

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most commonly sustained cardiac arrhythmia among the general population12345 and is related to a 5-fold increase in stroke risk.256 Preventing stroke is the principal management in AF patients.7 Warfarin has been used for several decades as the mainstay of oral anticoagulants (OACs) and to reduce the relative risk of stroke in AF patients by 64% and all-cause mortality by 26%, compared to that in control groups.89 Direct oral anticoagulants (DOACs) have been shown to be as safe and effective as warfarin in large randomized controlled trials,10 with lower incidences of intracranial hemorrhage. Indeed, DOACs also have several potential advantages over warfarin, including no need for routine coagulation monitoring11 and fewer drug–drug and food–drug interactions.12 Current guidelines suggest preferential use of DOACs in patients with nonvalvular AF and risk of thromboembolic events.51314 Nevertheless, both economical and medical reasons have limited the use of DOAC.
Recent guidelines for AF patients undergoing percutaneous coronary intervention or acute coronary syndrome recommend short-term use of triple antithrombotic agents (TAT; OAC+P2Y12 inhibitor+aspirin), 1-year dual antithrombotic agents (DAT, OAC+P2Y12 inhibitor or aspirin), and OAC alone for 1 year after percutaneous coronary intervention. However, the usage of TAT, DAT, or dual antiplatelet agents (DAP) is popular in many patients with AF.1516
Large cohort data showing contemporary anticoagulant usage patterns are still lacking. This study examined the antithrombotic agent usage patterns and identified factors related to the use of DOACs or antiplatelet agents in a modern, prospective, multicenter AF registry.
Go to : 
MATERIALS AND METHODS
Study design and centers
The study design of the COmparison study of Drugs for symptom control and complication prEvention of Atrial Fibrillation (CODE-AF) has been described in a previous study.17 Briefly, the CODE-AF registry is a prospective, multicenter, observational study of AF patients >18 years at 18 tertiary centers, including all geographical regions of Korea.17 The study enrollment period was from June 2016 to May 2019.
The primary aim of the CODE-AF registry was to assess the outcomes of medical treatments, such as rate or rhythm control treatments, and anticoagulation.17 The secondary aim of the registry was to document the clinical epidemiology of AF patients and the diagnostic and therapeutic courses, such as the organization of AF management programs, applied in these patients and their clinical outcomes.17 The Korea Heart Rhythm Society designed and coordinated this registry.17 Data are entered in a common electronic database that limits inconsistencies and errors and provides online help for key variables.17 The study provided informed consent for inclusion in all patients and was approved by the ethics committee of each center. This study was registered at ClinicalTrials.gov (NCT02786095). The study was approved by the ethics committee of Severance Hospital (4-2016-0105).
Patients
Over the inclusion period, each center enrolled patients with AF attending the outpatient clinic and those hospitalized over the same period for AF. This registry excluded patients with moderate to severe mitral stenosis and a history of valve surgery, which are indications of warfarin use. Also, patients with deep vein thrombosis or pulmonary embolism were not included in the registry. From 10779 enrolled patients in the registry, patients with missing warfarin or DOAC usage data (n= 47) and patients who switched OAC from warfarin to DOAC or vice versa (n=203) were excluded. After exclusion, a total of 10529 patients were analyzed. Data collection was performed according to the same criteria and was usually performed by personnel who were not going to be associated with clinical activity in the project. Congestive heart failure/left ventricular dysfunction, hypertension, age ≥75 years (doubled), diabetes, stroke (doubled)–vascular disease, 65–74 years of age, and sex category (female) [CHA2DS2-VASc] score and hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio, older adult, and drugs/alcohol concomitantly (HAS-BLED) score were calculated for all patients with non-valvular AF. A follow-up visit was scheduled every 6 months, either by personal interview or telephone contact.
Anticoagulation
Patients with low stroke risk generally are not recommended antithrombotic therapy, while patients with high stroke risk (i.e., CHA2DS2-VASc score ≥1 for men and ≥2 for women) are likely to benefit from anticoagulation therapy.51318 However, because the recommendation for patients with intermediate stroke risk remains controversial, guideline adherence was not evaluated in these patients.51318
Statistical analysis
All continuous variables were normally distributed, expressed as a mean±SD, and compared using Student's t-test. Categorical variables are expressed as numbers (percentages) and were compared between patients under warfarin or DOAC treatment using a χ-squared test or Fisher exact test, as appropriate. Multivariable logistic regression was performed to identify factors associated with warfarin versus DOAC. The outcome of interest was binary (warfarin or DOAC; OAC or non-OAC; OAC with or without antiplatelet agent). Logistic regression was performed by a backward conditional test. The significance threshold for inclusion in the model was 0.05. Candidate variables were chosen from previous studies and experience. Results are presented as an odds ratio (OR) and 95% confidence interval (CI). All p-values were two tailed, and values less than 0.05 were considered statistically significant. All statistical analyses were performed using the SPSS software (version 25.0; IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
Baseline characteristics
A total of 10529 patients with AF were analyzed. The mean age was 66.9±14.4 years, and 6833 (64.9%) of the patients were men. Mean CHA2DS2-VASc and HAS-BLED scores were 2.6±1.7 and 1.8±1.1, respectively. OAC was used in 7409 (70.4%) patients: warfarin in 1556 (14.8%); and DOAC in 5853 (55.6%). Among patients with DOAC use, 1400 (23.9%) patients were treated with dabigatran, 1310 (22.4%) with rivaroxaban, 2086 (35.6%) with apixaban, and 1080 (18.5%) with edoxaban.
Table 1 shows the comparison of baseline characteristics stratified by anticoagulant treatment. Compared to patients using warfarin, those using DOAC were older and had higher rates of arterial hypertension, diabetes mellitus, cancer, and a history of cerebrovascular disease. Mean CHA2DS2-VASc score was 2.6±1.7 in patients treated with warfarin and 3.1±1.5 in patients treated with DOAC (p<0.001).
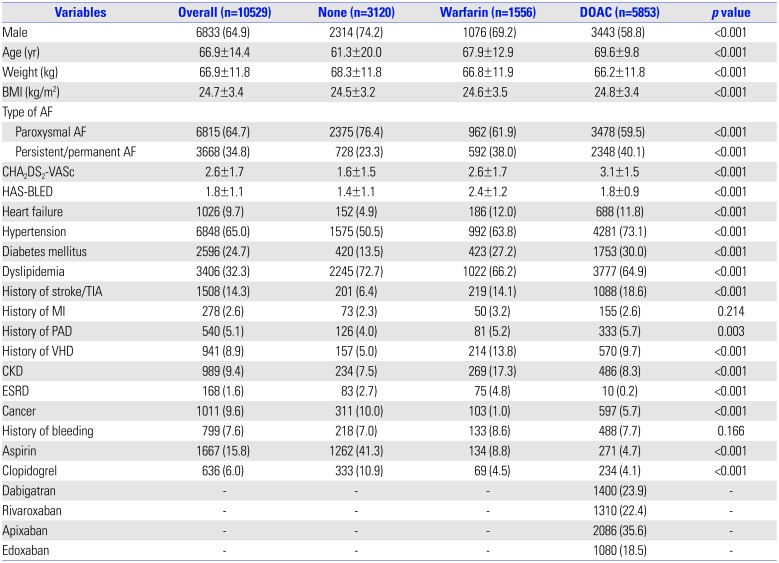
Table 1
Baseline Characteristics of Patients
AF, atrial fibrillation; BMI, body mass index; CHA2DS2-VASc, congestive heart failure, hypertension, age 75 years or older, diabetes mellitus, previous stroke/transient ischemic attack, vascular disease, age 65 to 74 years, female; HAS-BLED, hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio, elderly, concomitant drugs/alcohol; TIA, transient ischemic attack; MI, myocardial infarct; PAD, peripheral artery disease; VHD, valvular heart disease; CKD, chronic kidney disease; ESRD, end-stage renal disease.
Data are presented as mean±SD or number (%).
![]()
Anticoagulant treatment strategies according to stroke and bleeding risk
Fig. 1 shows anticoagulant usage patterns in different CHA2DS2-VASc score groups. In patients with high stroke risk (CHA2DS2-VASc ≥2), OAC was used in 83.2%, including 68.8% who received DOAC. In patients with low to intermediate stroke risk (CHA2DS2-VASc <2), OAC was used in 37.9%, including 22.0% who received DOAC. Patients at high stroke risk were more prone to be treated with DOAC than warfarin, compared to the low- and intermediate-risk groups (p<0.001).
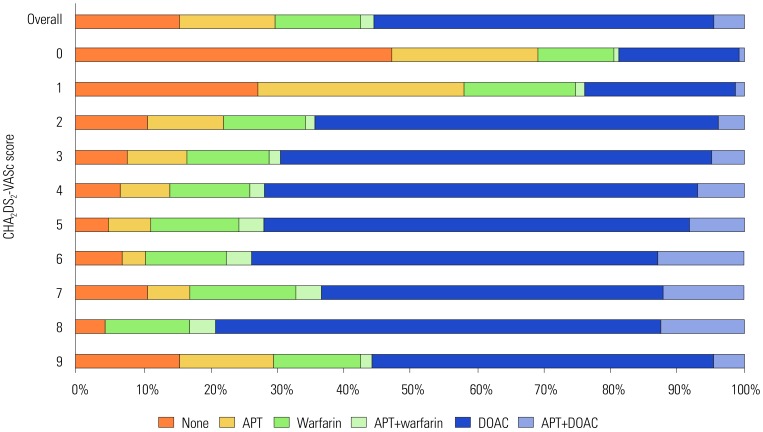
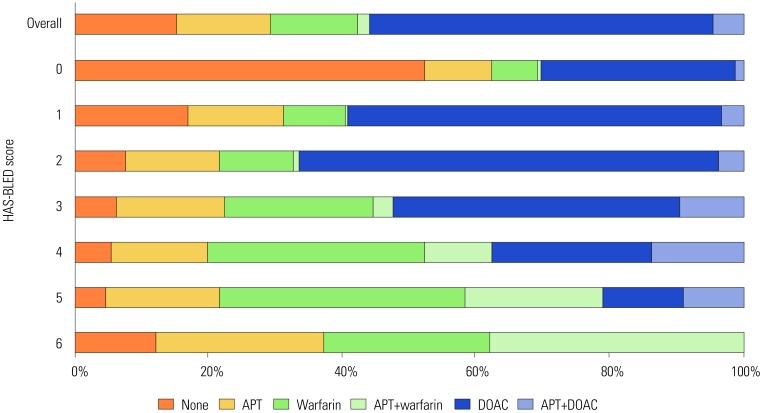
Fig. 2 shows anticoagulant usage patterns according to HAS-BLED score grouping. Mean HAS-BLED score was 2.4±1.2 in patients treated with warfarin and 1.8±0.9 in patients under DOAC treatment. In patients with low and intermediate bleeding risk (HAS-BLED score=0–2), OAC was used in 68.2%, including 57.9% who received DOAC. In patients with high bleeding risk (HAS-BLED score ≥3), OAC was used in 77.9%, including 48.1% who received DOAC. Patients at low and intermediate risk of bleeding were more prone to be treated with DOAC than those at high risk of bleeding (p<0.001).
OAC vs. non-OAC treatment in all patients
In 7547 AF patients with high stroke risk, OAC was not used in 16.8%, and antiplatelet was used in 8.8% among them. Aspirin, P2Y12 inhibitor, and aspirin plus P2Y12 inhibitor were used in 6.1, 1.7, and 1.0% patients, respectively. Fig. 3 shows variables associated with OAC or non-OAC treatment in the CHA2DS2-VASc score ≥2 groups. Compared to variables favoring non-OAC treatment, variables favoring OAC treatment were factors for calculating CHA2DS2-VASc score: age ≥75 (OR 1.60; 95% CI: 1.40–1.83), history of valvular heart disease (OR 1.28; 95% CI: 1.03–1.59), history of stroke/TIA (OR 1.51; 95% CI: 1.28–1.79), heart failure (OR 1.53; 95% CI: 1.24–1.88), and diabetes mellitus (OR 1.42; 95% CI: 1.23–1.63).
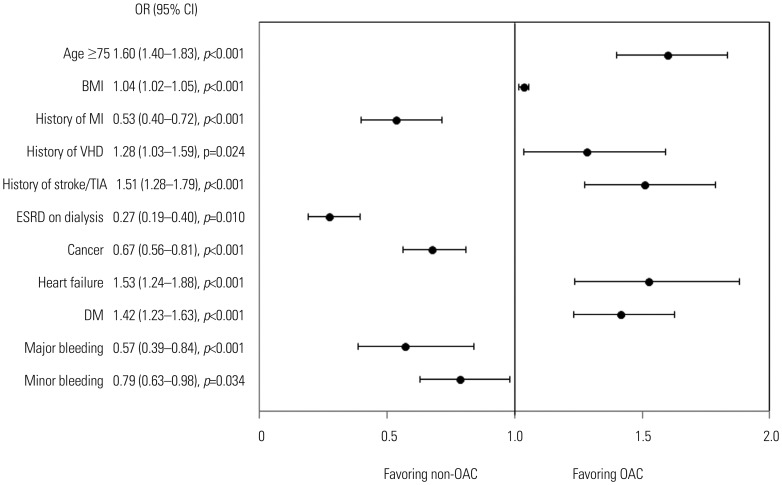 | Fig. 3Factors favoring OAC or non-OAC treatment in patients with CHA2DS2-VASc ≥2. OAC, oral anticoagulant; BMI, body mass index; MI, myocardial infarct; VHD, valvular heart disease; TIA, transient ischemic attack; ESRD, end-stage renal disease; DM, diabetes mellitus; OR, odds ratio; CI, confidence interval.
|
The four most important factors favoring non-OAC treatment were end-stage renal disease (ESRD) on dialysis (OR 0.27; 95% CI: 0.19–0.40), cancer (OR 0.67; 95% CI: 0.56–0.81), myocardial infarct (OR 0.53; 95% CI: 0.40–0.72), and history of major bleeding (OR 0.57; 95% CI: 0.39–0.84).
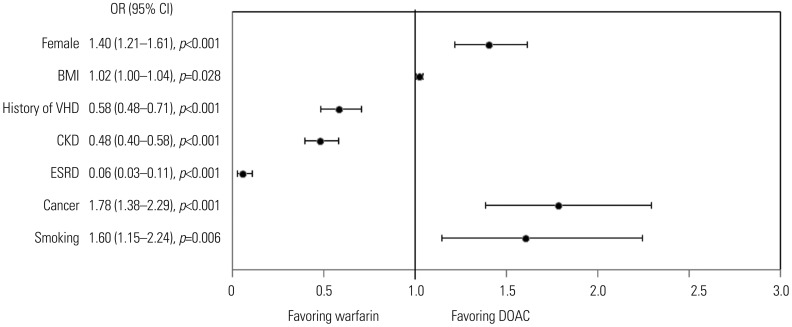
DOAC vs. warfarin in patients with CHA2DS2-VASc ≥2
We analyzed variables favoring DOAC or warfarin in the CHA2DS2-VASc score ≥2 group. The three important variables favoring DOAC treatment were female sex (OR 1.40; 95% CI: 1.21–1.61), cancer (OR 1.78; 95% CI: 1.38–2.29), and smoking (OR 1.60; 95% CI: 1.15–2.24) (Fig. 4). Variables favoring warfarin were ESRD (OR 0.06; 95% CI 0.03–0.11), chronic kidney disease (CKD) (OR 0.48; 95% CI 0.40–0.58), and history of valvular heart disease (OR 0.58; 95% CI 0.48–0.71) (Fig. 4). History of bleeding had no effect in determining the type of OAC.
OAC vs. DAT or TAT
In patients with CHA2DS2-VASc ≥2, antiplatelet agents were simultaneously used with OAC in 585 (7.8%) out of 7547 patients, including 433 (5.7%) who received DOAC and 152 (2.0%) with warfarin. However, 73.6% patients did not have any indication for the combination of antiplatelet agents, such as acute coronary syndrome, percutaneous coronary artery disease, or high thrombotic coronary lesions.
Variables associated with OAC plus antiplatelet agents were history of myocardial infarct (OR 3.94; 95% CI: 2.73–5.67), history of peripheral artery disease (OR 3.09; 95% CI: 2.34–3.07), and dyslipidemia (OR 2.43; 95% CI: 2.01–2.94) (Fig. 5).
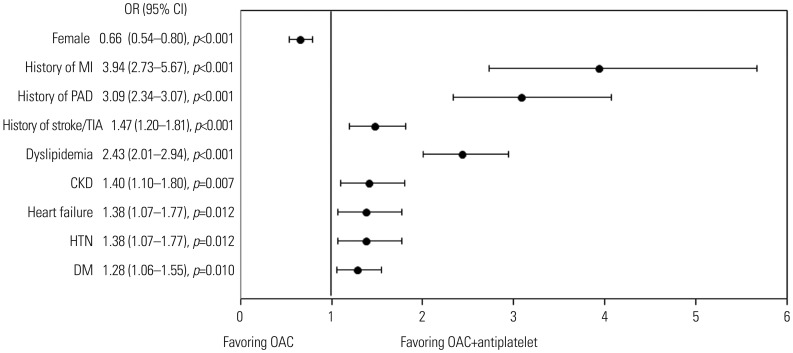 | Fig. 5Factors favoring OAC plus antiplatelet in patients with CHA2DS2-VASc ≥2. OAC, oral anticoagulant; MI, myocardial infarct; PAD, peripheral arterial disease; TIA, transient ischemic attack; CKD, chronic kidney disease; HTN, hypertension; DM, diabetes mellitus; OR, odds ratio; CI, confidence interval.
|
Go to :
DISCUSSION
Among AF patients at high risk of stroke, OAC was not administered in 16.8% of patients. Turkish registry showed that 27.1% of patients who have CHA2DS2-VASc score ≥2 received no OAC therapy. The primary reasons for the lack of anticoagulant usage in patients with high stroke risk were physicians' concerns for bleeding events and patient refusal.19 In our study, the four most important factors favoring non-OAC treatment were ESRD, history of myocardial infarct, history of major bleeding, and cancer. Second, among OAC patients, DOACs were used in 68.8%. Important factors favoring DOAC treatment were female, cancer, and smoking status. Finally, a combination of OAC and antiplatelet agents was used in 7.8% patients, but without definite indication in most patients (73.6%). This result suggests that, while adherence to general OAC guidelines has improved, antiplatelet agents are still being used against indication, thus necessitating improvement in the adherence to guidelines in Korean patients with AF.
The incidences of major bleeding and hemorrhagic stroke seem to be higher in patients under warfarin treatment. In large randomized controlled trials,10 patients treated with warfarin presented rates of 3.1–3.4%/year and 0.70–0.80%/year for major bleeding and hemorrhagic stroke, respectively. DOAC showed a significant reduction in hemorrhagic stroke of 0.23–0.49% and a similar reduction in major bleeding rate of 2.13–3.6%. Furthermore, DOAC was more frequently prescribed in patients with a history of major bleeding or hemorrhagic stroke. Table 2 shows a summary of different AF registry results for variables favoring DOAC or warfarin. In a Danish registry, patients under DOAC treatment were female, older, and had higher prevalences of stroke, bleeding, and alcoholism. Similar to this study, the main factor associated with warfarin treatment was the presence of kidney disease, myocardial infarction, and congestive heart failure.20 In a Spanish study (FANTASIIA), patients under DOAC treatment had higher prevalences of hemorrhagic stroke and bleeding history, university education, and higher glomerular filtration rate. Prescription of warfarin was higher in patients with history of cancer or bradyarrhythmias.21 A recent retrospective observational study reported that patients with greater bleeding and ischemic stroke risk were more likely to initiate warfarin, whereas in those at lower risk of bleeding, DOAC usage was more common.22

Table 2
Summary of Atrial Fibrillation Registry for Variables Favoring Warfarin or DOAC
| Study | Registry name | Number of data | Favoring warfarin variables | Favoring DOAC variables |
|---|---|---|---|---|
| Olesen, et al.20 | Danish | 18611 | CKD, MI, HF | Older age, female, prior stroke history, bleeding history, alcohol abuse |
| Moreno-Arribas, et al.21 | FANTASIIA (spanish) | 1290 | Malignancy, bradyarrhythmia | Major bleeding history, hemorrhagic stroke history, university education, high diastolic blood pressure, higher eGFR |
| This study | CODE-AF | 10529 | ESRD, CKD, history of valvular heart disease | Female, cancer, smoking history |
![]()
High-quality anticoagulation control with warfarin is associated with better efficacy and safety (with low stroke and bleeding risks); thus, effective stroke prevention in various guidelines on OAC refer to the use of well-controlled warfarin [time in therapeutic range (TTR) ≥70%) or one of the DOACs.23 However, it is difficult to maintain optimal TTR in Asian patients with AF.24
A cost-effectiveness study has demonstrated that DOACs are cost effective in Asian patients with AF.25 In this study, the usage rate and guideline adherence of OAC dramatically increased, because of the increased use of DOAC (55.6%). Interestingly, warfarin usage decreased more than that reported in a previous Korean study.1 Other studies reported a risk-treatment paradox, in which OAC use decreased with an increasing stroke risk.26 However, this study showed that the rate of OAC use was consistently maintained, even in patients with high bleeding risk.
TAT poses a higher bleeding risk than OAC or DAP alone.2728 Recent studies about DOAC showed that double antithrombotic therapy with OAC and a P2Y12 inhibitor is safer than triple antithrombotic therapy, including the use of warfarin.2930 Notably, both the 2018 ESC guidelines and the 2019 ACC/AHA/HRS guidelines for AF recommended DAT (COR IIa) as an alternative to TAT to reduce bleeding risk, although this indication is currently only applied to patients at high bleeding risk in European guidelines.153132 Therefore, the need for DOACs in combination with antiplatelet agents should be critically assessed, and the duration of combined therapy should be minimized. However, 73.6% patients did not have an indication for the combination of antiplatelet agents, such as acute coronary syndrome, percutaneous coronary artery disease, or high thrombotic coronary lesions. This result suggests that awareness regarding new guidelines is urgently required for Korean patients with AF.
The main limitation of our study is the nature of a transversal observational study. Our analysis of medication use focused on prescriptions filled in the first few months of the calendar year, and we were unable to ascertain longitudinal adherence. Secondly, patients are representative of a Korean population, and results may not be extrapolated to other populations. Finally, as all patients were enrolled from tertiary centers, the current registry is not free from referral bias.
In conclusion, ESRD, history of myocardial infarct, and history of major bleeding were related to non-OAC treatment. Renal disease and history of valvular heart disease were associated with warfarin usage, while female, cancer, and smoking status were associated with DOAC usage in patients at high risk of stroke. A combination of antiplatelet agents with OAC was prescribed in 73.6% patients without definite indication recommended by guidelines. This result suggests that, while adherence to general OAC guidelines have improved, antiplatelet agents are still being used against indications, thus necessitating improvement in adherence to guidelines in Korean patients with AF.
Go to :
 XML Download
XML Download