

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic rhinosinusitis (CRS) is an otorhinolaryngologic condition that is common around the world and affects quality of life1 (QoL), health care2 and productivity.3 CRS often occurs concurrently with lower airway diseases, such as asthma, in Caucasian patients, but not in Chinese patients.45 CRS is classified into 2 phenotypes, CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP).67 The endotypes of CRS differ based on the inflammatory cytokine profiles of the Caucasian and Chinese patients.5 Caucasian CRSwNP patients show a greater proportion of T helper (Th) 2 cells and higher levels of eosinophilic infiltrate than Chinese patients.5 Recent studies in China on the pathogenesis, phenotyping, endotyping, and different treatments of CRS have resulted in significant new developments that highlight progress in Chinese rhinological research. Consequently, the Chinese Society of Allergy and the Chinese Society of Otolaryngology Head and Neck Surgery convened an expert task force to develop the Chinese guidelines for CRS, founded on evidence-based models. After the initial meeting in October 2017, 2 seminars were held to update the consensus statement in August 2018 and January 2019. The guidelines on CRS (available in English) can be readily accessed by the international scientific community and will benefit clinical practice and research on CRS across the globe.
EPIDEMIOLOGY AND THE BURDEN OF CRS
The suggestions provided in the European Position Paper on Rhinosinusitis and Nasal Polyps (EP3OS), regarding the definition of symptom-based rhinosinusitis, are used in epidemiological studies.6 However, comparisons based on epidemiological studies are undesirable because of insufficient data, variable methods of investigation, and differences in regional, social, and economic circumstances of various countries.8 Medical management and surgical interventions cannot effectively control symptoms in CRS patients. The symptoms of CRSwNP and CRSsNP overlap; however, CRSwNP patients have more nasal symptoms and show higher symptom scores than the CRSsNP patients.9 CRSwNP is becoming increasingly prevalent and is particularly difficult to treat using conventional therapies.2
The estimated prevalence of CRS is 10.9% in Europe,10 16% in the United States,11 and 5.51% (EP3OS-defined CRS) in Sao Paulo, Brazil.12 A Population Health Survey estimates the prevalence of CRS in Korea to be 6.95%.13 In Canada, 5.7% of women and 3.4% of men have CRS.14 CRS is more prevalent than asthma and chronic obstructive pulmonary disease (COPD) according to the vital health statistics.15 Due to its high prevalence, CRS imposes enormous health and economic burdens on individuals, families, communities, and on society as a whole.16 The health burden of CRS in Asia is huge, especially in developing countries. CRS is common in mainland China with an estimated prevalence of 8%, meaning that approximately 107 million individuals have CRS.17 Due to changes in the environment and based on the status of health care, the prevalence and pattern of CRS can vary regionally and change over time.
CRS causes pronounced physical symptoms including a reduced sense of smell, rhinorrhea, nasal blockage, facial pressure or pain, and headache. Although not fatal, these symptoms are persistent and can affect QoL and work by impairing the general health, vitality, and social functioning of CRS patients. These symptoms can also result in stress-associated disorders, which can manifest as depression and anxiety.181920 Patients report that CRS impacts their daily life more severely than do medical examinations.21 In Southeast China, patients with CRS visit physicians 4.5 times more, and miss 11.7 more days of work or school per year than individuals without CRS. Patients with CRS are more likely to wake up during the night due to shortness of breath or coughing than individuals without CRS (6.9% vs. 1.4% and 14.7% vs. 4.2%, respectively).22 Individuals with self-reported CRS perceive to have an impaired QoL in terms of physical and mental functioning; this particularly affects women, the elderly and those with a higher level of education. These factors as well as clinical care must be considered when assessing the burden of CRS.
Clinical studies have shown that a patient's QoL can be greatly improved by adequately treating CRS.2123 However, few population-based studies show how CRS affects QoL. Studies examining QoL of CRS patients have mostly focused on patients with severe symptoms clinically diagnosed by nasal endoscopies and CT scans. It is still unclear whether, and to what extent, CRS impairs QoL in people with relatively mild symptoms. Moreover, patients without CRS, chosen as negative controls for these studies, may suffer from other disorders that affect their QoL. This selection bias has likely resulted in the effect of CRS on QoL. Furthermore, the impact of CRS on different subpopulations should also be considered.
CRS in combination with asthma is a common but severe airway disease.24 An epidemiological study by the Global Allergy and Asthma Network of Excellence showed a strong association between asthma and CRS (adjusted odds ratio, 3.47) in all age groups.25 In contrast, it has been reported that the prevalence of asthma among CRS patients in China is relatively low.26 Fan et al.26 showed that only 2–3% of CRS patients in southern China have concurrent asthma. Clinically, nasal polyps with comorbid asthma (NPcA) have gained increased attention due to the severity of this disease and due to the high recurrence of nasal polyps (NP).2728 In Western countries, approximately 32% of CRSwNP patients have asthma,2930 but the prevalence of NPcA in the Chinese population is unknown. NPcA is highly heterogeneous with respect to clinical, physiological and pathological parameters. A cluster analysis of 110 patients with NPcA by Wu et al.31 resulted in the classification of these patients into the following 3 distinct categories: atopic NPcA, smoking NPcA, and NPcA occurring at older age. This classification may contribute to improved management of NPcA. With respect to disease severity and treatment approaches, the clinical features of NPcA occurring concurrently with aspirin sensitivity differ from those of NPcA without aspirin sensitivity.32 Aspirin desensitization improves disease management and QoL in this patient population.3334
GENETICS AND EPIGENETICS
Genetic factors working in concert with environmental factors affect the development of CRS.35 Formal heritability studies are rare, but genetic studies on CRS have provided crucial insight into the etiology of this condition.36 Several studies have reported familial aggregation and significant familial risk of CRS.3738394041 Mutations in the CFTR gene, which causes cystic fibrosis (CF), are significantly associated with CRS, indicating that genetic variations in immunological molecules in the mucosa of the sinuses contribute to the pathogenesis of CRS.42 Using exome sequencing, Zhang et al. 43found a novel mutation in DNAH5 (c. 8030G > A), which may be responsible for CRS and primary ciliary dyskinesia in a Chinese family. Allergic rhinitis and asthma, which show even higher heritability, occur frequently in CRS patients,1726 further indicating the potential role of genetic components in CRS.
Candidate genes and genome-wide association studies (GWAS) have been used in genetic studies of CRS. Currently, over 70 genes are known to be associated with CRS,44 but only a limited number of susceptibility genes can be replicated.4546474849 Only a few single-gene association studies on CRS have been performed in China, and none of the reported susceptibility genes and loci for CRS have been identified in other populations. The susceptibility genes in the Chinese population with CRS are listed in Table 1. Most of these genes code for cytokines and cytokine receptors, proteins involved in the immune response pathways and airway remodeling proteins. Two DNA pool-based GWAS were conducted in Caucasian CRS patients and healthy controls. One study identified a total of 600 SNPs in 445 genes that were statistically significant; additionally it showed that the top 10 CRS-associated genes, including LAMA2 and LAMB1, PARS2 (the mitochondrial function gene), and AOAH showed interactions at the basement membrane (BM) and in the extracellular matrix (ECM).50 Another study reported 23 genetic variants associated with Staphylococcus aureus colonization in CRS patients.51 Zhang et al.50 identified the same CRS susceptibility genes that had been found earlier in a pool-based GWAS in a Caucasian population. Additioally, the study confirmed one SNP locus (rs4504543) in the AOAH gene, indicating that some genetic elements involved in the pathogenesis of CRS are common between Chinese and Caucasian populations.48 A large-scale GWAS on CRS and NP was performed in 2 large European cohorts with 4,366 NP patients, 5,608 CRS patients, and > 700,000 controls. This study indicated that a loss-of-function missense variant of ALOX15, p.Thr560Met shows a significant genome-wide association with NP and CRS.52 ALOX15 codes for arachidonate 15-lipoxygenase, which is elevated in NP tissues and plays an important role in inflammatory processes. Although the ExAC database shows that the p. Thr560Met variant of ALOX15 exhibits no polymorphisms in the East Asian population, other functional variants of ALOX15 associated with NP and CRS should be investigated in the Chinese population.
Table 1
Susceptibility genes for CRS identified in Chinese population studies
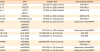
CRS, chronic rhinosinusitis; SNP, single-nucleotide polymorphism; CRSwNP, chronic rhinosinusitis with nasal polyps; HLA, human leukocyte antigen; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; ARMS-PCR, amplification refractory mutation system-polymerase chain reaction; VNTR, variable number tandem repeat; PCR-SSP, polymerase chain reaction-sequence specific primer.
![]()
Unlike genetic variations, epigenetic modifications can influence gene and protein expression without changing or modifying the basic DNA sequence, which impacts chronic inflammatory processes and patterns in certain tissues.5354 Hypermethylation in the promoter region of the collagen type XVIII alpha 1 chain was found in CRSwNP tissues obtained from a Chinese patient cohort.55 In airway epithelial cells, the overexpression of miR-125b increases type I interferon (IFN) expression by suppressing the EIF4E-binding protein 1, which may play an important role in the development of mucosal eosinophilia in eosinophilic CRSwNP.56 Additionally, Ma et al.57 reported that microRNAs (miRNAs) could potentially be involved in the regulation of dendritic cell (DC) function and in the core pathogenesis of CRS, highlighting new therapeutic targets in CRS.
MECHANISMS
General immunity involved in airway diseases
Unlike other organ systems in the body, the respiratory system is relatively open and consistently exposed to infectious agents, allergens, pollutants and other environmental factors. The diseases of the respiratory system occur in the upper and lower respiratory tracts. The immune system enables the host to resist infection and to clear harmful substances from the body. Immune cells (i.e., airway epithelial cells, DCs, granulocytes, mast cells, macrophages, innate lymphoid cells [ILC], T cells and B cells) and molecules (cytokines, chemokines, immunoglobulins [Igs] and complement factors) may be involved in the pathogeneses of the aforementioned diseases. For example, although CRS develops as a result of dysregulation of the immune response upon exposure to external stimuli, genetic factors should also be considered. The innate immune system is the first barrier in the body's defense system. In CRS patients, the innate immunity provided by the airway epithelium is impaired, leading to an insufficient local innate immune response against microbial agents and antigens that invade and stimulate the mucosal tissues. The abnormal innate immune response also initiates and maintains chronic inflammation by recruiting and activating other innate and adaptive immune cells.58
Breakdowns of tight junctions or defective nasal-sinus epithelial cells are typical of CRSwNP. They may be caused by external stimuli and inflammatory mediators, leading to abnormal regulation and declining function of epithelial cells.59 Activation of Toll-like receptor (TLR) signaling pathways or epithelial injury may promote expression of thymic stromal lymphopoietin (TSLP), interleukin (IL)-25, and IL-33 by epithelial cells; these molecules serve as important connections between innate and acquired immunity.60 In CRS patients, the expression of TSLP is significantly increased,6162 and this may promote the differentiation of T cells into Th2 cells63 and encourage type 2 ILC (ILC2) to secrete type 2 cytokines, especially IL-5, IL-13 and IL-4.6465 This cascade may explain why TSLP is positively associated with chronic type 2 eosinophilic inflammation which is observed in CRSwNP patients.6266 Expression of IL-25 and its receptor (IL-17RB) is also significantly elevated in CRSwNP patients. In a murine NP model, anti-IL-25 treatment reduced the number of polyps, thickness of the mucosal edema, collagen deposition and infiltration of inflammatory cells, 67 suggesting that IL-25 might serve as a potential target for CRSwNP.68
In addition to activating the DCs and inducing Th2-mediated reactions, TSLP, IL-25 and IL-33 may also contribute to the locally increased numbers and activity of ILC2 cells in CRSwNP.60 IL-33 is associated with the secretion of Th1 and Th17 cytokines and the local accumulation of neutrophils in Asian CRSwNP patients.69
Increased numbers of ILC2 cells are highly correlated with eosinophilia in blood and local tissues.7071 Type 2 cytokines contribute to the maturation and activation of eosinophils and induce the activation of endothelial cells and other target cells expressing adhesion molecules, chemokines, and different T-cell-associated factors.7072 Different DC subsets and macrophages may be involved in the pathogenesis of the distinct phenotypes and endotypes of CRS, as indicated by the increased number of distinct DC subsets in the NP4373; this suggests that these subsets may be functionally different from each other. Furthermore, it has been found that the CD11c+ DC counts are significantly elevated in the NP of subjects suffering from eosinophilic allergies compared to those in the relevant controls.74 Correspondingly, M2 macrophages, which predominate in CRSwNP, attracted DC and Th2 cells by secreting chemokine (C-C motif) ligand (CCL) 18. An increased number of CD163+ M2 macrophages was also observed in eosinophilic NP of atopic subjects.74 Conversely, M1 macrophages were predominant in CRSsNP.75 Eosinophils play a critical role in CRSwNP, type 2 inflammation and local tissue damage76; local basophil and mast cell counts are normally associated with those of the infiltrating eosinophils.77
T-helper cell subtypes may contribute to the phenotypes and endotypes of CRS. Th1 cells are normally the predominant T lymphocytes in CRS patients, especially in those with CRSwNP. Th2 cells are mainly found in the nasal polyp tissues of CRSwNP patients but are nearly absent from the nasal mucosa of the CRSsNP patients.7879 CRSwNP patients, especially in China, show an infiltration of various inflammatory cells, mainly neutrophils, and Th1 and Th17 cells.8081 Some patients show an assortment of infiltrating cells. For example, Th17/Th2-type inflammation may exist simultaneously in the same nasal polyp, while neutrophils with relevant biomarkers may also occur in eosinophilic NP.5 Th17 cells may participate in the pathogenesis of CRS by secreting IL-17A and IL-21,8283 but the role of the regulatory T cells (Tregs) in CRSwNP tissues remains controversial.84
The increase in the number of B cells, plasma cells and lymphoid follicles in the NP of the CRSwNP patients might be due to the upregulated expression of B-cell activating factor (BAFF) in local tissues. Local B cells are activated under certain conditions and can differentiate into memory B cells and/or plasma cells, which produce IgM, IgG, IgA and IgE after undergoing somatic hypermutation and/or class switch recombination.8486 IgE is a key factor in some CRSwNP patients,87 while other types of antibodies may contribute to local inflammation and tissue damage via the activation of classical complement pathways.88 Some autoantibodies, such as antinuclear antibody, anti-double stranded DNA (anti-dsDNA) antibody and anti-neutrophil cytoplasmic antibody, have been detected in the polyp tissues.899091 The potential mechanisms associated with asthma, rhinitis and CRS are illustrated in Fig. 1.
 | Fig. 1Potential mechanisms of immune cells and mediators involved in the pathogenesis of airway diseases.IL, interleukin; DC, dendritic cell; TSLP, thymic stromal lymphopoietin; BAFF, B-cell activating factor; Ig, immunoglobulin; Th, T helper; CCL23, chemokine (C-C motif) ligand 23; CRSsNP, chronic rhinosinusitis without nasal polyps; CRSwNP, chronic rhinosinusitis with nasal polyps.
|
Microbiology of CRS
Initially, CRS was thought to be an infectious disease that was caused by viruses, fungi or bacteria. Although CRS is indeed an immune-mediated condition, the local microbial milieu may exacerbate the progression of CRS.92
Standard microbial cultures and gene sequencing are the 2 major methods that are used to identify microbes locally. Standard cultures offer defined conditions for microbial growth, and gene sequencing (especially next-generation sequencing) is culture-independent and targets taxonomically-informative regions of the genome.93 A comparison between the 2 approaches showed that only half of the dominant bacteria and 5% of the low-abundance bacteria identified with gene sequencing in CRS patients and healthy controls were identified by the standard culture method. Next generation sequencing will further provide detailed information about microbial communities inhabiting the nasal sinus membrane.94
Bacteria
No differences were found between the CRS patients and healthy individuals with respect to bacterial composition, indicating that bacteria existent in the CRS patients were also likely to exist in the healthy individuals. Most studies show an increased bacterial abundance in CRS patients. However, results regarding bacterial diversity in CRS patients compared to that of healthy controls are controversial.95 Staphylococcus, Propionibacterium and Corynebacterium were found to be the most abundant bacteria in the sinonasal mucosae of both CRS patients and healthy controls; Anaerococcus, Streptococcus, Pseudomonas, Haemophilus and Moraxella were less common.92
In the sinonasal mucosae, bacteria exist as free-floating planktonic replicating cells and biofilms. Biofilms are complex, multicellular assemblages comprised of a polysaccharide matrix, which acts as structural basis for microbial clusters and as a barrier to the surrounding environment. Biofilms protect the bacteria living inside from various threats, including host phagocytic cells, antibiotics, and surfactants.9697 CRS patients with biofilm formation have poor prognosis and postoperative outcomes.98
Different bacteria play different roles in the pathophysiology of CRS. S. aureus frequently colonizes the human nose and is more abundant in CRS patients than in healthy controls.99 Exotoxins produced by S. aureus disrupt the integrity of the epithelial barriers and show anti-inflammatory activity. They affect the complement system, antimicrobial peptide production, adhesion, and chemotactic processes.100101 S. aureus enterotoxins (SEs) can act as super-antigens, stimulating the generation of polyclonal IgE and eosinophilic inflammation. IgE specific to SEs (SE-IgE) occurs in nearly half of all the NP. The presence of specific IgE in response to enterotoxins A and B (SEA and SEB) is positively correlated with the total IgE concentration and eosinophilic inflammation in the nasal tissue.102 However, the polyp colonization rate of S. aureus in Chinese CRSwNP patients and healthy controls is much lower than that reported in European studies.103 Only 20% of the NP express IL-5 and are predominantly colonized by gram-positive bacteria in Chinese CRSwNP patients.104 Liu et al.105 found no significant differences in the bacteriological profiles in the nasal middle meatus among the Chinese CRSwNP and CRSsNP patients and healthy controls. They also showed that the most common bacteria were coagulase-negative Staphylococci, Corynebacterium species, S. aureus, and Haemophilus influenzae. Interestingly, the isolation rates of S. aureus are lower in Chinese CRSwNP patients than in their Caucasian counterparts.105
Corynebacterium tuberculostearicum was found to be correlated with the severity of CRS, and this was further confirmed in a human cohort and in a study performed in a murine model.106 Some bacterial species may play a protective function in CRS patients. Acinetobacter johnsonii exhibits a higher mean relative abundance in healthy individuals and it can release factors that promote IL-10 production, thereby exerting beneficial anti-inflammatory effects in patients with CRS.107
Fungi
Fungi widely colonize the sinonasal mucosae of CRS patients and healthy individuals. Amplicon sequencing, used to study fungal organisms in CRS, revealed no major differences in the fungal microbiomes of the controls and the CRS patients.108 The results regarding the prevalence are conflicting. Cleland et al.108 reported that Malassezia was the most prevalent fungal genera, while Aurora et al.109 found Cryptococcus to be the most commonly-detected organism. These variations may have resulted from differences in detection methods, CRS subtypes, disease severity, geography and other comorbidities.110
Fungi and bacteria may interact, and the presence of fungi may help bacteria to invade and grow in the sinonasal mucosae of patients with allergic fungal rhinosinusitis (AFRS). For example, adhesion of S. aureus to the Candida albicans hyphae may aggravate intramucosal invasion.111 Oral, topical and intravenous antifungals are not recommended in CRS, indicating that fungi are unimportant in the pathophysiologic processes of CRS.112
Viruses
CRS is more severe during seasons that are associated with a high prevalence of viral infection.113 Cho et al.114 detected multiple respiratory viruses in the lavage samples from CRS patients but not in those from the non-CRS controls, with human rhinovirus showing particularly higher prevalence in CRS patients than in the controls. Liao et al.115 tested the scraped epithelial cells from the middle meatus and revealed a higher prevalence of respiratory viruses in the CRSwNP and CRSsNP patients than in the healthy controls although the difference was not statistically significant. Viral infections can increase the incidence of opportunistic secondary bacterial infections which exacerbate CRS116 by disrupting epithelial barrier integrity and impairing ciliary function and mucociliary clearance (MCC).117 Wang et al.118 showed severe infiltrations of S. aureus into the nasal mucosa and CRSwNP tissues pre-infected with herpes simplex virus type 1 (HSV1). Nasal polyp tissues collected from the CRSwNP patients—who were infected with HSV1—showed significantly lower production of IFN-γ and IL-17 than the inferior turbinate tissues from the healthy controls.119
Innate immunity and CRS
Innate immunity in the sinonasal cavity and pathogen detection by the TLRs expressed on the sinonasal epithelial cells, bitter taste receptors, and sweet taste receptors, are important protective factors. Activation of these receptors elicits innate immune responses, resulting in improved MCC and defensin secretion.58 Innate immune effector cells, including dendritic and mast cells, eosinophils, and ILCs, are involved in shaping the CRS pathophysiology and contribute to the secretory phenotype of T cells and B-cell differentiation.120
Eosinophilic and non-eosinophilic CRSwNP also show distinct lesional DC profiles. Only DCs from eosinophilic CRSwNP induced enhanced Th2 responses when cocultured with naive CD4+ T cells.43 In innate immunity, the expression of the antimicrobial protein, nasal epithelium clone 1 in the short palate and lungs (SPLUNC1) is differentially impaired in subsets of eosinophilic and non-eosinophilic CRSwNP. Eosinophilic CRSwNP shows significantly decreased SPLUNC1 expression.121 TSLP—which is similar to IL-7 and is produced by epithelial and keratinized cells122—is an important initiator of the Th2-cell response. TSLP activates dendritic and other antigen-presenting cells, thereby driving the differentiation of CD4+ T cells towards the Th phenotype.123 TSLP and TSLP receptors show significantly higher expression in the eosinophilic CRSwNP compared to that in the non-eosinophilic CRSwNP.124
Immune and epithelial cells in the sinonasal mucosa interact with the inhaled environmental stimuli and the nasal bacterial microbiome, thereby forming a dynamic immune barrier that is altered in CRS. Defects in innate immunity combined with chronic activation of various inflammatory cells are responsible for CRS pathogenesis. Epithelial injury in the nasal mucosa may allow pathogens, proteases, or antigens to enter the lamina. These irritants, together with IL-25, IL-33 and TSLP secreted during epithelial injury, initiate, recruit and activate antigen-specific T and B cells.72
T-cell immunity in CRS
T-cell-associated immunity, especially CD4+ Th cells, which orchestrate local mucosal immune responses, may play an important role in CRS pathogenesis. Dysregulation of the Th1/Th2 balance may cause a Th2-biased response, which induces the formation of NP.125126127128 CRSsNP is characterized predominantly by a Th1-mediated neutrophilic milieu whereas CRSwNP is characterized by Th2-biased eosinophilic inflammation in Caucasian patients.129130
Derycke et al.79 found more CD3+ T cells in the NP tissues than in the CRSsNP or control nasal tissues but observed no significant differences between the CRSsNP and the control tissues. They found that effector T cells predominantly showed a Th1 phenotype in CRSwNP and CRSsNP and in the control mucosal tissues. However, Th2 cells (CD3+CD4+ cells producing IL-4 or IL-5) were only detected in CRSwNP.
Th17 cells are a novel Th-cell subset that express IL-17 and are involved in T-cell-mediated immunity in CRS. Cao et al.82 demonstrated an upregulated Th17 response in Asian patients with CRSsNP or CRSwNP. Derycke et al.131 found that Th17 cells can modulate neutrophil survival by secreting IL-17A in Caucasian patients with non-CF and CRSwNP. IL-17A+-cell numbers were positively associated with those of eosinophils in the Japanese CRS patients.132 Jiang et al.133 showed enhanced Th17 responses in Chinese CRSwNP patients. Saito et al.83 showed that IL-17A+-cells are correlated with high eosinophil numbers but not with the high neutrophil counts in Japanese patients with asthma-associated CRSwNP.
Several studies have presented conflicting findings on the role of Tregs in CRS pathogenesis. Two separate studies have found that the expression of FoxP3, the master transcriptional regulator of Tregs, is decreased at the messenger RNA (mRNA) and protein level in CRSwNP as is the expression of the regulatory cytokines IL-10 and transforming growth factor (TGF)-β, indicating a Treg deficiency or dysfunction in CRSwNP tissues.81129 Wu et al.134 found decreased expression of FoxP3 in the NP tissues compared to that in the healthy uncinate process tissues. They found a molecular mechanism regulating the inhibitory function of Tregs via the phosphorylation motif (Ser270/274) of Foxp3, which is recognized by the proinflammatory kinase, GSK-3β. Ma et al.135 found decreased percentage of FoxP3+CD8+ Tregs in the eosinophilic and non-eosinophilic NP. Conversely, Miljkovic et al.136 found that Tregs (CD45+CD4+CD25+CD127low) are significantly elevated in the CRSwNP nasal tissues compared to those in the CRSsNP tissues. Overall, the frequencies of Tregs (CD3+CD4+CD25+FoxP3+) were significantly higher in the CRS tissues than in the control tissues, while CD8+ Treg (CD3+CD8+CD25+FoxP3+) levels were significantly reduced in the CRSwNP.137 In summary, although Tregs play an important role in inflammatory diseases, it is essential that the role of Tregs in CRS be investigated worldwide.
B-cell immunity in CRS
As key components of adaptive immune responses, B cells produce antibodies, function as antigen-presenting or regulatory cells and can contribute to the pathogenesis of inflammatory disorders, including CRS. Although B cells are likely to be important in CRS, their role in airway mucosa is unclear and should be determined in future studies.
B cells accumulate in the lamina propria of NPs.85 The levels of total IgE, SE-IgE, and IgE-positive cells, are increased in CRSwNP samples.87 Furthermore, the levels of the Ig isotypes, IgM, IgG, IgA and IgE, are elevated in the CRSwNP nasal mucosa. Ig isotypes with the exception of IgE, show normal expression in the sera of CRSwNP patients, indicating that antibodies in the NPs are produced by local immune cells.138 Whether B-cell responses in CRSwNP nasal mucosa are antigen specific, superantigen-stimulated, or an expansion of natural antibody responses, remains to be determined.139 IgE may be involved in the pathogenesis of CRSwNP through activation of eosinophils, mast cells, and basophils via Fc receptors.8485 The antigen specificity of antibodies and their roles in CRS are unclear.84 Further, it is also unknown whether these B cells enter the nasal tissue as naïve cells and later become activated, or whether they enter the nasal tissue as memory cells and get primed within the tissue.
In Western countries, CRSwNP manifests in the form of a local Th2-mediated inflammation with increased IgE levels. IgE induces allergic inflammation by activating the mast cells and basophils. Germinal center (GC)-like structures are detected in CRSwNP. The type 2 cytokine, IL-13 is responsible for the B-lineage cell responses in eosinophilic CRSwNP. IL-13 can stimulate IgE class-switch, recombination, and IgE production in B cells.140 BAFF, a important factor for B-cell maturation and survival, can induce T-cell dependent or independent Ig class switching and production, resulting in increased CD20 expression. Concentrations of BAFF, IgE and IL-5, are increased in eosinophilic nasal polyp tissues, and BAFF protein levels are associated with those of IgE and IL-5.141 Previous studies have suggested that the levels of Th17-associated mediators (myeloperoxidase [MPO], IL-8, IL-17A and IL-23), BAFF, and Th1 cytokine (IFN-γ), were upregulated in refractory CRSwNP compared to that in the controls and primary NP regardless of tissue eosinophilia or asthmatic comorbidity.142
BAFF is a pathogenic factor in autoimmune diseases. The levels of IgG anti-dsDNA and anti-BP-180 antibodies are increased in CRSwNP nasal tissues, suggesting that these autoantibodies are involved in the pathogenesis of CRSwNP.89 Locally increased B-cell accumulation and IgE responses occur in CRSwNP with over 30% of B and plasma cells in the NP re-expressing RAG1 and RAG2 that are required for receptor revision, class switching to IgE, and B-cell differentiation into IgE-secreting plasma cells.86143 B cells and activated plasma cells may be recruited by the B cell chemotactic factors C-X-C motif chemokine ligand (CXCL) 13 and CXCL12, which are elevated in CRSwNP.144
Eosinophils in CRS
Eosinophils, which are important granulocytes and immune-system components, develop during hematopoiesis in the bone marrow and then migrate into the blood where they respond primarily to invasion of multicellular parasites. Eosinophils are important for modulating allergy and asthma. In healthy individuals, eosinophils make up approximately 1%-3% of white blood cells. In some CRS patients, eosinophilia is increased and is independent of concomitant allergic rhinitis and atopy. Based on the extent of tissue eosinophilia, CRSwNP is classified into eosinophilic and non-eosinophilic subtypes. These subtypes, which are characterized by their distinct clinical features, computed tomography (CT) scans, and different immunopathologic mechanisms, are associated with different prognoses and therapeutic strategies (details have been provided in section 5.1, eosinophilic CRS [ECRS] and non-ECRS).
Tissue eosinophilia is modulated by miRNAs. Eosinophilic CRSwNP shows distinct miRNA expression profiles in Chinese adults. MiR-125b is specifically upregulated in eosinophilic CRSwNP and may enhance type I IFN expression thereby contributing to tissue eosinophilia.56
Osteopontin (OPN), also known as early T lymphocyte activation 1, is a phosphorylated acidic glycoprotein produced by various immune cells.145 A study using an in vitro dispersed NP cell culture system showed that recombinant human OPN promotes eosinophil migration and the production of eosinophilic cationic protein (ECP).146
High mobility group box 1 (HMGB1), a non-histone chromatin-binding nuclear protein, is essential for DNA recombination, repair, and transcription, and for cellular differentiation and signaling.147 In the extracellular microenvironment, HMGB1 is involved in the recruitment of inflammatory cells.148 Expression of HMGB1 protein and mRNA is higher in eosinophilic CRSwNP than that in the controls.149
Neutrophils in CRS
Neutrophils are terminal effector cells in tissue destruction and antibacterial defenses. They are also immunocompetent cells that upregulate the inflammatory response by secreting cytokines, including IL-1α, -1β, -6 and -8, IFN-α, and tumor necrosis factor (TNF).150 Subtypes of polarized neutrophils include classical, proinflammatory N1, and anti-inflammatory or tumorigenic N2 neutrophils.151 The roles of the N1 and N2 neutrophils in humans have not yet been detailed, especially in CRS.
Compared to CRSwNP, CRSsNP is more neutrophilic and shows a type 1- and type-17-dominant cytokine profile.5 Biofilm-positive CRSsNP patients also exhibit higher levels of neutrophils.152153 Neutrophils are major sources of TGF-β2 in CRS, the expression of which is upregulated in CRSsNP and non-eosinophilic CRSwNP. Thus, neutrophils play an important role during the fibrotic events in CRSsNP and non-eosinophilic CRSwNP.130 They are also major sources of oncostatin M (OSM) in individuals with CRSwNP and severe asthma. OSM is elevated in CRSwNP and may contribute to the disruption of the epithelial barrier.154 Aging may affect neutrophil responsiveness and survival. Age-related decline in neutrophil-mediated inflammation occurs in non-eosinophilic CRSwNP and may favorably influence postoperative results in elderly patients.155 Elastase-positive neutrophils may be a cellular biomarker in refractory CRSwNP.156
The recruitment of neutrophils from the circulation into the extravascular spaces first involves transendothelial migration of the neutrophils into the inflammatory sinus mucosa. Then, neutrophils migrate out of the mucosa and into the sinus effusion. Mucosal epithelial cells and IL-8 are essential for neutrophil recruitment in CRS.157158 Growth-related oncogene-alpha, granulocyte chemotactic protein-2, and epithelial cell-derived neutrophil attractant-78 are also implicated in neutrophil chemotaxis in CRS, while the roles of CXCL1, CXCL2 and IL-1β which are also involved in neutrophil chemotaxis, remain undetermined.158159
Composed of several proinflammatory cytokines, including IL-1β, IL-36γ and IL-33, IL-1 cytokine family participate in the regulation of neutrophilic inflammation in CRS.160 Recently, Wang et al.161 reported that the expression of the IL-36 family is upregulated in CRSsNP and CRSwNP. Epithelial cell-derived IL-36γ can be activated by neutrophil-secreted elastase. Neutrophils are the major cell type expressing IL-36R in CRS.161 Upon activation by cleaved IL-36, neutrophils secrete IL-17A and -8 thereby exacerbating neutrophilic inflammation in CRS.161
Remodeling in CRS
Remodeling refers to permanent or transient changes in tissue architecture, including structural changes in the epithelium and production of the ECM.162 Tissue remodeling in CRS may occur concurrently with or after inflammation.
Classification of tissue remodeling in different CRS types
In addition to the persistent and exaggerated inflammation of the sinonasal mucosa, CRS is also characterized by marked tissue remodeling, including epithelial damage and metaplasia, BM thickening, fibrosis, goblet cell and mucus gland hyperplasia, and/or edema.130163164 Hellquist's classification lists 4 types of tissue remodeling that occur in CRS: edematous, fibrotic, glandular and atypical.165 Increased fibrosis is observed in CRSsNP whereas CRSwNP involves tissue edema with albumin deposition and pseudocyst formation.166167 Both CRSsNP and CRSwNP involve goblet-cell hyperplasia in the epithelium.84
Mechanisms of tissue remodeling in CRS
Tissue remodeling is a dynamic process involving growth factor-induced ECM production and the degradation of ECM mediated by proteases and protease inhibitors.164 TGF-β and matrix metalloproteinases (MMPs) are both critical factors involved in these processes.168 The proteins and cytokines involved in CRS-associated tissue remodeling are listed in Table 2.
Table 2
Biological modulators associated with tissue remodeling in chronic rhinosinusitis

| Biological modulators | Author | Technique | Result | Conclusion |
|---|---|---|---|---|
| Growth factors and cytokines | Watelet et al.422 | ELISA, RT-PCR, IHC | CRSsNP presented significantly higher concentrations of TGF-β1 at the protein and mRNA levels, compared to those in the CRSwNP samples. No TGF-β1 staining was found in the pseudocyst areas of the NPs. | In CRS, TGF-β1 was associated with fibrosis. |
| Liu et al.423 (study in Chinese) | IHC, RT-PCR, cell culture, immunofluorescence | Eosinophil derived TGF-β1 induced tenascin C (an ECM glycoprotein) expression in nasal epithelial cells in CRSwNP. | Eosinophil-derived TGF-β1 may contribute, at least partially, to tissue remodeling in CRSwNP. | |
| Li et al.164 (study in Chinese) | Immunoassay, RT-PCR | TGF-β1 and FOXP3 levels were significantly increased in CRSsNP but reduced in CRSwNP. | Lack of TGF-β1 expression in CRSwNP may contribute to edema in CRSwNP. | |
| Li et al.169 (study in Chinese) | Western blotting | TGF-β1, TGF-βRI, TGF-βRII, Smad3 and Smad7 levels were increased in CRSsNP, while Smad3 levels were decreased in CRSwNP. | CRSwNP was characterized by a lower level of TGF-β1 signaling. | |
| Shi et al.130 (study on Chinese) | RT-PCR, IHC | TGF-β1 was downregulated in all types of CRS. TGF-β2 protein levels were upregulated in CRSsNP compared to CRSwNP and the controls. No significant differences in the TGF-β3 mRNA expression levels were observed among the different types of CRS. | Distinct remodeling patterns were revealed for the different types of CRS. Neutrophils were the major sources of TGF-β2 and were related to fibrosis in CRS. | |
| Metalloproteinase and tissue inhibitor of metalloproteinase | Bhandari et al.170 | RT-PCR, IHC | Levels of MMP-2 were upregulated in CRSwNP. MMP2 cleaved type IV collagen, the major structural component of the BMs. | Upregulation of the MMP2 in CRSwNP may damage the collagen in the BMs of the epithelium and blood vessels, causing an increase in vessel permeability and an edema in the stroma. |
| Li et al.164 (study in Chinese) | ELISA | TIMP-1 and TIMP-4 levels were lower in CRSwNP than in CRSsNP. | Decreased inhibition of collagen degradation may contribute to edemas in CRSwNP. | |
| Shi et al.130 (study in Chinese) | RT-PCR, IHC | MMP-2 mRNA levels were downregulated in CRSwNP, but not in CRSsNP. MMP-7 mRNA levels were upregulated in all CRS types. TIMP-4 protein levels decreased in the eosinophilic CRSwNP and increased in the CRSsNP. No difference in the TIMP-1 mRNA expression in the different study groups was observed. | Lower expression of TIMP-4 may lead to loss of inhibition of the MMPs and result in extensive edemas in the eosinophilic CRSwNP. | |
| Kahveci et al.171 | IHC, ELISA | MMP-9 levels were increased in the glands of the CRSwNP patients. TIMP-1 levels were decreased in the polyp tissues. | MMP-9 and TIMP-1 imbalances may lead to edemas in the CRSwNP. | |
| Wang et al.424 (study in Chinese) | ||||
| Coagulation factors | Shimizu et al.425 | ELISA | Thrombin and thrombin-antithrombin complexes were significantly increased in the nasal secretions of the CRSwNP patients with asthma, compared to those in the control group. Thrombin and protease-activated receptor 1 agonist peptide significantly stimulated VEGF secretions in the cultured human airway epithelial cells. | Increased activation of the coagulation system occurred in the sinonasal mucosa of the CRS patients, and thrombin may play a role in nasal polyp formation, by stimulating VEGF production from airway epithelial cells. |
| Takabayashi et al.173 | RT-PCR, ELISA, IHC | FXIII-A was significantly increased in the CRSwNP tissues, and most FXIII-A-positive staining was observed in the type 2 macrophages of the CRSwNP. | Overproduction of FXIII-A by type 2 macrophages may contribute to excessive fibrin depositions in the submucosa of CRSwNP patients, which may contribute to tissue remodeling and pathogenesis of CRS wNP. | |
| Takabayashi et al.174 | RT-PCR, ELISA, IHC | The levels of the fibrin were increased, whereas those of the d-dimer were decreased in the CRSwNP, suggesting reduced fibrinolysis. t-PA expression was decreased in CRSwNP and may be downregulated by Th2 cytokines. | A Th2-mediated reduction in t-PA may lead to excessive fibrin depositions in the submucosa of NP, which may contribute to tissue remodeling and pathogenesis of the CRSwNP. | |
| Shimizu et al.426 | IHC, ELISA | TF expression was localized to the nasal epithelial cells and the infiltrating eosinophils of the nasal mucosa. TFPI expression was localized to the nasal epithelial cells, and fibrin depositions were observed in the lamina propria of NPs. | By upregulating the coagulation systems, TF and TFPI playan important role in the pathogenesis of CRSwNP. | |
| Other proteins and cytokines | Coste et al.427 | IHC | PDGF expression was increased in the NP epithelium, compared to that of the controls. | Increased local PDGF production was involved in the epithelial cell proliferation of NPs. PDGF could also be involved in the pathogenesis of NP via its effects on connective tissue remodeling. |
| Hu et al.428 (study in Chinese) | IHC | The level of expression of the VEGF and the mean blood-vessel density were significantly greater within the NPs than within the corresponding sinusitis mucosa. The expression of these parameters correlated well with the relative size of the NPs. | VEGF participated in the development of NPs, possibly via regulating blood vessel formation. | |
| Kouzaki et al.429 | IHC | PDGF was produced by macrophages, eosinophils, and epithelial cells and acted on epithelial cells and fibroblasts with PDGF receptor expression in CRSwNP. | PGDF potentially promoted tissue fibrosis and the formation of NP in CRSwNP. | |
| Lee et al.430 | ELISA, IHC, Flow cytometry | VEGF functioned in an autocrine manner to promote nasal epithelial cell growth and to inhibit apoptosis. | VEGF functioned through neuropilin-1 to amplify cell growth, contributing to hyperplastic polyposis. | |
| Shi et al.130 (study in Chinese) | RT-PCR | HB-EGF mRNA expression correlated with TGF-β2 expression. | A potential role of HB-EGF in TGF-β2-mediated tissue fibrosis in CRS. | |
| Bayar Muluk et al.431 | IHC | Fibroblast-derived PDGF is possibly more important than mononuclear cell-derived PDGF in the polyp developing process. Perivascular PDGF expression was increased in the deep mucosal layers of the NPs. | Increased perivascular PDGF expression in the deep layers of the mucosa resulted in sinonasal polyp formation, as it caused increased vascular permeability and extracellular edema and promoted migration of the inflammatory cells to the extracellular area. | |
| Lin et al.432 (study in Chinese) | IHC | PDGFRα protein expression was increased in CRSwNP compared to that in the controls and was expressed significantly more in the eosinophilic CRSwNP than in the non-eosinophilic CRSwNP. | PDGFRα may play a pivotal role in the pathophysiology of CRSwNP by synergizing with PDGF-A. | |
| Hu et al.433 (study in Chinese) | RT-PCR, ELISA | VEGF mRNA expression level was significantly increased in CRSwNP compared to that in the control. Protein levels of the VEGF could be downregulated by clarithromycin. | Therapeutic effects of the clarithromycin in the CRS occurred partially via the downregulation of VEGF expression. | |
| Wang et al.162 (study in Chinese) | IHC | The expression of TLR2 correlated negatively with the squamous hyperplasia in CRSsNP, and positively with the gland hyperplasia in CRSwNP. TGF-β1 was downregulated by the TLR2 agonist in CRSwNP and upregulated by the TLR4 agonist in CRSsNP. MMP-9 was upregulated by the TLR4 agonist in CRSwNP. | TLR2 and TLR4 were closely associated with TGF-β1 expression and tissue remodeling in CRS. | |
| Li et al.434; Sha et al.435 (study in Chinese) | IHC, ELISA | HGF affects the expression of TGF-β1 and plays an antifibrotic role. | The balance of HGF and TGF-β1 is involved in CRS tissue remodeling. | |
| Azizzadeh Delshad et al.436 | IHC | The expression of VEGF was significantly higher in CRSwNP than in CRSsNP. | VEGF was involved in polyp formation. | |
| Ebenezer et al.172 | IHC | Periostin is an ECM protein that is elevated in the sinonasal tissues of the CRS patients. Periostin expression is associated with remodeling changes and tissue eosinophilia. | Periostin expression was associated with BM thickening, fibrosis, and tissue eosinophilia, and may be used to identify patients undergoing tissue remodeling. |
CRSwNP, chronic rhinosinusitis with nasal polyps; CRSsNP, chronic rhinosinusitis without nasal polyps; CRS, chronic rhinosinusitis; NP, nasal polyps; IHC, immunohistochemistry; RT-PCR, reverse-transcriptase protein chain reaction; ELISA, enzyme-linked immunosorbent assay; TGF, transforming growth factor; TGF-βR, transforming growth factor-beta receptor; FOXP, forkhead box protein; MMP, matrix metalloproteinases; mRNA, messenger RNA; TIMP, tissue inhibitor of metalloproteinases; Smad3, SMAD family member 3; PDGF, platelet-derived growth factor; PDGFRα, Platelet-derived growth factor receptor alpha; VEGF, vascular endothelial growth factor; HGF, hepatocyte growth factor; HB-EGF, heparin-binding epidermal growth factor; TLR, Toll-like receptor; ECM, extracellular matrix; BM, basement membrane; TF, tissue factor; t-PA, tissue plasminogen activator; TFPI, tissue factor pathway inhibitor.
![]()
In CRSsNP, fibrosis is mainly associated with high levels of TGF-β1 or TGF-β2. Upregulated expression of receptors and signal transducers in CRSsNP induces the activation of the TGF-β signaling pathway.169 However, the expression levels of TGF-β1 in CRSwNP are debated (Table 2).
Edematous CRS, commonly observed in CRSwNP and eosinophilic CRSwNP, may result from an imbalance between the expression of MMPs and tissue inhibitor of metalloproteinases (TIMPs) (Table 2).164170171 Reduced TIMP-1 and -4 expression may disinhibit the activities of MMP 2, 7 and 9, thereby resulting in the generation of the extensive edemas observed in CRSwNP.130 Periostin, an important tissue-remodeling molecule, is also associated with the basement-membrane thickening and fibrosis in CRS.172 Activation of the coagulation system and increased generation of thrombin and coagulation factor XIII-A lead to the excessive production and cross-linking of fibrin and edema in CRSwNP.173174
Correlation between tissue remodeling and inflammation in CRS
Tissue remodeling is associated with the inflammation patterns in Chinese CRS patients. Eosinophilic and neutrophilic inflammation is positively correlated with the severity of edema and fibrosis, respectively, in CRS. Neutrophils are the major sources of TGF-β2, which is upregulated in CRSsNP and non-eosinophilic CRSwNP, relative to that of the control tissues and eosinophilic CRSwNP.130 Eosinophilic NPs were characterized by diffuse ethmoidal and olfactory involvement, whereas non-eosinophilic NPs showed more localized patterns and maxillary sinus involvement. In addition, high ethmoidal/maxillary CT scores were positively correlated with the levels of Th2 inflammatory markers, including IL-4, IL-5, periostin mRNA expression and total IgE levels in the NPs, whereas the levels of the Th1 cytokines and IFN-γ, were inversely correlated.175
Epithelial exfoliation and BM thickness are strongly correlated with the number of infiltrating eosinophils176 and IL-17A-positive cells83 in CRS. Conversely, tissue remodeling may promote inflammation. MMP-2 and -9 and TGF-β1 facilitate eosinophil and mast cell migration into the NP.177 However, airway remodeling can occur early in life178 without obvious inflammation,179 challenging the view that remodeling is dependent on prior development of inflammation.
Epithelial to mesenchymal transition (EMT) in CRS
The epithelium provides an effective barrier between the airway and subepithelium. This barrier supports epithelial cells, tight junctions, and adherens junctions, which ensure a strong cell-to-cell contact.180 If epithelial cohesion and integrity are destroyed by injury, inflammation or infection, the sinonasal mucosa can be invaded by pathogens and environmental antigens, resulting in the development of CRS.59
EMT is a process in which epithelial cells lose their cell-to-cell interactions and polarized character, eventually turning into spindle-shaped migratory mesenchymal cells. This process is crucial for wound repair, organ development, and tumor progression.181 EMT is characterized by the downregulated expression of epithelial marker proteins (including E-cadherin, ZO-1, claudin and occludin) and upregulated expression of mesenchymal-associated markers (including periostin, vimentin, MMP2, MMP9 and α-smooth muscle actin [αSMA]).72 It is implicated in CRS.182 The process of tissue remodeling, which induces epithelial loss and differentiation of fibroblasts into myofibroblasts, is associated with the pathogenesis of CRSwNP.164 The loss of E-cadherin expression is a fundamental event in EMT.183 Meng et al.163 found that increased TGF-β expression activates myofibroblasts to express αSMA and vimentin and that the expression of ZO-1, occludin and E-cadherin was reduced in mature polyps. EMT is particularly prevalent in the stalks of early-stage polyps, indicating that polyp stalks are an important site for EMT events.163 Hypoxia can induce EMT, and expression of hypoxia-inducible factor-1α is correlated with E-cadherin loss and αSMA expression. It is likely that hypoxia-induced EMT contributes to nasal polyp formation.184 Although the exact mechanisms by which EMT plays a role in CRS are unclear, the role of inducible factors (including TGF-β, epidermal growth factor family, vascular endothelial growth factor and fibroblast growth factor) and EMT-inducing signaling pathways (including Notch, Wnt, tyrosine kinase receptor and SMAD) is well-documented in COPD and asthma and should therefore be examined in CRS.185
Osteitis in CRS
In 1998, Kennedy et al.186 examined 43 ethmoid bone samples obtained from endoscopic surgeries and developed the concept of “bone remodeling” to explain the phenomenon of osteitis. Osteitis occurs in CRS and involves the formation and destruction of active bones along with inflammatory cell infiltration of the bone surface.186
The mechanisms of osteitis in CRS are unclear. Bone is a dynamic tissue that is constantly formed and resorbed in response to changes in mechanical loading, altered serum calcium levels, and a wide range of paracrine and endocrine factors. The dynamic nature of the skeleton is maintained by remodeling, and this involves the coordinated activities of osteoclasts (cells that destroy bone) and osteoblasts (cells that form bone), as well as osteocytes within the bone matrix and osteoblast-derived lining cells that cover the bone surface. Cytokines such as nuclear factor-κB (NF-κB),187188 colony stimulating factor (CSF)-1, TNF, IL-6, IL-11, IL-13,189 IL-15, IL-17A190 and macrophage CSF may be involved in the initiation and regulation of bone remodeling. 191192 A significant positive correlation between IL-13 and mineralization was observed in vitro.189 Moreover, elevation of IL-13 and IL-17A in CRS with neo-osteogenesis was related to osteoblast differentiation by inducing Runt-related transcription factor 2.190 Osteitis is activated by the TGF-β/Smad signaling pathway in CRSwNP, indicating that eosinophils are important for bone remodeling.193
Osteitis in CRS is defined as, inflammatory changes in the marrow-less bone, leading to disruptions in the lamellar bone and the formation of new woven bone.194 Histopathological diagnosis is considered the “gold standard” for diagnosing osteitis. The diagnostic criteria include new woven bone, periosteal thickening, bone absorption, and fibrosis.186194195196197198199 However, imaging is more practical for the diagnosis of osteitis in CRS than histopathology. Presently, CT is used to diagnose and evaluate sinus osteitis. Biedlingmaier et al.198 used CT to evaluate and predict bone remodeling using decreased bone density, destruction of the trabeculae and bone cortex, and bone sclerosis.
For evaluating osteitis, Georgalas et al.199 recommended using a global assessment tool and developed the Global Osteitis Score System. This evaluation system consists of a scale for evaluating the thickness of nasal bones and can be used to determine the severity and scope of osteitis.199 Measuring the Hounsfield units in CT is even more accurate than measuring the bone density when evaluating osteitis in CRS.200
ENDOTYPES OF CRS
CRSwNP and CRSsNP are the 2 phenotypes of CRS based on the presence or absence of NP.6201 Discriminating between the 2 phenotypes is relatively straightforward and is done via nasal endoscopic examination and through imaging techniques such as CT scanning. The therapies available for CRS are scant and include nasal and/or oral corticosteroids, antibiotics (macrolides and doxycycline), and surgery (if the drug therapies prove unsuccessful).6202203 To reflect the pathomechanisms of CRS more comprehensively and to establish a more precise therapeutic strategy, it is necessary to define the endotypes of CRS. Distinct CRS clusters based on their immunological mechanisms, are important for the development of individualized treatment strategies for CRS patients. The determination of CRS endotypes will help in providing personalized treatments for this patient population.87204205
ECRS and non-ECRS
CRS is a heterogeneous entity showing different inflammatory endotypes. Based on the results of nasal endoscopy and CT scanning, the current guidelines recommend classifying CRS as involving or not involving polyps.6 However, these clinically observable phenotypes do not adequately reflect the diversity of CRS,206207 and cellular endotypes are more useful for determining the mechanisms of inflammation.
Mucosal eosinophilia is a common histological feature of NP. The inflammatory patterns of CRS are designated as eosinophilic and neutrophilic (non-eosinophilic) based on the predominant inflammatory-cell type.208
Statistically, patients with mucosal eosinophilia are defined as those who fall outside the normal range obtained using healthy sinonasal mucosa.209 Using this method, Cao et al.82 used a cutoff value of ≥ 10% (4.77% + (2 × 2.47%) = 9.71%) to determine the proportion of tissue eosinophils among the total inflammatory cells in the Chinese patients. The proportion of mucosal eosinophilia in CRS is 68% in Beijing and 46% in Wuhan.82
This cutoff value can be used to define tissue eosinophilia. However, tissue eosinophilia does not equate with eosinophilic CRSwNP. To determine eosinophilic CRSwNP, criteria should be fulfilled by examining the CRS tissue samples. To date, an international consensus has not been reached regarding the definition of ECRS perhaps in part because tissue eosinophilia in CRS is known to vary by geographical region.
Eosinophilic and non-eosinophilic CRSwNP have different clinical characteristics. Compared to non-eosinophilic CRSwNP, eosinophilic CRSwNP is more prevalent in men and is associated with smoking, atopy, and a higher absolute count of peripheral blood eosinophils and IgE levels. Peripheral eosinophils are independently and significantly associated with eosinophilic CRSwNP.210 Zuo et al.211 showed that a smell-loss score, ethmoid osteitis index, and the number and ratio of blood eosinophils, can be used as surrogate markers for the differential diagnosis of ECRS.
Eosinophilic and non-eosinophilic CRSwNP show distinct tissue remodeling patterns. Although Chinese patients with non-eosinophilic and eosinophilic CRSwNP present with edema in the lamina propria, eosinophilic CRSwNP is more edematous and less fibrotic compared to the non-eosinophilic CRSwNP. Eosinophilic CRSwNP shows decreased collagen deposition and increased severity of edema compared to that in the non-eosinophilic CRSwNP and CRSsNP.130 Glandular hyperplasia occurs more in non-eosinophilic CRSwNP and CRSsNP, than in eosinophilic CRSwNP.82131212 Atypical CRS, characterized by large and pleomorphic histiocytes, has been rarely found in Chinese CRS patients.
Eosinophilic and non-eosinophilic CRSwNP exhibit elevated Th1 and Th17 cell counts in the local microenvironment, while only eosinophilic CRSwNP shows increased Th2 cell counts. Chinese patients with eosinophilic CRSwNP show increased total IgE levels compared to those of patients with non-eosinophilic CRSwNP. Local IgE, specific for common aeroallergens, is more frequently found in the eosinophilic CRSwNP than in the non-eosinophilic CRSwNP.213
Although CRSwNP in Western countries is mostly eosinophilic,581 a significant percentage of CRSwNPs in Asian countries are non-eosinophilic, including China,82 Korea,214 Japan,215 and Malaysia.216 In China, neutrophil numbers are decreased further in the eosinophilic CRSwNP than in the non-eosinophilic CRSwNP and CRSsNP.130 Genetic factors or genetic/environmental interactions, may play a role in eosinophilic infiltration as evidenced by the reduced eosinophilia in second-generation Asian CRSwNP patients compared to that in the Caucasian CRSwNP patients.217 The inflammatory patterns have evolved over time. The prevalence of eosinophilic CRSwNP in Asian countries, including Thailand, Korea, and China, has increased remarkably in the past 10 to 20 years, indicating that environmental factors are involved in the pathogenesis of CRSwNP.214218219220221
In the previous decade, studies on CRS inflammatory patterns were mostly conducted in patients of European descent. Several recent studies have shown the immunological differences between patients of European descent and Chinese patients. Zhang et al.222 found fewer activated eosinophils and lower IgE levels in the NPs of patients from South China, compared to those of patients of European descent. They further showed that tissues from the CRSwNP patients of European descent exhibited significantly high levels of the Th2 cytokine IL-5 and Th2 transcription factor GATA binding protein 3 (GATA-3), and higher levels of eosinophilic inflammation (ECP/MPO77 ratio > 1) compared to those of the controls. These findings were obtained by comparing a Th1/Th17 cell pattern with neutrophilic inflammation (ECP/MPO ratio < 1) in tissues obtained from Chinese CRSwNP patients and healthy controls.81 Cao et al.82 found that CRSsNP patients from south China had higher levels of IFN-γ expression whereas only a subpopulation of patients with eosinophilic CRSwNP showed enhanced expression of GATA-3 and IL-5. These findings indicate immunological heterogeneity among different regions within the same disease phenotype and show why CRS phenotyping does not reflect detailed differences in pathogenic mechanisms. These results also highlight the importance of delineating the CRS endotypes, which can reveal pathogenic patterns based on the underlying mechanisms.
Cluster analysis of CRS endotypes
Cluster analysis is an unsupervised learning method that can integrate multiple variables to identify unique patient categories. It can be used to categorize heterogeneous disorders into disease subtypes and has recently been employed to identify various inflammatory diseases, such as asthma,223 COPD,224 and obstructive sleep apnea.225 Distinct CRS clusters with diverse inflammatory mechanisms can be used to develop personalized treatment strategies for CRS patients. Nakayama et al.226 identified 4 distinct clinical CRS phenotypes based on the presence of NPs and mucosal eosinophil counts; however, these clusters were not correlated with treatment choices or therapeutic outcomes. Lou et al.227 used unsupervised hierarchical cluster analysis and translated the theoretical stratification into a clinically meaningful stratification. This approach generated 5 distinct clusters (Fig. 2) in a retrospective cohort of 366 Chinese CRSwNP patients thereby providing relevant information on disease recurrence. Plasma cell-dominant and lymphocyte-dominant CRSwNP, showed polyp recurrence in less than 7% of the patients. The clusters indicated that a mixed inflammatory pattern or inflammation characterized by a neutrophil infiltration would indicate poor prognosis with polyp recurrence in 75% and 46.4% of the patients, respectively. Notably, CRSwNP characterized by extensive tissue eosinophilia (tissue eosinophil counts ≥ 54.5%) showed the highest polyp recurrence rate of 98.5%.
 | Fig. 2Representative hematoxylin and eosin staining of nasal polyps in 5 inflammatory phenotypes (400× magnification). (A) Cluster 1, the plasma cell-dominant group. (B) Cluster 2, the lymphocyte-dominant group. (C) Cluster 3, the mixed group. (D) Cluster 4, the neutrophil-dominant group. (E) Cluster 5, the eosinophil-dominant group. Plasma cell, green arrow; lymphocyte, black arrow; neutrophil, blue arrow; eosinophil, red arrow.
|
Using cluster analysis, Tomassen et al.5 described 3 endotypes of CRSwNP and CRSsNP in the CRS samples obtained from 11 European centers. These endotypes showed different expression patterns of Th cytokines, inflammatory biomarkers, and IgE. Based on these findings, CRS can be categorized into, non-type 2 inflammation, and moderate and severe type 2 inflammation, with increased occurrence of NPs and asthma as comorbidity.5 Wang et al.228 evaluated the Th cytokine and marker profiles in the CRS patients from Asia (China and Japan), Europe (Benelux and Germany) and Australia. They demonstrated a remarkable diversity in the Th cytokine signatures between these geographical regions and showed that tissues from the European and Australian CRSwNP patients were characterized by a stronger expression of type 2 inflammation than those from the Asian patients. Conversely, in Asia, the expression patterns were shown to vary from low type 2 expression in Chengdu/China to moderate expression in Beijing and Japan. Accordingly, the percentage of eosinophilic inflammation (ECP/MPO ratio > 1) and SE-IgE levels in the European, Australian and Japanese CRSwNP patients were higher than those in patients from Beijing and Chengdu in China. These differences were reflected in the tissues obtained from the CRSsNP patients. Recently, Liao et al.229 described 7 clusters of CRS patients in central China, with 28 clinical variables and 39 mucosal cellular and molecular variables. The 7 clusters were classified into 3 endotypes: (1)type 2 inflammation with higher levels of Th2 cytokines such as IL-5 and -13, and with severe eosinophilic infiltration; (2)mixed type 1 and 3 inflammation with higher levels of Th1 (IL-12 and IFN-γ) and Th17 (IL-17) cytokines, and moderate levels of IL-5 (Th2 cytokine); and (3)non-type 1/type 2/type 3 inflammation with lower expression of Th1, Th2, and Th17 cytokines.229 A recent study of CRS patients in America identified 6 clusters and suggested that a severe type 2 endotype and a mild type 2 endotype with pro-inflammatory signatures were both present in 15% of the subjects. However, 70% of the patients were characterised by disease with a low overall inflammatory burden but without distinct Th1-, Th2- or Th17-associated signatures.230 Table 3 summaries the endotypes from the different regions from the studies referenced above. Kim et al.231 evaluated the expression of Th cytokines, chemokines and transcriptional factors based on the classification of ECRS (non, mild, moderate and severe ECRS) and found that the upregulation trend of type 2 cytokines (IL-5, IL-13, CCL24 and etc.) and the downregulation trend of type 3 cytokines (IL-17 and IL-22) and the type 1 cytokine (IFN-γ) were associated with an increased prevalence of phenotypes such as asthma and atopy from control to severe ECRS.
Table 3
Endotypes based on cytokine profiles in different regions

| Authors | Regions | Analysis | Parameters | Endotypes | Clinical outcomes |
|---|---|---|---|---|---|
| Tomassen et al.5 | Multicenters in Europe | Cluster analysis with 2 CRS phenotypes together | Mucosal Th cytokines, eosinophilic/neutrophilic markers and IgE | Severe type 2, moderate type 2 and non-type 2 | More CRSwNP and asthma in moderate and severe type 2 |
| Wang et al.228 | Benelux, Germany, Beijing and Chengdu of China, Japan and Australia | Descriptive study for CRSwNP and CRSsNP respectively | Mucosal Th cytokines | CRSwMP: type 2 dominance in Europe/Australia/Japan, mixed type 1, 2 and 3 in Beijing and non-type 1, 2, 3 in Chengdu | Different endotypes driven therapeutic strategy |
| CRSsNP: mixed type 1, 2 and 3 in Benelux, Germany, Australia and Beijing, non-type 1, 2, 3 in Chengdu | |||||
| Liao et al.229 | Middle region of China | Cluster analysis with 2 CRS phenotypes together | Clinical variables and mucosal cellular and molecular variables | Type 2, mixed type 1 and 3 with moderate type 2, non-type 1, 2, 3 | Distinct endotypes of CRS display differences in clinical response to treatments |
| Turner et al.230 | America | Cluster analysis with 2 CRS phenotypes together | Mucosal Th cytokines | Severe type 2, mild type 2 and non-type1, 2, 3 | Diverse endotypes differ substantially with different phenotypes and disease behavior |
CRS, chronic rhinosinusitis; CRSwNP, chronic rhinosinusitis with nasal polyps; CRSsNP, chronic rhinosinusitis without nasal polyps.
![]()
These studies have shown that it is possible to identify CRS endotypes via the key factors that regulate immunity and inflammation in CRS such as Th cytokines and IgE levels. Monoclonal antibodies (mAbs) against type 2 inflammatory factors, such as IL-5, IL-4Rα, IgE and GATA-3 specific DNAzyme, can inhibit type 2 and eosinophilic inflammation and are used to treat conditions associated with airway inflammation such as CRSwNP and asthma.87204205232233 However, these biotherapies target type 2 inflammation and further studies are needed to target the non-type 2 immunity and other factors in CRS.234235236
Precision medicine, which targets key biomarkers, is used for the management of cancer and inflammation,237could be used to manage upper airway diseases such as CRS and rhinitis based on their endotypes.60238239 Moving forward, it is important to determine the mechanisms of CRS and to identify the key regulatory markers with respect to the CRS endotypes.
DIAGNOSIS
Symptoms
CRS (with or without polyps) is defined as an inflammation of the nasal cavity and paranasal sinuses. The symptoms can be categorized into main and secondary symptoms and are important for the diagnosis of CRS. The main symptoms include nasal blockage/obstruction/congestion and nasal discharge (anterior/posterior nasal drip) while the secondary symptoms involve facial pain/pressure and the reduction or loss of smell. Two or more symptoms, one of which must belong to the main category, are required to be manifested for a condition to be diagnosed as CRS.
Nasal obstruction is commonly reported in CRS. Nasal discharge may be anterior or posterior and may present as thick purulent secretions or watery discharge. The incidence of facial pain in CRS patients is variable. NPs, mucosal edema and excessive nasal secretions can physically prevent odorants from reaching the olfactory cleft. Therefore, olfactory disturbance is common. Additional minor symptoms include dizziness, ear pressure, sore and/or itchy throat, cough, and sleep impairment.
Symptom severity in CRS patients can be estimated using a visual analogue scale (VAS) score on a measurable continuum (0–10 cm) or as a grade (no symptoms, mild, moderate or severe symptoms). For example, mild disease is defined by a VAS score of 0–3, moderate as > 3–7, and severe as ≥ 7.240
Physical examination
Physical examination performed using anterior rhinoscopy or nasal endoscopy in combination with symptom assessment can be used to diagnose CRS. Anterior rhinoscopy is the first step in examining patients with chronic sinusitis; however, its use is restricted by the limited illumination and access into the nasal cavity. Nasal endoscopy offers better illumination and visualization compared to that of anterior rhinoscopy and permits a complete examination of the nasal cavities, sinuses, and nasopharynx. It is convenient for observing polyps, edema, discharge, crusting and scarring in the nasal cavities of CRS patients. However, in post-surgical CRS patients, nasal endoscopy does not necessarily correlate with symptoms.241
Radiology
CT is an important auxiliary method for diagnosing CRS, particularly for identifying cells around the frontal recess.242 The characteristics of CRS that are detectable via CT include unilateral or bilateral mucoperiosteal thickening, soft tissue masses, sinus expansion, and osteitis of bony architecture in the affected sinuses.243 In our previous study, we observed intrasinus hyperattenuating masses on CT scans,244 and these features are more prominent in images of the soft tissues. The sinuses were mostly affected bilaterally. CT is increasingly used to assist with endoscopic sinus surgery (ESS), and ESS is often performed based on CT characteristics of CRS. Bone structure and markers identified on CT scans are used as landmarks in ESS. Identifying important structural and anatomical abnormalities pre-surgery will help ensure safety during surgery. Certain features of the soft tissue masses on CT scans can help in differentiating CRS (especially with NPs) from other nasal diseases (such as benign nasal tumors or sinus cysts). Nasal imaging navigator technology is also based on CT. In 1997, Lund et al. 245proposed the Lund-Mackay CT scoring system which is widely used in rhinology. The score ranges from 0‒24 based on the opacification of 10 bilateral sinuses (0 = normal; 1 = partial opacification; 2 = total opacification) and ostiomeatal complex (OMC) (0 = normal; 2 = total opacification). This scoring system allows physicians to quantitatively assess the severity of CRS symptoms and to correlate it with the extent of disease. The Lund-Mackay CT scoring system is simple to use and makes nasal endoscopy more predictable.245
Recent studies have examined the phenotypes of eosinophilic and non-ECRS. These 2 phenotypes show a heterogeneous opacification pattern. Ishitoya et al.246 demonstrated that Japanese patients with ECRS showed ethmoid sinus-dominant opacification while those with non-ECRS showed maxillary sinus-dominant opacification. Once CRS becomes more severe, both phenotypes show a pan-sinusitis pattern.246 A study in China showed that a ratio of ethmoid to maxillary sinuses that was equal to or greater than 2.59 on the Lund-Mackay CT scoring system could be used to pre-diagnose eosinophilic or non-ECRS.247
Magnetic resonance imaging (MRI) shows that mucosal edema and mucus accumulation are the main pathological changes in CRS. T2-weighted images show extended hyperintense signaling in the affected sinuses, which represent the inflamed mucosa. In ECRS, differences in the signal intensity are sometimes observed on T2-weighted images; these are caused by variations in the concentrations or the water-free content of the sinus secretions.248 MRI is not routinely used to examine CRS patients unless the unilateral sinus is affected.
Nasal cytology in CRS
Nasal cytological testing is used to assess inflammation in nasal cavities and sinuses. Samples are obtained by nasal swabbing, brushing or lavage. Liquid-based cytology can exclude the mucus in nasal secretions, providing a cleaner background for observation.249
Nasal cytological testing is non-invasive, simple to perform and convenient for evaluating different types of inflammation in the nasal mucosa. Both total inflammatory cell counts and individual inflammatory cell types in the secretions are closely correlated with those in the mucosa of the inferior nasal turbinate. The sensitivity and specificity of cytological testing during inflammation of the nasal mucosa is 94.1 and 76.9%, respectively.249
Nasal cytology is also important in the diagnosis and treatment of patients with NPs. Eosinophil numbers in nasal secretions and polyp tissues are significantly correlated.250 Nasal cytology helps to differentiate whether or not NPs are accompanied by allergic rhinitis.251
Cytological testing is not fully accepted for diagnosing CRSwNPs. In children with rhinosinusitis, inflammatory cell numbers are higher, and the ratio between ciliated and goblet cells is reversed compared to that in the controls.252 Nasal cytological testing is unsuitable for assessing inflammation in sinusitis as indicated by a low sensitivity of 63.4% and by the lack of a significant correlation between the total and individual inflammatory cell counts in the paranasal sinus mucosa.249
DIFFERENTIAL DIAGNOSIS
AFRS
Whether AFRS is truly a unique disease is debatable.6 AFRS is not clinically distinct from eosinophilic mucus CRS253 and may eventually be renamed as eosinophilic fungal CRS. Nevertheless, in 1994, AFRS was defined using the classic Bent-Kuhn criteria as follows254: (1) nasal polyposis, (2) type I hypersensitivity, (3) eosinophilic mucin without fungal invasion into the sinus and bone tissue, (4) fungi detectable by staining and (5) characteristic radiological findings. These criteria can be used to distinguish between AFRS and CRS.
AFRS is predominantly observed in adolescents and young adults255 and is more common in geographical areas that have high humidity.256 Patients with AFRS are usually atopic to various fungi, show IgE sensitization, and tend to have concomitant asthma and recurrent rhinosinusitis/NPs, and undergo recurrent surgeries. The symptoms of AFRS are similar to those of CRS, including recurrent nasal obstruction, rhinorrhea, and postnasal drainage. The mucin produced in AFRS has a thick, “peanut butter-like” appearance, and is brown and occasionally bloody with crusty casts. This mucin expands, resulting in facial asymmetry and proptosis. Treatment with antihistamines and nasal corticosteroid sprays is often inadequate.257
Sensitization can be assessed via laboratory testing. Total IgE titers are typically higher in AFRS than in CRS.258 Moreover, AFRS exhibits a unique appearance on radiological images. The accumulation of iron, manganese and other elements in the mucus allows for the detection of sinus opacification and calcification via CT.259 There is also a sheet area of high-attenuation, having an appearance of “ground glass” within the sinuses.260 Often, bone thinning and erosion are observed as an expansive lesion, secondary to the accumulation and expansion of the mucus. Bony invasions are generally not present.261 A mixed or high-intensity signal on T1-weighted sequences can be observed using MRI, whereas a signal void or low signal intensity is observed on the T2-weighted sequences.
AFRS is only diagnosed after ESS262 because histopathology is required for the diagnosis of the condition. Pathologically, eosinophilic mucus rich in inflammatory debris and Charcot-Leyden crystals is the hallmark of AFRS. The causative fungi are identified via histological evaluation using Gomori methenamine silver staining and fungal cultures.
Aspirin-exacerbated respiratory disease (AERD)
CRSwNP may be accompanied by asthma and aspirin intolerance in a syndrome called AERD. It is a clinical triad of nasal polyposis, asthma, and respiratory hypersensitivity to NSAIDs, specifically aspirin. Samter and Beers266 further described it in 1968. Therefore, AERD was previously called and “Samter's Triad.”
AERD occurs in 9%-10% of patients with nasal polyposis.267 A cohort study in China revealed that the prevalence of AERD is much lower in Chinese CRS patients (0.57%) than in individuals of European descent.268 The average age of onset is 34 years, and women are more prone to develop AERD than men; AERD is very rare in children.269
AERD is a discrete disorder that occurs within another distinct disease and is therefore different from most other medical conditions.270 Thus, this syndrome is often missed unless evaluations for asthma and aspirin hypersensitivity are performed in patients with nasal polyposis.
The mechanisms underlying AERD are unclear, but they are hypothesized to involve the inhibition of cyclooxygenase 1 (COX-1). Respiratory reactions occurring within 0.5–2 hours of the ingestion of a COX-1 inhibitor are the most prominent and definitive features distinguishing patients with AERD from those with CRSwNP.271 Thus, it is crucial to obtain the medical history of CRSwNP patients, especially for those with anosmia and/or recurrent NP, to establish whether they have aspirin intolerance. An aspirin provocation test can be used to confirm the diagnosis.
Aspirin desensitization is the most beneficial therapy for AERD patients. Other therapies, including the avoidance of aspirin and other NSAIDs, are ineffective. Functional ESS (FESS) can be useful for AERD patients, but NP regrow rapidly after surgery. Moreover, additional studies are required to demonstrate the differences between Chinese and Caucasian populations with respect to AERD.
IgG4-related CRS
IgG4-related CRS has recently been proposed as a new clinical entity272 although its characteristics have not been widely investigated. Currently, IgG4-related CRS is mainly diagnosed using the criteria that are used for the IgG4-related disease (IgG4-RD), a systemic, immune-mediated condition that affects various organs.273274 The 2011 Boston criteria proposed that the histological diagnosis of IgG4-RD be based on the presence of characteristic morphological features, including lymphoplasmacellular inflammation, storiform fibrosis, obliterative phlebitis, prominent IgG4-positive plasma cells, and an IgG4-/IgG-positive ratio of > 40%.275 Conversely, the development of IgG4-RD in the nasal cavity and paranasal sinuses is relatively rare, and published data on IgG4-RD in these sites is both limited and controversial. Moteki et al.272 first described IgG4-related CRS in 2011. They assessed serum IgG4 levels and performed immunohistochemical labeling for IgG4 in nasal mucosal tissues from patients with IgG4-related CRS and common CRS. Their results indicated that increased serum IgG4 levels, but not positive staining for IgG4 in the nasal mucosa, was a diagnostic factor for IgG4-RD. Piao et al.276 have shown that increased concentration of serum IgG4 and infiltration of IgG4-positive plasma cells into the nasal mucosa of patients with Mikulicz's disease occurs more in IgG4-related CRS (MD-CRS) than in MD or common CRS alone. They further suggested that IgG4-positive plasma cells should be assessed histopathologically when establishing a differential diagnosis of IgG4-related CRS. A comprehensive evaluation of the clinical symptoms, serum IgG4 levels, and infiltration of IgG4-positive plasma cells can provide an accurate diagnosis of IgG4-related CRS.277
Benign tumors
In this section, we have summarized and reviewed the differential diagnoses of benign and malignant tumors that mimic CRS and CRSwNP. These benign and malignant tumors can appear in any area of the nose, and therefore, it is crucial to perform imaging before the initiation of any intervention; for the best results, imaging should involve biopsy.
Epithelial tumors
Inverted papilloma, the most common benign tumor occurring within the middle meatus, may extend into the nasal cavity and sinuses. The clinical features include bloody nasal discharge, unilateral lesions, dendritic protrusions and limited growth. Endoscopic surgery is an effective approach for removing nasal inverted papillomas with minimal invasiveness, but this tumor shows high recurrence. Pathological examination of the surgical margins can be used to partially predict the prognosis.278 Salivary gland tumors and pleomorphic adenomas may occur concurrently within the nose and sinuses, but such occurrences are uncommon.279
Mesenchymal tumors
Fibroma and angiofibroma occur almost exclusively in adolescents presenting with nasal obstruction and epistaxis.280 Less common mesenchymal tumors include schwannomas,281 neurofibromas,282 meningiomas,283 leiomyomas,284 angioleiomyomas285 and other benign nasal tumors that can be identified via histological evaluation and imaging of biopsy samples.
Malignant tumors
Malignant tumors, such as squamous cell carcinoma or mucinous adenocarcinoma, can mimic CRS within the nose and sinuses. The early clinical signs and symptoms of sinonasal malignant tumors include unilateral and progressive nasal congestion, bloody discharge, and nasal discharge with malodorous pus; these may be accompanied by headache, epiphora and dysosmia. A definite diagnosis is made by pathological biopsy. Squamous cell carcinoma286 is the most common malignant tumor of the sinonasal region, but mesenchymal tumors must also be suspected until proven otherwise.
MANAGEMENT
Medical treatment
Corticosteroids
Glucocorticoids have anti-inflammatory and immune suppression effects, and are consequently, the most important drugs against CRS287; they can be used both orally and topically. Short-term treatment with oral steroids, called “medical polypectomy,”288289 significantly reduces polyp size and alleviates symptoms. However, the effects of oral steroids on CRSwNP are not maintained for a long time. This is exemplified by oral methylprednisolone. Its effect on polyp size peak at week 3, but after 2 months, polyps recur.202 Oral steroids can also generate adverse effects including inhibition of adrenal axis function, slowed growth, osteoporosis and gastrointestinal discomforts. Contraindications should be evaluated before starting treatment with oral steroids, and potential side effects must be monitored during therapy. In CRSsNP, short-term treatment with systemic steroids has gradually reduced and replaced with treatment with topical steroids. The frequent use of systemic steroids is not recommended because of the potential adverse effects. There are no recommendations for oral corticosteroid use in CRSsNP, because currently there are no clinical data to confirm their efficacy and because of the potential side effects of a systemic steroid therapy.290
To the best of our knowledge, numerous randomized controlled trials (RCTs) have reached a consensus on using nasal steroids for CRS (designated by grade A recommendation) has been reached via,287290291 and nasal steroid sprays are commonly used in clinical practice. Local side effects of steroid nasal sprays include epistaxis, dry nose, septal perforation, and nasal cauterization and irritation, but these occur at low rates. In clinical trials, corticosteroid-treated groups and control groups show no significant differences with respect to the adverse events, and the systemic side effects of the nasal corticosteroids remain debatable.292 Early studies have suggested that beclomethasone propionate, a corticosteroid nasal spray, affects growth, and that this may be related to its high bioavailability.292 Fluticasone furoate and triamcinolone acetonide have been reported to cause a small, but not statistically or clinically significant, decrease in growth.293 However, fluticasone propionate may suppress the hypothalamic pituitary-adrenal axis.293 There is no evidence that nasal steroids increase the risk of developing cataracts, glaucoma, or elevated intraocular pressure.
Nasal corticosteroids cannot rapidly alleviate symptoms and reduce mucosal inflammation, and should, therefore, be used for > 12 weeks to maintain efficacy. Steroid drops, irrigation, and inhalation are also used in clinical practice. Intranasal nebulization with a budesonide suspension for 2 weeks alleviates nasal symptoms, reduces polyp size, and downregulates inflammatory factors and tissue remodeling in eosinophilic CRSwNP with no significant effects on the function of the adrenal cortex and no serious side effects.
Intranasal nebulization with budesonide 1 mg BID, which differs from nasal steroid sprays and oral pills, is a safe and effective way to treat patients with NPs and can be used as a conventional perioperative therapy against NPs.294 No systemic side effects have been observed in asthma patients treated with nasal sprays and inhaled steroids.292 Nasal irrigation with budesonide was once assessed for use in CRS,295 but long-term safety and efficacy of this application needs further study.
Due to the heterogeneity of CRS, patients with different endotypes show different responses to drugs.227 Some patients show a poor or lack of response to standard steroid therapies287; this is known as glucocorticoid resistance. The mechanism of glucocorticoid resistance in CRS is unclear. Increased expression of phosphorylated glucocorticoid receptor (GR) α or that of its competitive receptor GRβ would interfere with the anti-inflammatory effects of glucocorticoids. Downregulation of GR expression, which occurs post glucocorticoid treatment may cause secondary glucocorticoid resistance.287 Unlike eosinophilic CRSwNP, CRSwNP with increased neutrophilic inflammation is less responsive to glucocorticoid treatment,296 indicating that different CRSwNP endotypes show different responses to glucocorticoids.
Macrolides
Macrolides are antibiotics containing a 14-, 15- or 16-membered macrocyclic lactone ring. Orally administered macrolides show good bioavailability and tissue penetration. They are active against most gram-positive bacteria, some gram-negative bacteria, mycobacteria, chlamydia, Legionella spp., and mycoplasma.299300 In 1990, Suzuki et al.301 found that long-term low-dose erythromycin therapy in patients with diffuse pan-bronchiolitis improved the 10-year survival rate and relieved CRS symptoms; this promoted the use of macrolides as new treatment options in CRS. Macrolide activity against CRS involves anti-inflammatory and immunomodulatory mechanisms including the inhibition of NF-κB, pro-inflammatory cytokines (IL-8, IL-5, IL-6 and IL-1) and oxygen radicals, expression of granulocyte adhesion factor; enhancement of mucociliary activity; and decreasing the formation of bacterial biofilms.302303304305306 In 2007, macrolide therapy received an A-class recommendation form the EP3OS for the treatment of CRSsNP.307 However, macrolides show no effects in patients with high levels of IgE or those with NPs or asthma. Additionally, long-term treatment with macrolides may result in bacterial resistance. Based on the data by Wallwork et al.308 and Videler et al.309 the EP3OS recommendation was downgraded from A to C in 2012.6
Macrolides and nasal steroids exert similar clinical effects in CRSsNP patients; both can alleviate subjective or objective symptoms and improve endoscopic scores.310 The CRSsNP phenotype in Chinese adults differs from that in patients of European descent. The cytokine profile of the Chinese CRSsNP is Th1-dominant with non-eosinophilic inflammation82; macrolide-based treatments are more effective for this endotype. Therefore, long-term, low-dose macrolide therapy is recommended for CRSsNP patients with neutrophilic inflammatory patterns and low IgE levels.308311 Oral or nasal steroids and surgery remain the preferred therapy for CRSwNP patients. Long-term, low-dose macrolide therapy post-surgery can improve the subjective or objective symptom score, shrink polyp size, and delay polyp recurrence.312313314 Lou et al.227 identified 5 clusters of NP including plasma cell-dominant, lymphocyte-dominant, mixed inflammatory-cell type, neutrophil-dominant, and eosinophil-dominant. Some CRSwNP patients are not sensitive to steroid therapy; this may be due to the presence of different NP phenotypes. Long-term, low-dose macrolide therapy is recommended for treating corticosteroid-resistant CRSwNP patients, neutrophil-dominant NPs, the persistent edema of nasal mucosa, and purulent nasal discharge.315316 In a previous meta-analysis conducted using a non-RCT study,317 we found significant differences between the endoscopic scores of the control group and those of the groups treated with macrolides for 8 weeks (standardized mean difference [SMD], −0.77; 95% confidence interval [CI], −1.07, −0.46; P < 0.00001) and 12 weeks (SMD, −1.04; 95% CI, −1.97, −0.82; P < 0.00001). In 2 non-RCT studies, the CT scans revealed a significant improvement after 12 weeks of treatment with macrolides (mean difference, −5.81; 95% CI, −8.10, −3.52; P < 0.00001). Additionally, Asian and non-Asian subgroups were assessed in 5 RCT studies using a Sino-Nasal Outcome Test (SNOT) after 12 weeks of macrolide therapy; the treated and control Asian subgroups showed significant differences (SMD, −0.51; 95% CI, −0.99, −0.02; P = 0.04) while no differences were observed between the control and treated non-Asian subgroup (SMD, −0.01; 95% CI, −0.65, 0.63; P = 0.98).
Clarithromycin, azithromycin, and roxithromycin are some of the widely used macrolides. Compared to the doses used for acute infections, the daily dose of macrolides during the treatment of CRS is halved, and the treatment period lasts generally 12 weeks. Long-term, low-dose macrolide therapy is considered safe.6 However, inclusion and exclusion criteria require careful consideration as do the possible adverse events, including bacterial resistance, cardiovascular effects, gastrointestinal reactions, hearing loss, allergies, and liver damage.
Antimicrobial therapy for CRS
No clinically controlled trial has examined the effect of antibiotics vs. placebo in the treatment of CRSsNP. Published clinical trials have shown no significant differences between the effects of the various antibiotics tested (mostly cefuroxime, amoxicillin-clavulanic and ciprofloxacin).318319 Several RCTs have reported that doxycycline can alleviate certain symptoms of CRSwNP.217 Currently, there is no evidence supporting the use of CRS (CRSsNP and CRSwNP) patients with antibiotic therapy in CRSsNP or CRSwNP.320 Studies have shown that bacterial infection is not a determining factor in CRS pathogenesis.72 However, antibiotics are recommended for conditions similar to acute bacterial rhinosinusitis, exacerbated CRS with evidence of bacterial infection, and orbital and intracranial complications that occur in CRS. Clinically, empirical therapy uses broad-spectrum antibiotics (mostly amoxicillin-clavulanate potassium, and new generation cephalosporin and quinolone) to target gram-positive, gram-negative, and anaerobic organisms, while EP3OS recommends culture-directed therapy with susceptibility testing using the commonly prescribed dosages and a treatment duration of < 2 weeks. Although fungi can contribute to the pathogenesis of ECRS, clinical trials indicate that antifungal therapy is not beneficial and may potentially result in severe adverse effects. Therefore, antifungal therapy is not recommended for CRS.321
Other medical treatments
1) Leukotriene receptor antagonists (LTRAs)
In the pathophysiology of allergic diseases, cysteinyl leukotrienes (CysLTs) act as modulators and mediators via distinct receptors (CysLTRs) while antileukotrienes are important in therapies against allergic rhinitis and asthma.3322 CysLTs play more important roles in ECRS than in non-ECRS,323324 and LTRAs have been shown to be effective in treating ECRS.325326 CysLTs and CysLTRs are significantly enhanced in CRSwNP patients, particularly in those with IL-5+ NPs compared to those in CRSsNP patients and the healthy controls. LTRAs, such as montelukast, can downregulate cytokine and mucin expression in polyp explants, and thereby alleviate the symptoms of recalcitrant CRSwNP.327
Intranasal corticosteroids (INCSs) is an effective drug against CRSwNP, but it cannot inhibit all the cytokines and inflammatory transmitters involved in the formation of the NP. INCSs show a limited impact on leukotriene-mediated airway inflammation, but supplementation with LTRAs can improve clinical outcomes327328329330331 and is an ideal complementary-treatment strategy. A meta-analysis showed that LTRAs are superior to placebos with respect to the alleviation of CRS symptoms.332 Compared to the placebo, LTRA significantly improved the symptoms, polyp size, and immunologic parameters, including eosinophilia, in the CRSwNP patients. Postoperatively, LTRAs are also effective when combined with INCSs and can reduce facial pain/headache, nasal itching, sneezing, postnasal drip, and olfactory impairments. Combinatorial therapies with LTRA and INCSs can reduce the symptoms but not the general severity of CRSwNP, and they do not have any effect on asthma, AERD, or atopy. It seems that LTRAs may provide additional benefits to INCS for symptom management but not for reducing its general severity. Meanwhile, the outcomes seem to be unaffected with regards to the generalized status of asthma, AERD, and atopy.
ESS does not reverse the progression of mucosal inflammation; therefore, a local or systemic therapy is used instead. A clinical study evaluated the effects of montelukast (10 mg) and mometasone furoate nasal spray (400 μg) on the postoperative course of nasal polyposis.333 The SNOT-22 scores were reduced in both groups at the 6-month follow-up with the mometasone furoate group showing a marginal advantage with respect to the recurrence rate. Another prospective, randomized, open-label trial was used to evaluate the effectiveness of using montelukast as an adjunct to the INCS-based therapy after ESS for the CRSwNP patients.334 INCS was assessed as a monotherapy and in combination with montelukast for 1 year. The results indicated that the subjective and objective scores were significantly reduced in both INCS monotherapy and INCSs in combination with montelukast groups with no significant differences. More RCT studies are required to evaluate LTRAs in the treatment of CRS.
2) Antihistamines
Antihistamines bind to H1 receptors are used to treat allergic diseases. Second-generation oral and intranasal H1-antihistamines are recommended as the first-line of treatment for allergic rhinitis because they show weaker sedative effects and stronger anti-inflammatory effects than first-generation H1-antihistamines.335 The second-generation oral H1-antihistamine, desloratadine inhibits eosinophilic inflammation in NPs; these effects of desloratadine may be augmented by mometasone furoate.336 To date, no RCTs have evaluated H1-antihistamine therapy in adults or children with CRS. Current data are insufficient to determine whether oral or intranasal H1-antihistamines can be used to treat CRS patients without allergic rhinitis.
3) Mucolytics
Mucolytics are used for the treatment of rhinosinusitis as they have mucolytic, secretolytic, anti-inflammatory, antibacterial, antiviral, and immunological activities.337338339 The herbal dry extract, BNO 1011 is based on a combination of 5 herbs that can significantly improve radiographic, histological, and MCC parameters in a rabbit model of CRS.142 Daily treatment with BNO 1016 (Sinupret extract, a combination of 5 botanical drugs) for 12 weeks has been shown to be clinically safe and effective.340 However, a systematic review reported limited evidence regarding whether the herbal medicinal products, including Sinupret, are beneficial for the treatment of rhinosinusitis, particularly CRS.341 Web-based nationwide surveys show that oral mucolytics are commonly used by a majority of Chinese otolaryngologists (69%) for postoperative treatment of CRS.342 However, more evidence-based studies are needed to further evaluate this approach.
4) Decongestants
Nasal obstruction is common in CRS. The main function of decongestants is to shrink blood vessels and reduce the volume of the inferior and middle turbinates.343 Before the use of INCSs, decongestants were used to reduce nasal edema and expand the nasal cavity344 and thereby improve the distribution and efficacy of the INCS. Combinatorial therapy with INCS and oxymetazoline for 6 weeks was more effective than INCS monotherapy at alleviating nasal obstructions and disturbances in smell, improving MCC, and reducing polyp size in CRSwNP.345 Decongestants can be further subdivided into intranasal (spray or drops) and oral medications. Generally, short-term treatments (usually < 7 days) with nasal decongestants will help avoid the rebound effects that cause rhinitis medicamentosa. However, the current evidence does not support the use of oral decongestants in CRS.
5) Bacterial lysates
Bacterial lysates stimulate non-specific defense mechanisms and general immunity, leading to increased immunoprotection. Oral bacterial lysates can minimize the risk of recurrent respiratory infections in children and adults and reduce the severity of airway-related symptoms and the number of infections requiring antibiotic treatment.346 OM-85 BV (Broncho-Vaxom), an orally applicable bacterial lysate, possesses ciliostimulatory and immunogenic properties that may be partially responsible for its efficacy as a therapeutic agent for respiratory disorders.347 The effects of OM-85 BV as an adjunctive treatment in CRS have been demonstrated in mice.348 Additionally, a multi-centric, placebo-controlled, double-blind clinical study indicated that the oral administration of OM-85 BV can be used as an adjunct to standard therapies in adults for CRS.349 Bacterial lysates used during CRS remission in children can provide long-term prophylaxis, and effectively decrease the frequency of rhinosinusitis attacks.350 Generally, oral bacterial lysates are adjunctive drugs that are cost-effective and show good safety and few adverse reactions. However, further clinical trials are needed to evaluate this class drug.
Nasal irrigation
Nasal irrigation or nasal washing/douching/lavage is a simple, inexpensive, and well-tolerated procedure that has been used by otolaryngologists for treating rhinitis and sinusitis, for over a century.351 Nasal irrigation can increase MCC, alleviate mucosal swelling, dislodge thick secretions, remove local inflammatory mediators, allergens, and infective debris, reduce postoperative crusting, and moisten the sinonasal cavities. Because of its confirmed effectiveness and safety, nasal irrigation is recommended as a supplementary therapy in CRS. Various solutions consisting of solo isotonic and hypertonic saline, dead-sea salts, or those including topical corticosteroids, antibiotics, or natural substances are used for nasal irrigation.352353354 Compared to the common methods of nasal delivery, high-volume nasal irrigation is better able to deliver and maximally distribute topical medications to the sinus mucosa.355
In 2007, a study published on the Cochrane library demonstrated that irrigation with nasal saline is well-tolerated and alleviates the symptoms of CRS to a greater degree than the placebo, thereby improving QoL as assessed by using the disease-specific QoL (DSQOL) questionnaire.356 A recent review in the Cochrane library demonstrated improvement in DSQOL of CRS patients after a minimum of 3 months of high-volume nasal irrigation with hypertonic saline compared with that of the placebo; however, 23% of the treated individuals experienced adverse reactions including epistaxis.357 A twice daily regimen of nasal irrigation with a solution of 0.05% mupirocin and Ringers salts markedly reduced the VAS, DSQOL, and endoscopic findings in the most recalcitrant CRS patients.358 Although this clinical application is off-label, the efficiency and safety of nasal irrigation with corticosteroids is being evaluated.353 In 2009, the first study on high-volume nasal irrigation with budesonide reported that 75% of the CRS patients subjected to the treatment showed significant improvements in their VAS and endoscopic scores.295 No adrenal suppression was detected after 1 mg of budesonide in 120 ml of saline was administered twice daily for 60 days.359
Nasal irrigation plays a crucial adjunctive role in post-ESS care. At present, nasal irrigation using a saline solution is considered to be effective for preventing purulent rhinorrhea, granulation, and polyp recurrence after ESS.360 Nasal irrigation with budesonide is also an effective postoperative therapy for patients with NP and asthma as evidenced by decreased DSQOL and Lund-Kennedy scores and reduced intake of oral steroids.361 Furthermore, 83% of the difficult-to-treat CRS patients exhibited satisfactory alleviation of their subjective symptoms, and 75% of the patients showed improvement in DSQOL and endoscopic scores after 500-mL irrigation with 1 mg budesonide in a saline solution, twice daily for 3 months.362
Surgery
Procedures
Surgical intervention is used to treat CRS patients who are unresponsive to the maximal medical treatments after they have been administered for at least 12 weeks.363 Twenty years ago, Naumann364 described the OMC, which has become the anatomical basis for FESS, which is considered to be the first option for surgical intervention in CRS.
FESS can provide immediate and long-term symptom relief, and can improve QoL in 85% of the patients.365 FESS involves the clearance of polyps and polypoid mucosa and the opening of the sinus ostia with the protection of normal and edematous mucosa. In FESS, CRS symptoms are alleviated by the removal of inflammatory tissues (including the mucosa and the underling bone), reduction of the antigenic load that triggers inflammation, and improvements in sinus ventilation and MCC. ESS is classified into routine and revision surgery based on changes in the pathophysiology of CRS patients. Major complications of surgery include cerebrospinal fluid leak, meningitis, hemorrhage and orbital injuries. The extent of FESS varies from uncinectomy to sphenoethmoidectomy with and without middle turbinate resection.
1) Surgical indications
ESS is considered for CRS that is unresponsive to medical intervention, complicated acute sinusitis, allergic fungal sinusitis, mucoceles and symptomatic polypoid disease that is inadequately managed by other medicines,.
2) Preoperative evaluation
Endoscopy
Endoscopic evaluation of the anatomy or lesions is important before surgery, particularly in patients who have had prior surgical intervention. It is necessary to determine whether the 0-degree 4-mm telescope can be introduced into the nose and bilaterally advanced to the anterior attachment of the middle turbinate. If the 0-degree telescope cannot be introduced into this region, septoplasty is required during surgical intervention.
Imaging
It is essential to re-review a patient's CT scans before surgical intervention and preferably shortly before the surgery. Standardized methodology should be used to review the scans to ensure that no significant anatomic variations are missed. Although CT is the primary diagnostic modality for sinus disease, preoperative MRI is recommended for some sinus disorders, including complications of acute or chronic sinusitis, allergic fungal sinusitis, mucocele or tumors. Imaging via MRI is vital when differential diagnosis is necessary, and the disease is adjacent to the skull base erosion. Evaluation of dehiscent areas in the sphenoid sinus is very important for excluding the possibility of a carotid artery aneurysm.
3) Surgical principles
FESS is primarily aimed at reopening the dependent sinuses and at reestablishing drainage and ventilation of the sinuses. With the advent of through-cutting forceps, microdebriders, and improved hand instrumentation, the removal of diseased tissue and bone is now achieved with good mucoperiosteal preservation. The extent of FESS varies from simple uncinectomy to a complete sphenoethmoidectomy, antrostomy, and frontal sinusotomy. Extended frontal sinus procedures are generally not performed during the first surgery. However, when the involved mucosa and bone represent an inflammatory burden, the effect of FESS is limited, and radical endoscopic surgery is required.
Uncinectomy
Uncinectomy is usually the first step in ethmoidectomy. This procedure begins with dissection using a sickle knife or backward cutting “sewing door technique.” The upper part of the uncinate process is used as an anatomical landmark for orientation of the drainage pathway of the frontal sinus and for exposing the ostium of the maxillary sinus (Fig. 3).
 | Fig. 3Endoscopic view of an uncinectomy. (A) An incision was made with a sickle knife or elevator, along the anterior margin of the UP. (B) The EB was exposed after the removal of the UP, and natural ostium maxillary sinus (↑) can be observed.NS, nasal septum; MT, middle turbinate; UP, uncinate process; EB, ethmoidal bulla.
*Upper attachment of UP.
|
Ethmoidectomy
After the uncinectomy, the anterior wall of the ethmoidal bulla, the second lamella, can be observed and removed up to the basal lamella of the middle turbinate. The posterior ethmoidal cells can be cleared after resecting the basal lamella. The Onodi cell usually indicates the last posterior ethmoidal cell. The lateral wall of the ethmoidal sinus is the lamina papyracea. Dehiscence in the lamina can be identified once the lamina papyracea is identified and cleaned of cells (Fig. 4).
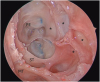
Sphenoidectomy
The sphenoid sinus can be opened using transethmoidal and transnasal approaches. The lower third superior turbinate, an important landmark for locating the ostium through the superior meatus, can be removed; the ostium of the sphenoid sinus medial to the attachment of the superior turbinate can then be identified (Fig. 5). The anterior wall can then be resected through the natural ostium using the Kerrison punch. The transnasal approach often begins with a partial resection of the inferoposterior middle turbinate or lateralization of the middle turbinate; the sphenoid sinus is then opened using the technique used in the transethmoidal approach.
 | Fig. 5Endoscopic image of the cadaver shows that: (A) After partial superior turbinectomy, the ostium of the SS (↑), located medially to the remnant ST (△△△), was well exposed; (B) the SS was opened by a Kerrison punch.ST, superior turbinate; SS, sphenoidal sinus; PE, posterior ethmoidal sinus.
*Lamina papyracea.
|
Frontal sinus surgery
The endoscopic frontal recess approach (Draf I frontal sinus surgery) is the primary means of managing chronic frontal sinusitis. Only the septal cells in the frontal recess need to be removed to improve the drainage and ventilation of the frontal sinus (Fig. 6). This approach is considered when only minor pathology is present in the frontal sinus.
 | Fig. 6Postoperative endoscopy and images demonstrate Draf type frontal sinus surgeries: Draf I, II (a, b) and III. FS (↑).FS, frontal sinus.
|
Extended frontal sinus drainage is achieved after an ethmoidectomy by resecting the floor of the frontal sinus between the lamina papyracea and the middle turbinate (Draf II a) or nasal septum (Draf II b) anterior to the ventral margin of the olfactory fossa. Indications for Draf IIa include moderate or severe mucosal pathology, benign tumors, and mucocele. Draf II b is utilized when Draf IIa fails or for treating benign tumors or recurrent polyps with hyperplastic bones in the frontal recess. For Draf IIb, the frontal process of the maxilla and frontal beak are removed by drilling.
Draf III, also called the median drainage procedure, is accomplished by resecting portions of the superior nasal septum, interfrontal septum, cells in the frontal recess, and the frontal sinus floor. Identifying the first olfactory fibers on both sides helps to achieve a maximal opening of the frontal sinus. Indications for Draf III vary and include failed ESS, osteogenesis in the frontal recess, and frontal ostium, frontal recess adhesion366367 and benign and malignant tumors.
4) Revision surgery
Revision surgeries for recurrent CRS are based on the different pathogenic backgrounds. In revision surgery, key anatomic landmarks may be altered or missing, increasing the risk of severe complications, such as orbital injury, cerebrospinal fluid leak, and excessive bleeding. The middle turbinate, a commonly used landmark, may be altered or removed. During revision sinus surgery, preservation of the mucosa helps to avoid exposing the underlying bone, which can result in osteoneogenesis and osteitis. Radical endoscopic surgery (RES) is indicated368 when the sinus mucosa and bone represent an inflammatory burden,193 such as in CRSwNP and comorbid asthma, aspirin intolerance, and recurrent CRSwNP with or without the hyperplastic ethmoidal bone. These patients often exhibit high levels of eosinophils in their peripheral blood and/or mucosal tissue, high levels of specific IgE, and NPs in the middle turbinate and septum, which are the risk factors for recurrent CRS.
RES, which includes nasalization, extensive opening of the maxillary and sphenoid sinuses, and Draf IIb or III type frontal sinus surgeries, are the most common procedures in revision surgery (Fig. 7). Although these procedures are controversial, follow-ups have shown satisfactory outcomes.369 Surgery is only the beginning of the treatment; long-term periodical follow-ups and sustained medical therapies should be performed based on the pathophysiology of the chronic sinus disease.370371
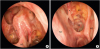 | Fig. 7Postoperative endoscopy. Well-epithelized nasal cavity after nasalization using the Draf III procedure. (A), endoscopic view of bilateral frontal sinuses and ethmoid sinuses. (B), endoscopic view of left ethmoid sinus, sphenoid sinus and maxillary sinus.FS, frontal sinus; ES, ethmoidal sinus; SS, sphenoidal sinus; MS, maxillary sinus, NS, nasal septum.
*Middle turbinate.
|
Surgery in CRS with asthma
Asthma is commonly concomitant with CRSwNP and CRSsNP. In CRS patients undergoing ESS, the prevalence of asthma is 10% compared to a 1% prevalence in the general adult population.372373 The prevalence of asthma in Chinese CRS patients is lower than that in patients of European descent.26374 Sinus disease is more severe in CRS when asthma occurs as a comorbidity. These patients develop earlier and more severe olfactory dysfunctions and show higher CT olfactory scores.372 There are no differences between the asthmatic and non-asthmatic CRS patients with respect to total nasal resistance or bilateral nasal cavity volumes when assessed by acoustic rhinometry.375 Consistently, these patients have more severe asthma, and most are refractory to medical treatments. ESS is the mainstay for severe CRS with asthma. Asthma could be considered a risk factor for the most negative outcomes of ESS,376377 but this is up for debate.378379 Patients with both CRS and asthma might benefit from extended ESS. Chen et al.380381 found that symptoms and endoscopic scores in CRS patients with asthma were improved significantly at the 1- and 3-year postoperative follow-ups (Fig. 8). Compared to FESS, extended ESS (partial middle turbinate and superior turbinate resection) showed better endoscopic appearance and olfactory symptom VAS scores in patients with CRS and asthma, postoperatively.382 Alsharif et al.383 proposed a reboot technique for type-2 CRSwNP. The aim of this technique was to maximally remove all the sinus mucosa and allow for a healthy re-epithelialization from the preserved nasal mucosa. They found that their reboot technique reduced the recurrence of NP in a 30-month follow-up.
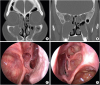
Perioperative management and follow-up
Perioperative management of chronic CRS includes surgery, medications, and other treatment strategies, 1 to 2 weeks before surgery, and 3 to 6 months after surgery.
Preoperative management
Preoperative management (conducted for 7 to 14 days) involves the control of infection and inflammation in the nasal cavity and/or sinuses and the management of conditions such as hypertension and coagulation dysfunction. Preoperative management is meant to improve surgical safety.384 Rules regarding these medications are outlined in section 8.1. Drugs and foods such as anticoagulants, aspirin and ginseng that can cause intraoperative bleeding should be discontinued at least 5 days prior to surgery.385
Blood pressure should be maintained under 150/95 mmHg for 3 to 5 days. Fasting blood glucose levels should be <9.0 mmol/L. For patients with heart, lung, liver, or kidney dysfunctions, laboratory results should be in accordance with the requirements of general anesthesia.
Intraoperative management
The goal of intra-operative management is to assess the patient using a sinus CT, endoscope, and other correlated examinations.386 Minimally invasive surgery and function-conserving management should be considered. The choice of nasal packing and packing material should be left to the surgeons.387388
Postoperative follow-up
Successful ESS in CRS is only a part of the therapeutic approach as postoperative follow-ups and comprehensive therapy are also essential in CRS.389 Postoperative therapies for CRS can be divided into 3 stages, cleaning, mucous transition, and epithelialization. Postoperative mucosal morphology and functional recovery usually require 3 months or more, and comprehensive therapy is necessary during this period.13 The principles of postoperative medication have been described in section 8.1.
Efficacy evaluations help to analyze the course of therapy and that of the disease via subjective and objective methods. Assessment of VAS, Lund-Mackay and Lund-Kennedy scores is recommended for CRS patients. SF-36390 and SNOT-20391 are also suggested and provide more comprehensive and scientific information.392
Evaluation and prediction of surgical outcome
ESS, the standard surgical intervention for CRS,287393 is effective and safe.394395 A systematic review393 reported that ESS leads to symptomatic improvements in up to 98% of CRSwNP patients with a low frequency of major complications. Another review showed 91% symptom improvement rates after ESS.396 The 22-item version of the SNOT-22 can predict the likelihood of postsurgical symptom alleviation in CRS.397 Delayed surgery (> 60 months) leads to decreased improvement in long-term SNOT-22 scores regardless of the co-occurrence of co-morbid asthma and/or allergies.398 SNOT-22 is used to categorize CRS into 5 clusters having different outcomes.399
CRSwNP patients show higher recurrence rates than those with CRSsNP.400 A multicenter prospective cohort study demonstrated that the recurrence rates after ESS ranged from 35 to 40% when the follow-up period was prolonged from 6 to 18 months.401 Another study showed that 60% of the patients experienced polyp relapse within a follow-up period of 12 to 168 months.28 In agreement with the results obtained in the US, the postoperative polyp recurrence was found to be greater than 50% in Turkey.402 In the Chinese population, the recurrence rate was 55% when CRSwNP patients were followed after 3 years.403
Clinical factors, such as prior ESS, increased preoperative polyp severity, and eosinophilic density of the NP,28401402 are associated with an increased likelihood of polyp recurrence. Evaluation of the inflammatory cells and cytokine profiles help in the identification of biomarkers that can be used to assess the risk of recurrence.
Biomarkers can be identified from nasal polyp biopsies, nasal secretions, and peripheral blood.404 Lou et al.403 demonstrated that CRSwNP patients with > 27% eosinophils or 55 eosinophils/high power field (HPF) showed recurrence. Two Japanese studies215377 showed that mucosal eosinophilia (> 70 eosinophils/HPF) results in poor prognosis. Mucosal eosinophilia at 120 cells/HPF is strongly correlated with recurrent CRS.405 Similarly, Grgić et al.406 showed that high tissue eosinophil infiltration (> 20/HPF) indicates high risk of recurrence. Thus, tissue eosinophilia provides valuable information regarding NP recurrence after ESS. The degree of tissue eosinophilia can be considered to be an important predictor of NP recurrence.
Blood eosinophilia can be used as a surrogate for tissue eosinophilic inflammation.210405 Studies have shown the prognostic role of blood eosinophil counts and percentages in the recurrence of CRSwNP.377405407 However, various conditions, including allergy, autoimmune diseases, drugs, and parasitic infections, can alter the number of eosinophils in circulation. Thus, blood eosinophilia does not precisely reflect tissue eosinophilia, and its prognostic ability remains limited.403
The diversity of nasal microbiota in nasal secretions can affect surgical outcomes.408 The relative abundance of the phylum Actinobacteria and genus Corynebacterium indicates improved surgical outcomes408 whereas repeated sinus surgery frequently results in Pseudomonas aeruginosa positive bacterial cultures.409 However, the prognostic role of microbiota in ESS requires further study.
Recent immunological advancements may help to distinguish CRS with different recurrence rates. Grgić et al.406 showed that IL-5 levels in the tissue homogenates can be used to predict recurrence. Another study found a heterogeneous, rather than homogeneous, Th pattern in the nonrecurrent CRSwNP.206 Th1, Th2 and Th17 cytokines, along with significantly increased levels of IFN-γ, were produced in most cases of the nonrecurrent CRSwNP whereas the recurrent CRSwNP expressed a predominantly Th2-type inflammation with increased levels of IL-5, ECP, IgE and SE-IgE.206 Therefore, understanding the diversity of the CRS endotypes across the world5 will be useful for predicting the outcomes in different regions.
Targeted treatment with biologics
Improved understanding of the pathophysiological mechanisms of CRS has spurred the development of targeted therapies based on the biomarkers of CRS patients, resulting in endotype-driven treatments.238239 Among these endotypes, the type 2 inflammation-based endotype is well understood, but the non-type 2 inflammation-based, and other endotypes require further studies.
Anti-IgE
Omalizumab, a recombinant, humanized, anti-IgE mAb can bind circulating IgE via its high-affinity receptor (FcεRI) and prevent it from binding to effector cells such as mast cells, basophils, DCs, and eosinophils. Subsequently, the expression of FcεRI on effector cells is reduced. 410 In CRSwNP patients with comorbid asthma, omalizumab can reduce the upper and lower airway symptoms, endoscopic NP scores, and the requirement for other medical or surgical treatments.411412 However, omalizumab exerts scant and clinically irrelevant effects on CRS in which the presence of NPs was not taken into account.413 Until now, only omalizumab has been registered and approved for the treatment of asthma in China. However, other anti-IgE-based treatments are currently being developed; these include ligelizumab, which shows higher affinity for IgE, compared to omalizumab,414 and quilizumab, which targets the M1 epitope on the membrane IgE.415
Anti-IL5
Mepolizumab and reslizumab are humanized anti-IL5 mAbs that can neutralize IL-5. Reslizumab significantly reduces the blood eosinophil counts and nasal IL-5 levels in patients with NP and improves individual NP scores for up to 4 weeks in 50% of patients.416 Mepolizumab reduces NP scores in patients with severe and/or recurrent NPs.205 Reslizumab and mepolizumab are safe and well-tolerated in CRSwNP patients.205416 Benralizumab, another humanized mAb against the highly-expressed IL-5Rα receptor on eosinophils, has been shown to be safe and effective in uncontrolled asthma with eosinophilia in a phase III trial.417
Anti-IL-4/IL-13
IL-4 and -13 share the IL-4Rα subunit, which forms a functional IL-4 receptor, with the common γC subunit, or an IL-4 and -13 receptor, with an IL-13Rα subunit.418 Dupilumab, a fully human mAb against IL-4Rα, can inhibit the effects of IL-4 and -13232 and is used to treat atopic dermatitis and asthma.419420 In a recent phase II trial, Bachert et al.204 evaluated the use of subcutaneously-administered dupilumab in the treatment of the uncontrolled CRSwNP. This therapy was shown to improve endoscopic NP scores, CT scores (obtained using the Lund-Mackay scoring system) and QoL, and reduce major symptoms including loss of smell, nasal obstruction and congestion, and nocturnal awakenings in more than half of the treated patients, compared to the placebo group. This effect was retained for up to 2 months and slowly decreased during the 16 weeks of follow-up after treatment cessation.204
Additional anti-type 2 therapies
New anti-type 2 therapies include a GATA-3 specific DNAzyme, which was evaluated in a phase IIb study for the treatment of allergic asthma.233 So far, these targeted treatments have not been investigated in rhinitis or CRS. Another mAb, AK001, targets siglec-8, a cell surface receptor selectively expressed on mast cells, eosinophils, and basophils. A phase II study is currently evaluating the efficacy of AK001 in CRSwNP patients.421
UNMET NEEDS AND SUMMARY
CRS affects approximately 8% of the adult population in China. The inflammatory and remodeling characteristics of CRS in Chinese patients have shown an eosinophilic shift over time and differ from the characteristics of patients of European descent. The development of precision treatments based on endotype-driven pathways hinges on improving our understanding of the pathophysiologic mechanisms involved in CRS. Traditionally, clinicians differentiate phenotypes of a disease based on its clinical manifestations; however, we now recognize that the inflammatory endotypes of CRS also show considerable variation. Disease recurrence after pharmacotherapy and surgery is associated with a significant Th2 bias and eosinophilic inflammation. CRS endotypes vary by region and environment with respect to genetic factors. China's population is twice as large as that of Europe, and numerous distinct CRS endotypes exist within the Chinese population. Conducting multi-center studies nationwide is necessary to define the CRS endotypes and develop precision therapies for the Chinese population.
The therapeutic approaches summarized in the current guidelines do not achieve long-term symptom control. Pharmacotherapy and surgery demonstrate limited effects with respect to controlling severe CRSwNP, which shows frequent recurrence and asthma comorbidity. Verification of the CRS endotypes and mapping of the eosinophilic shift will provide new targets for interventions. Future studies would identify biomarkers that will be suitable for endotyping and predicting therapeutic responses. The development of biotherapeutics in China currently trails that of Western countries by nearly 2 decades, highlighting the pressing need for the development of these drug types. Dosages and treatments for the endotypes specific to the Chinese patients will also require further studies. In summary, therapies, including pharmacotherapies, surgical approaches, and biotherapeutics, should be tailored to the individual CRS endotypes.
 XML Download
XML Download