analysis
Data are reported as a mean±SD for continuous variables and as proportions (%) for categorical variables. Pearson correlation coefficients using two-sided p-values, with p-values<0.05 considered statistically significant, and Fisher's Z transformation statistics were applied for comparing correlations. Bland–Altman plots with 95% CIs for correlations were calculated. FFRs were each dichotomized at a threshold of 0.80 and 0.75, with FFR values ≤0.80 and ≤0.75, respectively, considered hemodynamically significant and causal of ischemia. The diagnostic accuracy, sensitivity, specificity, PPV, and negative predictive value (NPV) between vFFR and FFR at 0.80 and 0.75 were presented as proportions and 95% CIs. The areas under receiver operating characteristic curves (AUC) were compared according to the method proposed by DeLong, et al.27 Statistical analyses were performed using Medcalc software (version 17.6; MedCalc Software, Mariakerke, Belgium).
RESULTS
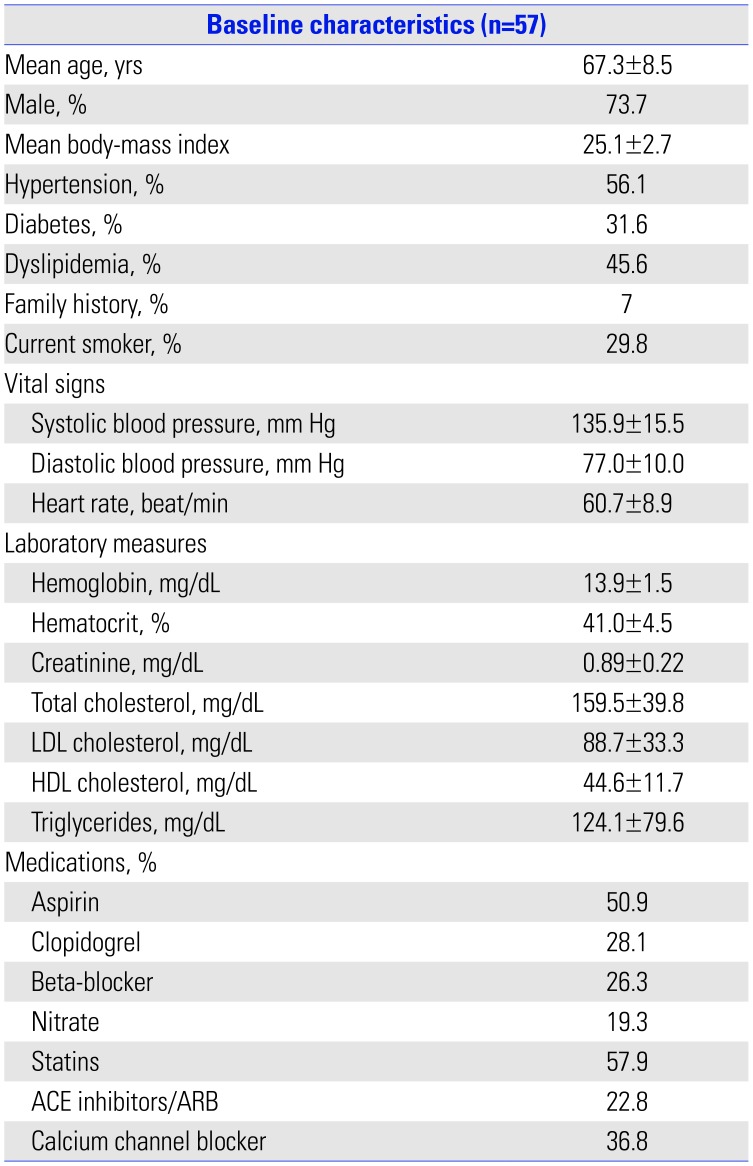
Three out of 60 patients analyzed (5%) were excluded based on failure of lumen segmentation due to severely calcified lesions or motion artifacts. We subsequently analyzed 100 lesions from 57 patients (42 men and 15 women, mean age: 67.3±8.5 years). Baseline patient characteristics are presented in Table 1. The lesions were primarily located in the LAD (47%), followed by the RCA (23%), LCX (18%), diagonal branch (DG, 5%), obtuse marginal branch (OM, 4%), left main (LM, 2%), and ramus intermedius (RI, 1%). The plaque composition profiles of the lesions were as follows: mixed plaque (59%), non-calcified plaques (29%), and calcified plaques (12%). Forty percent of plaques were located in the proximal segments of coronary arteries.
The average time for generating patient-specific 3D coronary geometry was 233 seconds (min=175 s, Q1=196 s, median=212 s, Q3=221 s, max=386 s). CFD simulations were carried out up to two cardiac cycles to damp initial transients and most runs were able to be completed within 20 minutes (average=514.7 s, min= 232 s, Q1=380 s, median=439 s, Q3=544 s, max=1370 s). The run time was highly dependent on the smoothness of coronary lumen surface and computational mesh quality. The representative simulation case of vFFR is shown in Fig. 2.
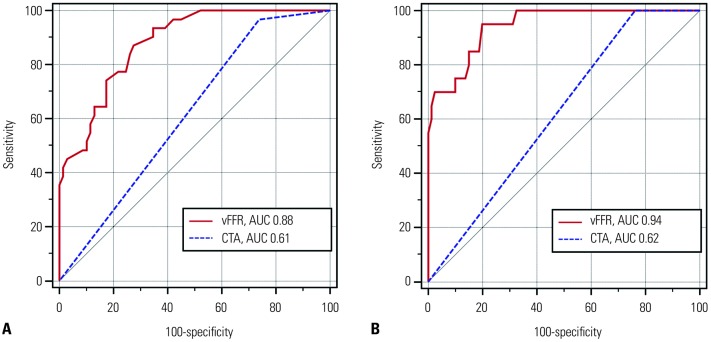
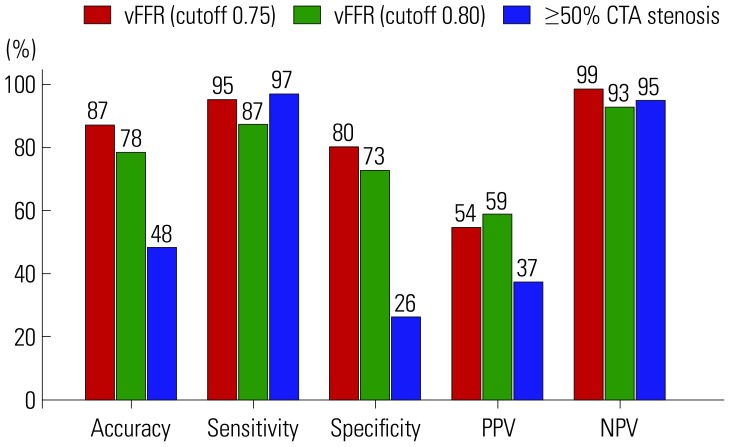
The correlation coefficient between vFFR and FFR was 0.75 (95% CI 0.65 to 0.83), and Bland-Altman analysis reavealed a mean bias of 0.005 (95% CI −0.011 to 0.021), with 95 % limits of agreement of −0.16 to 0.17 between vFFR and FFR (Fig. 3). Diagnostic performance was evaluated separately using FFR cutoffs of 0.80 and 0.75. The accuracy, sensitivity, specificity, PPV, and NPV when the FFR cutoff of 0.80 was used were 78.0% (95% CI 64.0–87.0), 87.1% (95% CI 70.2–96.4), 72.5% (95% CI 60.4–82.5), 58.7% (95% CI 48.6–68.1), and 92.6% (95% CI 83.2–96.9), respectively. In addition, the AUC value for vFFR was significantly higher [0.88 (95% CI 0.80–0.94) vs. 0.61 (95% CI 0.51–0.71)] than CTA ≥50% stenosis (Fig. 4A). Moreover, when a FFR cutoff of 0.75 was used the diagnostic performance significantly improved, with accuracy, sensitivity, specificity, PPV, and NPV of 87.0% (95% CI 77.0–95.7), 95.0% (95% CI 75.1–99.9), 80.0% (95% CI 69.6–88.1), 54.3% (95% CI 43.1–65.1), and 98.5% (95% CI 90.4–99.8), respectively. In addition, the AUC value for vFFR was excellent [0.94 (95% CI 0.88–0.98) vs. 0.62 (95% CI 0.52–0.71)], compared with CTA ≥50% stenosis (Fig. 4B). Fig. 5 shows the comparison of the diagnostic performances between vFFR and FFR at 0.8, between vFFR and FFR at 0.75, and between CTA ≥50% stenosis and FFR at 0.8.
The diagnostic performances according to vessel size were also evaluated by separating large vessels (n=70), such as the LM, LAD, and RCA, from small vessels (n=30), such as LCX, DG, OM, and RI. Large vessels showed higher accuracy than small vessels both with FFR cutoffs of 0.80 (80.5% vs. 73.3%) and 0.75 (88.9% vs. 83.3%).
DISCUSSION
In the present study, we developed a novel non-invasive CTA-derived on-site vFFR method and demonstrated its excellent correlation with invasively measured FFR. In addition, this method exhibited excellent diagnostic performance for detecting ischemia producing lesions, compared to invasive FFR as a reference standard. Furthermore, vFFR had significantly higher diagnostic performance and improved discriminatory power for the detection of lesion-specific ischemia, compared to obstructive (≥50%) CTA stenosis alone. Moreover, we also discovered that when an FFR cutoff of 0.75 was used, the diagnostic accuracy and discriminatory ability of vFFR for ischemia detection was greatly enhanced.
CTA is a robust noninvasive tool for ruling out obstructive or high-grade coronary artery stenosis, obviating unnecessary use of invasive catheterization.4567 On the other hand, CTA's tendency to overestimate coronary artery stenosis can lead to additional testing that is often unnecessary due to its low specificity and PPV for the detection of ischemia causing stenosis.89 Based on these limitations, FFR-CT was created, and several FFR-CT studies have shown great improvement in the diagnostic performance of ischemia detection by increasing specificity and PPV compared with other non-invasive imaging modalities, such as stress echocardiography, single photon emission computed tomography, or cardiac magnetic resonance.10111228 However, FFR-CT has several major limitations, including high addon costs (approximately $1500), potential risk of exposure of personal patient information based on need for off-site post-processing, and considerable processing time leading to a potential delay in patient care.1415161718 Furthermore, a recently introduced on-site CTA derived cFFR (Siemens cFFR, version 1.4; Siemens Healthcare, Forchheim, Germany) has been shown to have high diagnostic accuracy.29 However, this method requires a semi-automated coronary lumen segmentation process (−60 minutes per case), which might be a considerable limitation when considering its application to daily practice.30
On the other hand, the vFFR does not require the use of a supercomputer to compute coronary flow. Instead, the implementation of on-site CFD calculation is done using a novel parallel computing method. This method is based on a cluster with 40 cores, which then decomposes the domain into 40 subdomains and assigns a sub-domain to each computing core. Additionally, the coronary lumen segmentation and 3D reconstruction is conducted by a completely automated algorithm without any operator intervention, thus making the results available within 30 minutes, including segmentation and CFD calculation. In addition, the median radiation dose of CTA in this study was 3.92 mSv (95% CI 2.56 to 5.65), and 9 patients (16%) received less than 1 mSv (using 80 kVp along prospective electrocardiogram gating). To date, several studies have shown that CTA is able to visualize not only stenosis severity but also adverse plaque characteristics, which are closely related with future adverse events, in addition to lesion specific ischemia.3132333435 For example, Gaur, et al.36 demonstrated that adverse plaque characteristics provide additive valve in FFR-CT for prediction of ischemia. Based on these findings, CTA with the aid of on-site vFFR could potentially provide a comprehensive evaluation of coronary stenosis and adverse plaque features, as well as assessment of hemodynamically significant CAD, which could lead to a true “one-stop shop” with sub milli-Sievert radiation exposure.
This study is not without limitations. First, this was a retrospective pioneering study with a limited number of cases. Presently, vFFR requires further well-powered validation in prospective multicenter trials. Second, the vessels interrogated by FFR were limited to those clinically indicated, introducing potential selection bias. Lastly, we were unable to evaluate 5% (3/60) of patients in whom vessels were heavily calcified or there were severe motion artifacts that made CTA-derived FFR methods impossible. CTA image quality was also an important factor for successful simulation in this study, which is the case in most other imaging studies.3738 Recently developed high spatial resolution and wider CTA detector coverage may provide a solution for this issue in the near future.39
In conclusion, a novel on-site vFFR computing system employing a fully automated segmentation algorithm using a parallel computation method showed excellent diagnostic performance for the detection of lesion-specific ischemia and was significantly faster and cheaper.


 XML Download
XML Download