

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Trigeminal neuralgia (TN) is defined by the International Headache Society as “recurrent unilateral brief electric shock-like pains, abrupt in onset and termination, limited to the distribution of one or more divisions of the trigeminal nerve and triggered by innocuous stimuli.”1 It is characterized by the presence of a trigger zone, no objective neurological deficit, and no other identified causes of facial pain; it can cause severe pain and disrupt or impair quality of life in patients.2
Treatments for TN consist of pharmacological treatments, such as that with carbamazepine; surgical treatments, including open surgery and percutaneous procedures; and radiosurgery, including gamma knife radiosurgery (GKRS). Historically, GKRS was introduced as a treatment for TN. The Swedish neurosurgeon Lars Leksell began treating TN patients in 1951 using a prototype guiding device linked to a dental X-ray machine.3 Lindquist reported on the progress of TN patients who had undergone GKRS in 1991, and several studies have documented the safety and efficacy of GKRS, including long-term results, for TN.456 Other techniques of radiosurgery, such as cyber knife surgery and linear accelerator, were introduced in the 2000s and have shown effectiveness, compared to other surgical treatments.78
Several modifications have been made to the treatment regimens for GKRS over the past few decades. We reviewed the rationale, effects, safety, and current treatment policies of GKRS for TN in view of our institution's results and a review of the literature to date.
PATHOPHYSIOLOGY OF TN
The pathogenesis of TN is not fully understood, and its exact pathophysiology remains controversial. However, in general, it is described by a mixed peripheral and central mechanism.9 Neurovascular conflict is the most accepted theory, as it is related to TN in a vast majority of cases.10 Chronic nerve compression results in demyelination of trigeminal sensory fibers within the proximal nerve root, with progressive axonal degeneration.11 Demyelination can lead to ephaptic transmission, and the reentry mechanism causes an amplification of sensory inputs.1012 Meanwhile, nerve injury leads to a release of mediators that sensitize peripheral nerve terminations, resulting in neurochemical and phenotypic changes and increased excitability of trigeminal neurons and trigeminal nuclei (central sensitization).11 Ultrastructural and biochemical changes in axons and myelin are seen in the root, the Gasserian ganglion, or both.13
CLINICAL FEATURES AND CLASSIFICATION
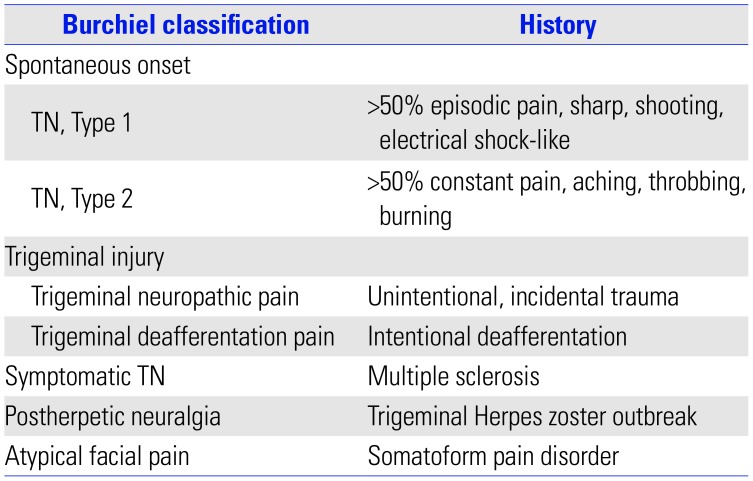
According to the International Classification of Headache Disorders, 3rd edition (ICHD-3), TN can be diagnosed when recurrent paroxysms of unilateral facial pain of a severely intense, electric shock-like, shooting, stabbing, or sharp nature occurs in one or more divisions of the trigeminal nerve.1 It should not radiate beyond the territory of the trigeminal nerve, should last between 1 second and 2 minutes, and should be precipitated by innocuous stimuli within the affected trigeminal distribution. TN is divided into the following three categories according to its cause: classical TN, secondary TN, and idiopathic TN. Classical TN refers to cases without an apparent cause other than neurovascular compression. When underlying diseases are present, such as a tumor in the cerebellopontine angle, arteriovenous malformation, or multiple sclerosis, secondary TN is diagnosed. Idiopathic TN could be diagnosed in cases where neither an electrophysiological test nor magnetic resonance images show significant abnormalities. Besides the ICHD classification, the Burchiel classification is also used to categorize TN and related facial pain syndromes using the characteristics of pain.14 The classification is based on the patient's history and is shown in Table 1.
GKRS AS A TREATMENT METHOD
Treatment method for TN
Treatments for TN are divided into the following three categories: pharmacological treatments; surgical treatments, including microvascular decompression (MVD) and percutaneous procedures, such as radiofrequency rhizotomy (RFR), balloon microcompression, and glycerol injection; and stereotactic radiosurgery.
The first therapeutic line is pharmacological treatment with carbamazepine. It is the only drug shown in a random-controlled trial to reduce the intensity and frequency of attacks, and it provides significant pain control in 80–85% of patients.15 Nevertheless, its efficacy can decrease, and in the long term, many patients become drug-resistant.16 Oxcarbazepine, baclofen, lamotrigine, and pimozide can also be used.17
Surgical treatment is the second therapeutic line and includes open surgery, percutaneous surgery, and radiosurgery. It is used in patients with medically intractable pain or those who suffer from side effects related to medication. MVD alleviates the underlying cause of a compressed trigeminal nerve root through exploration of the posterior fossa. It is considered a reference treatment modality, as it provides pain relief for approximately 90% of patients and has long-term effects (68–88% after 5 years and 61–88% after 10 years).1819 Therefore, MVD should be considered as the first surgical treatment modality for young patients with an obvious neurovascular conflict.20 However, major complications of surgery can include hearing loss, cerebrospinal fluid leakage, infection, hemorrhage, and brainstem infarction.1821
Percutaneous procedures are ablative techniques performed at the level of the Gasserian ganglion and are mechanistically based on physical, thermic, and chemical actions. Percutaneous procedures show a high initial success rate; however, over time, the recurrence rate is higher than that of MVD.22 The initial success rate for balloon microcompression was reported at 82–99%, and the median pain-free time was 20 months.2324 For glycerol injection, the initial success rate and the median pain-free time were 73–96% and 21 months, respectively.2425 For RFR, the initial success rate was 78.8–100%, and the probabilities of remaining pain-free 1, 2, and 11 years after the procedure were 65%, 49%, and 26%, respectively.262728 These ablative procedures pose a risk of hypesthesia, dysesthesia, severe facial numbness, corneal keratitis, and masseter muscle weakness.2930
Lastly, GKRS can be used for drug-resistant TN patients who are poor surgical candidates due to medical comorbidities or age or for those who refuse invasive therapy, especially in the absence of other primary indications, such as neurovascular conflict. GKRS has a very high rate of pain relief with minimal complications, showing a gradual decline in the complication rate due to advancement in imaging modalities.22 Burchiel's type 1 and type 2 TN are the most common indications of GKRS. GKRS may also be used in selected cases of multiple sclerosis-related and post-herpetic TN and in some cases of atypical facial pain.3132
Institutional results on GKRS for TN
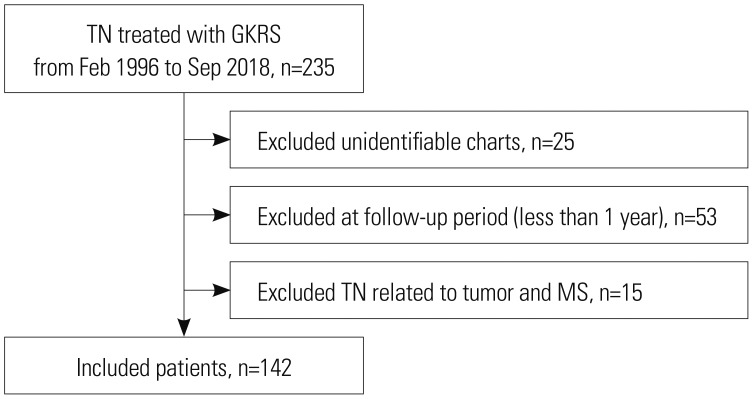
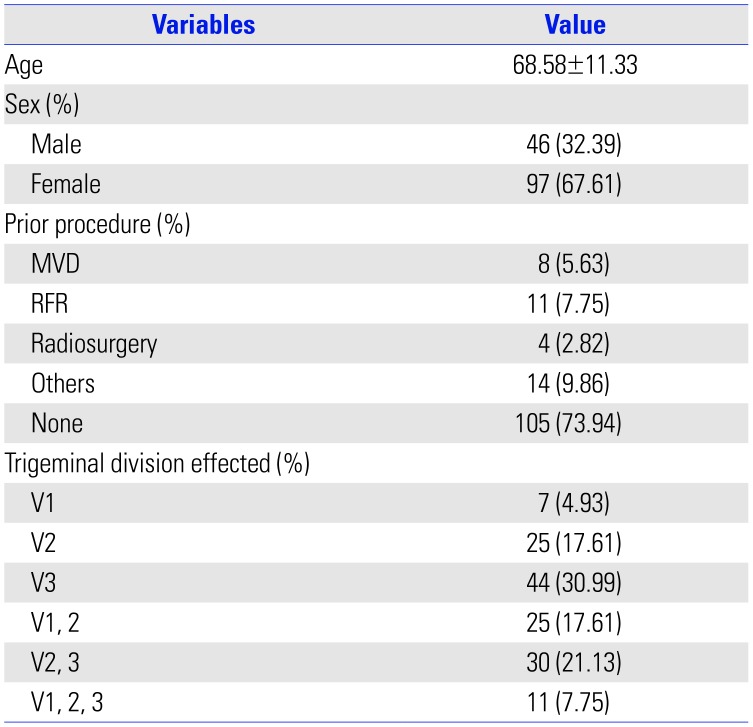
A total of 235 patients underwent GKRS for TN between February 1996 and September 2018. The indications for GKRS included failure of pharmacological treatment, significant adverse effects from medication, and failure of prior surgical treatment. Of these patients, 157 had charts and a follow-up period of more than 1 year. Of these patients, except for those with TN related to tumors and multiple sclerosis, 142 patients were reviewed (Fig. 1). Patient characteristics are shown in Table 2. GKRS was performed with a Gamma Knife (Leksell Gamma Knife, Elekta Instruments, Atlanta, GA, USA). Seven patients were treated with the Gamma Knife Model B, 28 patients with the Gamma Knife Model C, and 107 patients with the Perfexion Gamma Knife.
GKRS treatment was planned using T2-weighted magnetic resonance images with a slice thickness of 1 mm and constructive interference in steady-state images with 0.5-mm axial slices obtained with the stereotactic frame fixed to the head under local anesthesia. A single 4-mm isocenter with two or three beam blocking was used for treatment. It was positioned to cover the trigeminal root entry zone (REZ). After February 2005, planning was done such that a 15-Gy isodose line invaded less than 5% of the brainstem. The dose used varied from 60 to 90 Gy.
Pain from TN was assessed using Barrow Neurologic Institute (BNI) pain scores. BNI scores of I–IIIb were considered as indicative of successful treatment, whereas BNI pain scores of IV and V were considered reflective of unsuccessful treatment. Following improvements in pain after GKRS, any worsening of the pain (even if the level of pain was milder than that present prior to treatment) was considered as recurrence.
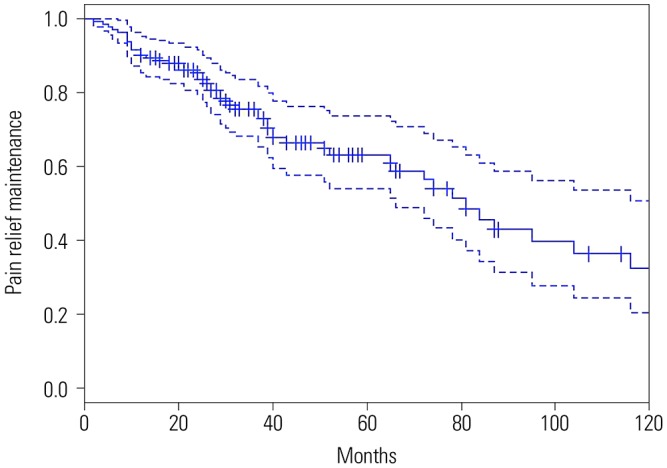
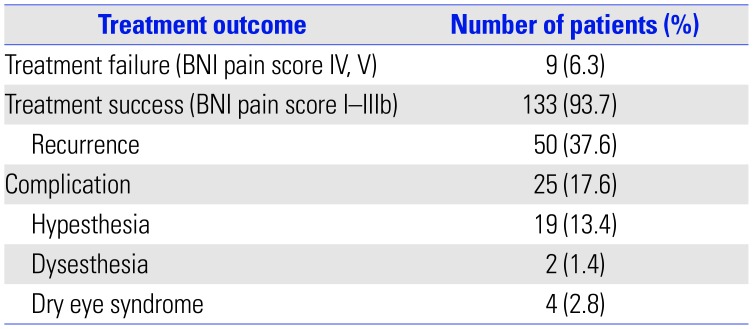
The median follow-up period was 37 months (12–250 months, 54.35±49.51 months). The median dose of gamma rays was 85 Gy (60–90 Gy, 84.23±3.743 Gy). After GKRS, 93.7% of patients (133/142) experienced successful treatment (Fig. 2). Of these, recurrence of pain occurred in 50 patients (37.6%, 50/133), and the median time to recurrence was 29 months (2–166 months, 42.26±38.08 months). Among patients who experienced recurrence, six (12%, 6/50) needed additional surgery or procedures, and the rest were controlled by medication. Complications were reported in a total of 25 patients (17.6%, 25/142) and included facial hypesthesia in 19 patients (13.4%), dysesthesia in 2 patients (1.4%), and dry eye syndrome in 4 patients (2.8%) (Table 3). Univariate comparisons were performed using the independent t-test and one-way ANOVA test. There were no statistically significant correlations between the prior procedure and complications (p=0.068) or between the types of prior procedures and complications (p=0.705). There were also no statistically significant relationships between dose and successful treatment, recurrence, and complications under significance of p<0.05.
Pain relief after GKRS
The rationale for achieving pain relief after GKRS is related to focal axonal degeneration of the trigeminal nerve associated with nociceptive sensibility, destruction of ionic channels, and electrophysiological blocking initially after nerve irradiation.3334 Additionally, a delayed radiation effect with axonal degeneration has been proposed, as some patients experience a late response after GKRS.35 In the literature, the latency to pain relief was 15 to 78 days on average, and the maximum time to pain relief was 6 months after treatment.29
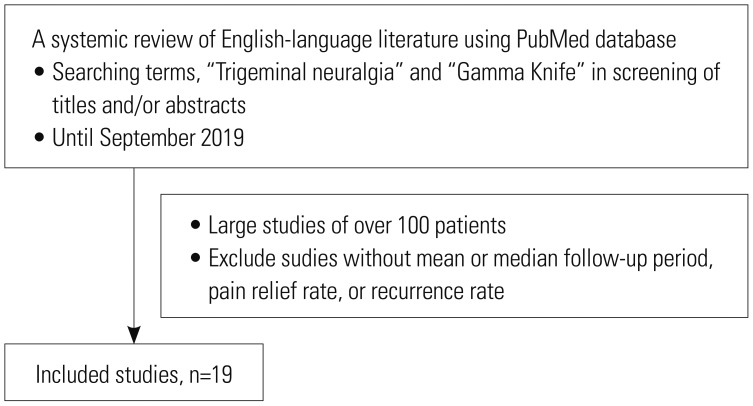
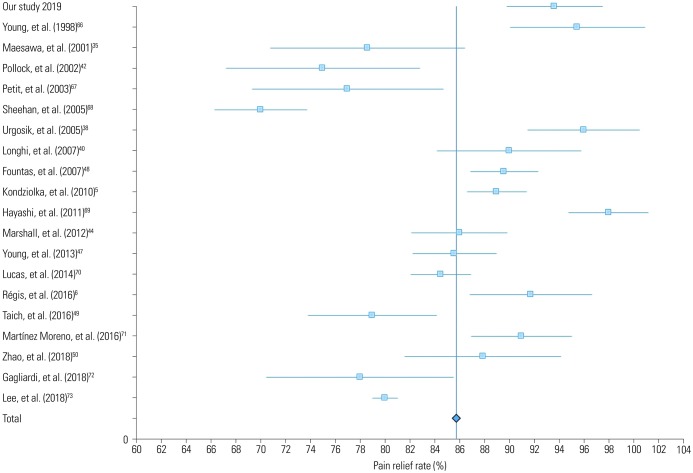
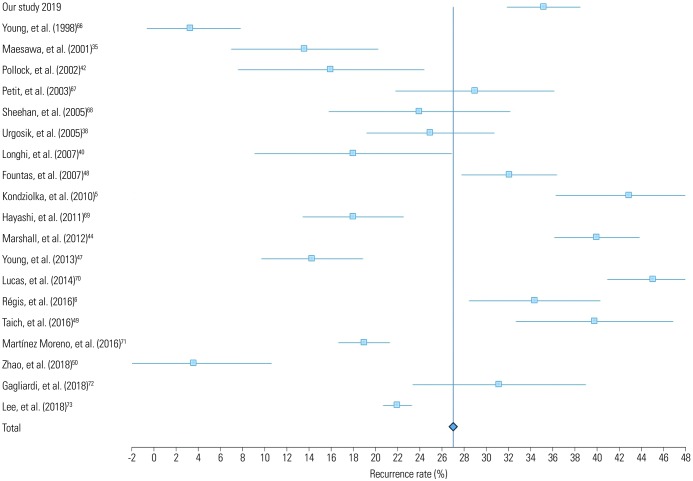
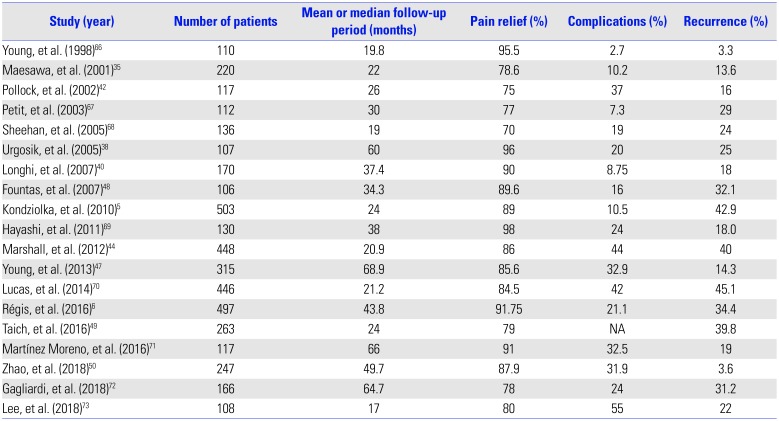
Table 4 lists studies with more than 100 patients who underwent GKRS for TN (Fig. 3). GKRS showed high rates of pain relief, ranging from 70–98% in large studies of over 100 patients (Fig. 4). Pain control was achieved in 69–85% of cases at 1 year, 59% at 2 years, and 38–52% at 5 years.3536 Regarding long-term results, rates of pain control maintenance were 32–59.7% at 7 years and 30–45.3% at 10 years.5637 Although follow-up periods vary among the studies, making direct comparison difficult, the average pain free duration was 7–58 months.353839 The mean recurrence rate was 26.9%, with a range of 3.3–45.1% (Fig. 5). In comparison, our data showed a higher recurrence rate than the average. This may be due to a difference in follow-up periods, because in our study, some patients experienced recurrent pain after approximately 14 years.
Complications of GKRS
Complications due to GKRS are uncommon, with hypesthesia being the most common adverse event. The incidence of hypesthesia is reported to be up to 2.7–55.0%, with a mean occurrence rate of 22.55%, slightly higher than our result (Table 4). Similar to the latency period for GKRS to be effective, there may also be a latency period between the procedure and the development of complications. The mean time to hypesthesia occurrence ranged from 6 to 36 months.29
Other complications include dysesthesia, deafferentation pain, dysgeusia, dry eye syndrome, keratitis, hearing impairment, and masticator weakness.4142 Rarely, significant injury to adjacent vasculature due to high doses have been reported.43 Terms used in each article related to complications had a lack of precision; hence, there may be differences in the rate of complications. Studies have reported dysesthesia in 0–16%, paresthesia in 0–13%, deafferentation pain in 0–3.3%, dry eye syndrome in 0–22.4%, and keratitis in 0–7%.44454647
Complications were not associated with the prior procedure in previous studies, which is consistent with our results.484950 This may be due to some differences in the mechanisms of complications in destructive procedures, such as GKRS, versus nondestructive procedures, such as MVD. Also, in MVD and other destructive procedures, such as RFR, the duration of complications is short, which does not seem to affect complications in a subsequent surgery. However, in the case of radiosurgery, there is a report that previous radiosurgery affects complications because there is a latency period of radiosurgery.49
Several studies have shown that complication rates are associated with the target selection, the length of the irradiated nerve, and the dose.425152 Our study showed a complication rate similar to that in previous studies, and complications due to GKRS do not appear to be statistically related to the high dose used.
Repeat GKRS
Due to the low incidence of complications associated with GKRS, rather than other procedures, repeat GKRS may be considered for pain recurrence. Repeat GKRS appears to have a similar efficacy to initial GKRS for TN, with rates of complete and partial pain relief ranging from 78% to 85%.515354 There is a report that prior GKRS is associated with bothersome facial numbness after GKRS. The main complications after repeat GKRS are new facial sensory symptoms caused by partial trigeminal nerve injury, seen in 11–69% of patients.545556
Therefore, to reduce complications due to repeat GKRS, decreasing the dose of the second GKRS would be helpful, as would moving the target to not overlap with the previous target, so that a previously treated nerve is not exposed to a high dose of radiation.54
GKRS policy: dose and target
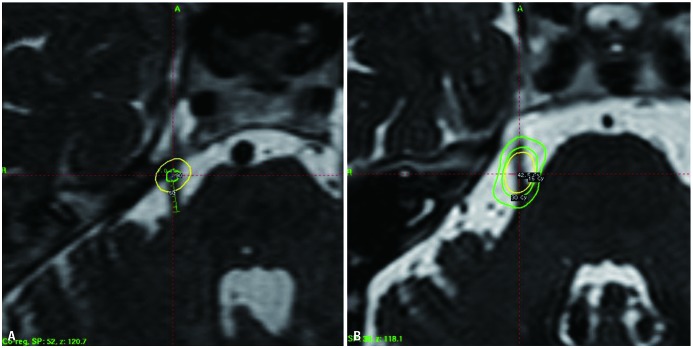
When GKRS was first used for TN, Leksell3 targeted the Gasserian ganglion. After that, Lindquist, et al.4 reported the results of GKRS targeting the Gasserian ganglion in 1991 and then stated the results of treatment of the trigeminal REZ, where peripheral myelination with Schwann cells transits to central myelination with oligodendrocytes. Rand, et al.57 reported the results of the GKRS targeting the retrogasserian area, anterior to REZ, in 1993. Since then, both the REZ and retrogasserian area have been used to treat TN with GKRS (Fig. 6).
There is still controversy regarding which target is better. The major difference between the targets is the dose received by the REZ and the brainstem. However, the effect and complications related to the target and the dose are not established. Several studies have compared the complications and effects between anterior and posterior targets.585960 They reported that an anterior target has lower complications than a posterior target, showing similar or better pain relief. However, since there is a difference between doses among studies and targets and the appropriate dose has not yet been established for the target, it is difficult to directly determine which target is better.
Determination of the treatment dose may vary according to the target. However, studies have shown that a dose of 70 Gy failed to control pain in 100% and that radiation below 70 Gy had little effect on the structure of the trigeminal nerve.6162 A radiation dose of more than 80 Gy causes partial degeneration with loss of axons and demyelination, which is the mechanism of pain relief in GKRS.62 Therefore, GKRS with 80 Gy or higher is usually performed. In addition, many studies have shown that higher doses lead to greater pain control.636465 However, a high dose of more than 90 Gy is related to a higher complication rate with similar pain control effects; hence, they are not usually used.56 Recently, a dose between 80 and 90 Gy is generally used, with modification depending the circumstances.
CONCLUSION
GKRS has been used for TN for a long time with low complication rates and high success rates. Over time, technical refinements have improved its safety and efficacy. GKRS is being increasingly used as a primary intervention for TN for patients who cannot undergo surgery due to medical comorbidities and age or for those who refuse invasive therapy. To further increase safety and efficiency, discussions are underway on the treatment policy to be applied. In the future, advances in imaging modalities and in GKRS technique, as well as accumulation of long-term results and experience will yield better results of GRKS for TN.
 XML Download
XML Download