

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Statins, which are 3-hydroxy-3-methyl-glutaryl-CoA (HMG-CoA) reductase inhibitors, have revolutionized today's cardiovascular management, as they markedly decrease blood cholesterol levels and effectively prevent atherosclerotic cardiovascular disease (CVD). Multiple large-scale clinical trials have confirmed that statin-induced reduction of low-density lipoprotein cholesterol (LDL-C) has a log-linear relationship with CVD prevention effects, where a 1 mM (38.7 mg/dL) reduction of LDL-C lowers the incidence of cardiovascular events by 22%.1 Atorvastatin has a longer plasma half-life than other statins and is an effective inhibitor of HMG-CoA reductase, thereby substantially lowering blood cholesterol levels.2 Furthermore, owing to its tolerability, efficacy, safety, and CVD preventative effects, it is currently one of the most widely used statins.345678
Reduction of LDL-C as a result of statin administration is proportional to the pre-administration concentration, so percentage reduction, as opposed to absolute reductions (mmol/L), is utilized as an indicator of statin efficacy.9 Intensity of statin therapy is divided into 3 efficacy categories: high-intensity that reduces LDL-C by more than 50%, moderate-intensity that reduces LDL-C by 49%–30%, and low-intensity that reduces LDL-C by less than 30%. The American Heart Association/American College of Cardiology (AHA/ACC) guidelines recommend high-intensity or moderate-intensity statin for patients with diabetes mellitus or intermediate-to-high risk.1011 However, even low-dose statin therapy is known to significantly lower LDL-C in Asians, including Koreans,1213141516 and some guidelines suggest administration of low-dose statin to Asians.1718
In general, women have low CVD risk, but as they reach menopause, when their blood estrogen levels decrease, their blood total cholesterol (TC) and LDL-C levels gradually increase, and postmenopausal women even have higher LDL-C levels than their male counterparts. Moreover, high-density lipoprotein cholesterol (HDL-C) concentration also slightly declines after menopause.1920 In addition to such changes in the blood lipid profile, the incidence of coronary artery disease (CAD) is about 2–3 times higher after menopause.2122 Therefore, treating dyslipidemia is critical for postmenopausal women with CVD or high cardiovascular risk. However, the main participants of past large-scale clinical trials on statins were men.23 Hence, more clinical trial data on the use of statin among postmenopausal women is needed.
Therefore, we have designed a prospective multicenter clinical trial to investigate the changes of blood lipid profile and adverse reactions of moderate-to-high intensity atorvastatin in postmenopausal Korean women at risk of CVD.
MATERIALS AND METHODS
1. Study subjects
Postmenopausal women aged 45 years or older, who had moderate-to-high CVD risk and whose blood LDL-C levels were higher than the target levels set by the second edition of the Korean Society of Lipid & Atherosclerosis (KSoLA) guidelines,24 were enrolled. Menopause was defined as bilateral oophorectomy, or at least 2 months of amenorrhea in an interval of 60 or more days in the past 12 months, or hysterectomy with follicle-stimulating hormone ≥40 IU/L and estradiol <50 pg/mL. CVD risk was classified based on the second edition of the KSoLA guideline, where individuals with 2 or more major risk factors excluding LDL-C was classified as the moderate-risk group and individuals with CAD, carotid artery disease, peripheral vascular disease, abdominal aneurysm, or diabetes mellitus as the high-risk group. LDL-C target was below 130 mg/dL and 100 mg/dL for the moderate-risk and high-risk groups, respectively.24
Exclusion criteria included the following: history of acute myocardial infarction or congestive heart failure within 3 months prior to clinical trial participation, body mass index (BMI) <18.5 or >30 kg/m2, liver enzyme level 2-fold higher than the normal upper limit, creatine kinase level 2-fold higher than the normal upper limit (excluding cases due to trauma, intramuscular injection, and excessive exercise), creatinine levels >2.5 mg/dL, fasting triglyceride (TG) levels ≥400 mg/dL, hemoglobin A1c (HbA1c) ≥11%, or fasting glucose ≥200 mg/dL, risk factors of rhabdomyolysis, and if undergoing hormone replacement therapy, use of another hyperlipidemia medication within 4 weeks of the study drug administration; or inability to participate in clinical trial as determined by the investigator.
2. Study design
This study is a 16-week prospective, open-label, single-arm clinical trial conducted at 3 teaching hospitals in Korea. This clinical trial was approved by the Institutional Review Board (IRB No. JEJUNUH 2010-32) at each hospital. Written informed consent was obtained from all participants, and we adhered to the Declaration of Helsinki. This clinical trial was conducted at Cheil General Hospital and Eulji Hospital in Seoul and Jeju National University Hospital from November 2010 to December 2011.
Eligible participants, postmenopausal women with a moderate-to-high cardiovascular risk, were administered atorvastatin for a total of 16 weeks. First, atorvastatin (20 mg) was administered daily for the first 8 weeks. If the LDL-C levels measured after 8 weeks reached the target, the same dose was continued for another 8 weeks. If the target was not achieved, the dose was increased to 40 mg for another 8 weeks. LDL-C target was set to <130 mg/dL for the moderate-risk group and <100 mg/dL for the high-risk group, per KSoLA guidelines.24 Use of any drugs that may impact the results was prohibited during the study period.
3. Study assessments
Participants' demographics and disease history were taken at the baseline visit, and drug history, anthropometric parameters, study drug adherence, vital signs, abnormal symptoms, and adverse reactions were assessed at the baseline visit and weeks 8 and 16 of drug administration. Aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, creatine kinase, total bilirubin, fasting glucose, HbA1c, high sensitivity C-reactive protein (hsCRP), TC, TG, HDL-C, LDL-C, apolipoprotein B (apoB), and apolipoprotein A1 (apoAI) were measured at the baseline visit and at weeks 8 and 16 of drug administration. These lab tests were conducted on blood samples taken after at least 12 hours of fasting, at each institution. LDL-C was measured directly without using an equation for calculation.
The primary endpoint was percentage change of LDL-C from baseline after 16 weeks of atorvastatin administration. The secondary endpoints were percentage changes of TC, TG, HDL-C, apoB, apoAI, and hsCRP.
4. Statistical analyses
This clinical trial was a pilot study, with a target sample size of 45 (15 from each institution) without statistical computation.
Efficacy analysis was performed on full analysis (FA) and per protocol (PP) sets, and analysis of baseline characteristics and safety were performed on a safety set. The FA set consisted of participants who met the inclusion/exclusion criteria, and had taken at least one dose of the study drug after prescription and underwent at least one efficacy assessment. In the PP set, the following cases were excluded from the FA set: violation of inclusion/exclusion criteria, use of prohibited drug during the study period, omission of tests for efficacy parameters, medication adherence <80%. The safety set consisted of participants who have taken at least one dose of the study drug and underwent at least one safety-related interview.
Statistical significance on the changes of efficacy parameters after study drug administration was analyzed with paired t-test (parametric test) or Wilcoxon's signed-rank test (non-parametric test).
RESULTS
1. Patient disposition
A total of 58 participants were selected, 44 of whom provided written consent to participate. However, 7 were excluded per the inclusion/exclusion criteria, so 37 participants were administered the study drug (safety set). Of them, 35 participants, after excluding 2 participants with omitted efficacy parameters since study drug administration, were included in the FA set; and 31 of these participants, after excluding 4 participants with a medication adherence of below 80% or omitted baseline efficacy parameters, were included in the PP set (Fig. 1).

2. Baseline characteristics
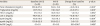
All participants were postmenopausal women, and the cause of menopause was natural for the majority of participants. The mean BMI was 25.3 and the mean waist circumference was 84.7 cm. A total of 75.6% of the participants had diabetes mellitus, a condition for the high CVD risk group. The highest percentage of participants had 2 of 5 major CVD risk factors (51.3%), followed by participants with one major risk factor (21.6%), participants with no risk factor (24.3%), and participants with 3 risk factors (2.7%; Table 1).
Table 1
Clinical and laboratory characteristics of the study subjects (safety set)

Data are expressed as mean±standard deviation or frequencies (%).
BP, blood pressure; CAD, coronary artery disease; HDL-C, high-density lipoprotein cholesterol.
*1) Smoking, 2) Hypertension (BP ≥140/90 mmHg or antihypertensive medication), 3) Low HDL-C (<40 mg/dL), 4) Family history of premature CAD, and 5) Age (male ≥45, female ≥55 years); High HDL-C (≥60 mg/dL) is considered as a protective factor, and one factor is excluded from the total number of risk factors.
![]()
3. Efficacy analysis
After 8 weeks of atorvastatin (20 mg), 33 (94.2%) participants reached the LDL-C target, and these participants maintained the same daily dose for the following 8 weeks. Two participants who did not reach the LDL-C target after the first 8 weeks took an increased dose (40 mg) in the second 8 weeks, after which they reached the LDL-C target. In the end, all participants achieved the LDL-C target after 16 weeks of atorvastatin administration (Table 2).
Table 2
Percentage of subjects who reached the low-density lipoprotein cholesterol goals* at 8 and 16 weeks of treatment (full analysis set)

| Duration (wk) | Treatment (n=35) |
|---|---|
| 8 | 33 (94.2) |
| 16 | 35 (100.0) |
Value are given as a number (%).
*Subjects with diabetes <100 mg/dL, subjects with 2 or more major risk factors <130 mg/dL.
![]()
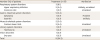
In the FA set, the percent change of LDL-C from baseline after 16 weeks of atorvastatin administration, the primary endpoint of this study, was −45.8%, showing a statistically significant reduction of LDL-C (p<0.001). TC, TG, and apoB were also significantly reduced by 33.2%, 24.2%, and 34.9%, respectively. However, HDL-C, apoAI, and hsCRP were not significantly changed (Table 3). The results of analyses on the PP set were similar to that of the FA set (Supplementary Table 1).
Table 3
Changes in efficacy measures from baseline to week 16 (full analysis set)
Data are shown as mean±standard deviation.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; apoB, apolipoprotein B; apoAI, apolipoprotein AI; hsCRP, high sensitivity C-reactive protein.
*Paired t-test; †Wilcoxon's signed-rank test.
![]()
4. Safety analysis
After 16 weeks of atorvastatin administration, the mean fasting blood glucose was elevated by 9.5 mg/dL, with no significant changes in HbA1c. Creatinine, total bilirubin, and creatine kinase were not significantly changed. AST and ALT increased by 2.2 and 4.2 U/L, respectively, but no participants had more than 3-fold increase from the normal upper limit (Table 4). Among the 37 participants who received atorvastatin administration, a total of 9 participants had abnormal symptoms: respiratory (n=3), digestive (n=2), musculoskeletal (n=2), urological (n=2), or eye (n=1). Both musculoskeletal symptoms were fractures, and none of the participants complained of myalgia. Most of these abnormal symptoms were not related to atorvastatin, and only one case of mild indigestion was determined to be possibly related (Table 5). None of the participants were prematurely withdrawn from the clinical trial for adverse reactions or abnormal symptoms.
Table 4
Summary of adverse events reported during the treatment period (safety set)
![]()
Table 5
Changes in clinical laboratory parameters from baseline to week 16 (full analysis set)

Data are expressed as mean±standard deviation.
*Paired t-test; †Wilcoxon's signed-rank test.
HbA1c, hemoglobin A1c; CI, confidence interval; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
![]()
DISCUSSION
According to the AHA/ACC guideline,10 the dosages of atorvastatin (20 or 40 mg) used in our study are those recommended for moderate- and high-intensity statin therapies, respectively, which were presumed to reduce LDL-C by 30–49 and >50%, respectively. Most of our participants were administered a moderate-intensity dosage (20 mg) for 16 weeks, and only 2 participants (5.8%) received an elevated dose (40 mg) during the second 8 weeks. Most previous clinical trials of atorvastatin in Koreans14252627 used a 10 mg dose, which reduced LDL-C levels by 33.3%–41.8%. In the present study, where most participants were administered 20 mg, LDL-C was reduced by 45.8%, suggesting that atorvastatin reduces LDL-C dose-dependently in Koreans, and a daily dose of 20 mg is more effective than 10 mg.
TC, TG, and apopB, the secondary endpoints of this clinical trial, decreased by 33.2%, 24.2%, and 34.9%, respectively, which are not markedly different from those of other atorvastatin studies.28 However, in the present study, HDL-C and apoAI did not significantly change (−1.2% and 0.0%, respectively) which differs from the significant elevation of HDL-C commonly observed in general statin studies. Although the exact reason is unknown, we speculate that changes of HDL-C caused by statin may vary according to the drug ingredients and patient's race. The majority of atorvastatin studies in Koreans1314252629 support this hypothesis, as they found that HDL-C tended to decrease after drug administration. High sensitivity CRP, another secondary endpoint, did not significantly change in our study, presumably because participants' baseline hsCRP levels were low. Exclusion of participants with recent diagnosis of CVD is likely the cause of low baseline hsCRP. In fact, the mean baseline hsCRP in participants of the JUPITER trial, a study that objectively proved the effects of statins for reducing hsCRP and CVD risk, was 4.3 mg/L, which is over 3-fold higher than that of our study.30
Statins are known to increase blood glucose and diabetes mellitus risk.3132 In the present study, fasting blood glucose was significantly elevated after 16 weeks of atorvastatin. However, the mean elevation of blood glucose was not large, at 9.5 mg/dL, and there were no significant changes in HbA1c. According to the UK Prospective Diabetes Study,33 a 1% reduction of HbA1c leads to 14% reduction of CAD, and according to the meta-analysis by Baigent et al.,1 a 38.7 mg/dL reduction of LDL-C can lower CAD by 22%. Therefore, the cardiovascular benefit of 45.8% reduction of LDL-C (77.1 mg/dL) in this study far outweighs the harm from a 9.5 mg/dL elevation of fasting blood glucose. However, the impact of high-dose statins on glycemic control or new-onset diabetes cannot be neglected, and large-scale, long-term clinical trials are required to substantiate this further. In the present study, liver enzyme levels were mildly elevated after atorvastatin administration. However, meaningful elevation of liver enzymes by statins is defined as greater than 3-fold increase from the upper normal limit,34 which did not occur in the present study. Statin-induced myalgia is a highly common side effect, with an incidence of about 5%–20%, but no participants complained of myalgia. However, this may be a result of the small sample size or neglect of the mild symptoms. The only abnormal symptom related to the atorvastatin in this study was indigestion, which was observed in one participant, and such gastrointestinal disturbance has been identified as the most common adverse reaction of atorvastatin by multiple clinical trials.35
This study has quite a few limitations. First, there was no control group. Therefore, we cannot eliminate the possibility that a change of lifestyle during the study period may have led to the improvements of blood lipid levels. Secondly, only 2 participants (5.8%) were given 40 mg of atorvastatin. As the vast majority of participants (94.2%) were given a daily dose of 20 mg, we cannot assess the efficacy and safety of high-intensity therapy (40 mg atorvastatin). Thirdly, the sample size was small, niche, and not properly calculated. To efficiently proceed with the clinical trial, we planned to recruit 45 participants. One of the reasons behind the absence of significant changes in HDL-C and hsCRP in the present study may the small sample size. This study was only conducted on postmenopausal women, so it may be inappropriate to generalize the findings of this clinical trial to all patients with dyslipidemia in Korea. As this was a pilot study and there was no preliminary study data, sample size could not be calculated using an appropriate statistical technique. In addition, we did not use a low-dose atorvastatin group. This study only involved a single atorvastatin group (20/40 mg), therefore, we cannot definitively conclude that high-dose atorvastatin administration is more effective than or equally safe as 10 mg of atorvastatin. Lastly, the incidence of CVD was not measured. A clinical trial that overcomes the above shortcomings is needed to objectively assess the effects, safety, and CVD preventative effects of high-dose atorvastatin in Koreans.
In the present study, 16 weeks of atorvastatin (20 or 40 mg) lowered LDL-C, the primary endpoint, by an average of 45.8% from baseline, and all participants (Korean postmenopausal women with moderate-to-high cardiovascular risk) reached the LDL-C target. TC, TG, and apoB were significantly reduced from baseline by 33.2%, 24.2%, and 34.9%, respectively, and abnormal symptoms or adverse reactions were not observed. To the best of our knowledge, this study is the first prospective clinical trial assessing the efficacy and safety of atorvastatin in postmenopausal Korean women. Based on the findings of this study, we can conclude that moderate- or high-intensity atorvastatin therapy safely and markedly improves blood lipid profiles of postmenopausal Korean women, and we can predict that it will suppress the onset of CVD related to dyslipidemia.
 XML Download
XML Download