

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of atherosclerotic cardiovascular disease (ASCVD) increases progressively with age.1 Individuals more than 75 years of age are more than 3 times as susceptible to cardiovascular mortality than younger age groups. Thus, primary prevention in this group is critical.23 However, most randomized trials have excluded older patients, resulting in insufficient clinical evidence for primary cardiovascular prevention in this population.45
We recently analyzed the effect of statins on clinical outcomes for primary prevention in patients aged >75 years. Here, we present the major results of that study and review other recent studies on the same topic, with a focus on the effects of statins for primary prevention in the elderly.
CURRENT STATIN GUIDELINES AND KNOWLEDGE GAPS REGARDING THE ELDERLY POPULATION
The 2018 American College of Cardiology/American Heart Association (ACC/AHA) and the 2019 European Society of Cardiology/European Atherosclerosis Society (ESC/EAS) guidelines were recently released.67 In Korea, the latest guideline for the management of dyslipidemia was released in 2019.8 However, these guidelines contain gaps regarding statin use in the elderly population; these gaps derive from concerns regarding frailty, multimorbidity, polypharmacy, and functional limitations in the elderly.9 Furthermore, each of these guidelines uses a different age threshold (Table 1). The recently published ESC/EAS guideline extended the age of the risk assessment system from 65 to 70, and recommended statin use for primary prevention according to individuals' level of risk until age 75.7 With this in mind, we have defined “elderly” as referring to individuals aged over 75 herein. We reviewed previous randomized controlled trials (RCTs), meta-analyses, and studies on statin therapy for primary statin prevention published since 2018.
Table 1
Comments on elderly patients in the latest guidelines

| Guideline | ESC/EAS 20197 | ACC/AHA 20186 | Korea 20188 |
|---|---|---|---|
| Age (yr) | 40–75 | 40–75 | 30–65 |
| Risk assessment | SCORE (40 to 70 yr) | Pooled cohort equation (≤79 yr) | No. of risk factors |
| Risk threshold for therapy | • High risk: 5% to 10% | • High risk: ≥20% | • Very high risk: coronary artery disease, atherosclerotic ischemic stroke and transient ischemic attack, peripheral artery disease |
| • Very high risk: ≥10% | • Intermediate risk: 7.5% to 20% | • High risk: carotid artery disease, abdominal aneurysm, diabetes | |
| • Intermediate: ≥2 RFs | |||
| • Low: ≤1 RF | |||
| Threshold for starting statin use | • Very high: 70 mg/dL | • ≥190 mg/dL | • Very high: ≥70 mg/dL |
| • High: 100 mg/dL | • Adults with diabetes | • High: ≥100 mg/dL | |
| • Intermediate: ≥130 mg/dL | |||
| • Low: ≥160 mg/dL | |||
| Target | • Very high: <55 mg/dL | • High: 50% or more decrease | • Very high: <70 mg/dL |
| • High: <70 mg/dL | • Intermediate: 30% decrease | • High: <100 mg/dL | |
| • Intermediate or low: <115 mg/dL | • Intermediate: <130 mg/dL | ||
| • Low: <160 mg/dL | |||
| Comment for elderly | • 65 to <75 yr: according to level of risk | • Not strong evidence for patients aged >75 yr | • The primary preventive effects of statins on older adults aged ≥70 yr have been proven |
| • >75 yr: at high risk or above, initiation of statin prevention | • Moderate-intensity statin use for patients aged >75 yr with 70 to 189 mg/dL may be reasonable | • ≥80 yr: evidence is lacking | |
| • Statin therapy should be started at a low dose if there is significant renal impairment and/or the potential for drug interactions, and then titrated upwards to achieve LDL-C treatment goals | • Statins should be used while carefully monitoring their interactions with other drugs and adverse reactions |
STATINS AND CLINICAL OUTCOMES OF PRIMARY PREVENTION IN INDIVIDUALS AGED >75 YEARS: THE SCOPE-75 STUDY
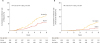
We recently conducted the SCOPE-75 study, which included patients aged >75 years who had at least 1 cardiovascular risk factor.10 In this retrospective, propensity score-matched study, we analyzed 639 statin users and 639 statin non-users. At a median follow-up of 5.2 years, statin users showed lower rates of major adverse cardiovascular and cerebrovascular events (1.25 vs 2.15 events/100 person-years; hazard ratio [HR], 0.59; 95% confidence interval [CI], 0.40–0.85; p=0.005) and all-cause mortality (0.65 vs. 1.19 events/100 person-years; HR, 0.56; 95% CI, 0.34–0.93; p=0.02). The HRs were the same for each outcome variable in Kaplan-Meier curves (Fig. 1). In this study, statin use was associated with a minimal increase of new-onset diabetes, but showed no association with new-onset cancers. This study shed light on the controversial issue of statin use for primary prevention in the elderly by providing evidence of an association between statin use and cardiovascular risk reduction in people aged >75 years.
Fig. 1
Incidence of MACCE and all-cause mortality in the SCOPE-75 study (from Kim et al.10 with permission).
MACCE, major adverse cardiac and cerebrovascular events; HR, hazard ratio.
PRIOR STUDIES PERFORMED IN MIXED POPULATIONS
Several clinical trials have provided evidence that statin use is beneficial for primary prevention in patients aged >75 years11 Patients in this age range were included in trials such as Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese (MEGA)12 and Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) (Table 2).1314 The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial-Lipid Lowering Trial (ALLHAT-LLT)1516 and PROspective Study of Pravastatin in the Elderly at Risk (PROSPER)17 trials enrolled patients aged 65–82. However, these studies contained mixed populations for primary and secondary prevention. These RCTs showed significant cardiovascular risk reduction in statin users, and the results were consistent in patients aged 66–75 years. Furthermore, 2 meta-analyses by Savarese et al.18 and Ridker et al.19 showed benefits of statin use for primary prevention in patients aged >65 years. Savarese et al.18 analyzed patients aged ≥65 years in 8 clinical trials and showed a relative risk reduction of 39.4% for myocardial infarction and 23.8% for stroke. Although the risk of all-cause and cardiovascular death was also reduced, that reduction was not statistically significant. The study by Ridker et al. 19 included the JUPITER and Heart Outcomes Prevention Evaluation-3 (HOPE-3) trials and analyzed 3 age groups: <65 years, 65 to <70 years, and ≥70 years. In all groups, statin therapy reduced cardiovascular risk (Table 2). A meta-analysis by the Cholesterol Treatment Trialists' Collaboration20 analyzed 186,864 patients from 28 clinical trials, of whom 14,483 (8%) were older than 75 years. In that study, statin therapy reduced major vascular events by 21% per 1.0 mmol/L decrease in low-density lipoprotein cholesterol. In the subgroup of elderly individuals (>75 years of age), statins were also associated with fewer vascular events (relative ratio [RR], 0.79; 95% CI, 0.77–0.81). However, for primary prevention in patients aged >75 years, the risk reduction was not significant (RR, 0.92; 95% CI, 0.73–1.16).20
Table 2
Prior studies on statin use for primary prevention that included mixed populations

| Study | Study design | No. of patients | Mean age (or range) (yr) | Outcome variables | Findings (95% CI) | |||
|---|---|---|---|---|---|---|---|---|
| RCTs | ||||||||
| ALLHAT-LLT15 | • Secondary analysis of RCT; usual care vs. pravastatin (40 mg) | • 10,355 | • 66 (>65: 55%) | • All-cause mortality | • Death: RR, 0.99 (0.89–1.11) | |||
| • Primary and secondary prevention | • CHD events | • CHD: RR, 0.91 (0.79–1.04) | ||||||
| PROSPER17 | • RCT; placebo vs. pravastatin (40 mg) | • 5,804 | • 75 (range 70–82) | • Composite (CHD death, nonfatal MI, fatal or nonfatal stroke) | • 16.2% vs. 14.1% | |||
| • Primary and secondary prevention | • 3,239 (primary prevention) | • HR, 0.85 (0.74–0.97) | ||||||
| • Primary prevention: no interaction | ||||||||
| MEGA12 | • RCT; diet vs. pravastatin (10–20 mg) | • 3,966 | • 58 (>65: 23%) | • CHD | • 5.0% vs. 3.3% | |||
| • Primary prevention | • HR, 0.67 (0.49–0.91) | |||||||
| • ≥60 yr: HR, 0.59 (0.40–0.88) | ||||||||
| JUPITER13 | • RCT; placebo vs. rosuvastatin (20 mg) | • 17,802 | • 66 (>65: 58%, ≥70: 32%)* | • Composite (MI, stroke, arterial revascularization, hospitalization for unstable angina, or CV death) | • 1.36%/yr vs. 0.77%/yr | |||
| • Primary prevention | • 5,695 (>70 yr) | • HR, 0.56 (0.46–0.69) | ||||||
| • >65 yr: no interaction | ||||||||
| • ≥70 yr: HR, 0.61 (0.46–0.82)† | ||||||||
| Meta-analyses | ||||||||
| Savarese et al.18 | • Meta-analysis of 8 trials; | • 24,674 (only age ≥65 yr) | • 73 | • MI, stroke, all-cause death, and CV death | • MI: RR, 0.606 (0.434–0.847) | |||
| - Lovastatin | • Stroke: RR, 0.762 (0.626–0.926) | |||||||
| - Pravastatin | • Death: RR, 0.941 (0.856–1.035) | |||||||
| - Atorvastatin | • CV death: RR, 0.907 (0.66–1.199) | |||||||
| - Fluvastatin | ||||||||
| - Rosuvastatin vs. placebo | ||||||||
| • Primary prevention | ||||||||
| Ridker et al.19 | • Meta-analysis of 2 trials | • 8,208 (65 to 70 yr) | • Composite (CV death, nonfatal MI, or nonfatal stroke) | • 65 to 70 yr: HR, 0.51 (0.38–0.69) | ||||
| - JUPITER, HOPE-3 | • 8,781 (≥70 yr) | • ≥70 yr: HR, 0.74 (0.61–0.91) | ||||||
| - Placebo vs. rosuvastatin (10–20 mg) | ||||||||
| CTT20 | • Meta-analysis of 28 RCTs; controls vs. statin | • 186,854 | • 78.8 (>75 yr) | • Composites (major coronary events, strokes, coronary revascularizations) | • 3.7% vs. 3.0%: RR, 0.79 (0.77–0.81) | |||
| • Primary and secondary prevention | • 14,483 (>75 yr) | - >75 yr: RR, 0.87 (0.77–0.99) | ||||||
| • Secondary: RR, 0.80 (0.77–0.82) | ||||||||
| - >75 yr: RR, 0.85 (0.73–0.98) | ||||||||
| • Primary: RR, 0.92 (0.71–0.80) | ||||||||
| - >75 yr: RR, 0.92 (0.73–1.16) | ||||||||
| - Per 1 mmol/L reduction in LDL-C | ||||||||
CHD, coronary heart disease; CI, confidence interval; CTT, Cholesterol Treatment Trialists' Collaboration; CV, cardiovascular; HR, hazard ratio; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction; RCT, randomized controlled trial; RR, relative ratio; JUPITER, Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin; MEGA, Management of Elevated Cholesterol in the Primary Prevention Group of Adult Japanese; PROSPER, PROspective Study of Pravastatin in the Elderly at Risk; ALLHAT-LLT, Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial-Lipid Lowering Trial.
STUDIES IN 2018 AND 2019 FOCUSING ONLY ON THE ELDERLY
Four retrospective studies—including ours—that analyzed the effects of statins for primary prevention in the elderly were published in 2018 and 2019 (Table 3).21 Ramos et al.22 analyzed 46,864 patients older than 74 with or without diabetes. In their study, statin users with diabetes showed significantly reduced risks of ASCVD (HR, 0.76; 95% CI, 0.65–0.89) and all-cause death (HR, 0.84; 95% CI, 0.75–0.94). However, statin treatment was not associated with a reduced risk of ASCVD (HR, 0.94; 95% CI, 0.86–1.04) or all-cause mortality (HR, 0.98; 95% CI, 0.91–1.05) in participants without diabetes. Their study also included 8,307 patients aged >85 years, but statins did not show a significant benefit in this subgroup. Bezin et al.23 reported that cumulative statin use for primary prevention was associated with a lower risk of acute coronary syndrome (adjusted HR, 0.93; 95% CI, 0.89–0.96) in patients aged 75 years or older who had modifiable risk factors. However, the benefits of statins were diminished in patients without risk factors (adjusted HR, 1.01; 95% CI, 0.86–1.18). Jun et al.24 conducted a nested case-control study using a Korean nationwide cohort, focusing on the elderly aged ≥75 years. That study showed that concurrent statin treatment reduced cardiovascular composite outcomes (adjusted odds ratio, 0.77; 95% CI, 0.71–0.84). However, former use of statins had no effect on cardiovascular outcomes or all-cause death. Their study also showed that a longer duration of statin exposure was associated with fewer cardiovascular events.24 As mentioned above, the SCOPE-75 study by us showed significantly lower cardiovascular risk and all-cause mortality in statin users.10 Collectively, these studies provide stronger evidence than was available before for the effects of statins on clinical outcomes. However, the lack of RCTs poses some limitations. The STAtins for Reducing Events in the Elderly (STAREE) trial, which is in progress, aims to determine the efficacy and safety of statins in elderly people aged ≥70 years.25 If properly finished, this trial might be able to provide more comprehensive information regarding the benefits and risks of statin use in the elderly population.
Table 3
Studies published in 2018–2019 analyzing the effects of statin use for primary prevention in the elderly

| Study | Study design | No. of patients | Mean age (or range) (yr) | Outcome variables | Findings (95% CI) |
|---|---|---|---|---|---|
| Ramos et al.22 | • Retrospective cohort study; statin non-users vs. statin users | • 46,864 | • Only ≥75 (>85: 18%) | • ASCVD | • ASCVD (non-diabetes, 75–84 years): RR, 1.00 (0.80–1.24) |
| • 8,307 (≥85 yr) | • ASCVD (diabetes, 75–84 years): RR, 0.76 (0.65–0.89) | ||||
| • ≥85 yr: non-significant | |||||
| Bezin et al.23 | • Retrospective cohort study; statin non-users vs. statin users | • 7,284 (≥75 yr) | • 80 (77–84) | • Composite (acute coronary syndrome, all-cause death) | • Secondary: adjusted HR, 0.75 (0.63–0.90) |
| • Primary and secondary prevention | • Primary with modifiable risk factor: adjusted HR, 0.93 (0.89–0.96) | ||||
| • Primary without modifiable risk factor: adjusted HR, 1.01 (0.86–1.18) | |||||
| Jun et al.24 | • Retrospective case-control study; case vs. control subjects | • 66,102 (≥75 yr) | • 84 | • Composite (MI, stroke, all-cause death) | • Adjusted OR, 0.77 (0.71–0.84) |
| • Primary prevention | |||||
| Kim et al.10 | • Retrospective cohort study; statin non-users vs. statin users | • 1,278 (≥75 yr) | • 78 (≥80: 30%) | • Composite (CV death, MI, coronary revascularization, stroke) | • 2.15%/yr vs. 1.25%/yr |
| • HR, 0.59 (0.41–0.85) |
STATIN USE IN PATIENTS AGED OVER 85 YEARS
To date, data on statin use in patients aged over 85 years remain extremely limited. No risk scoring systems in current guidelines include this population. In the ESC/EAS and ACC/AHA guidelines, statin use for primary prevention in patients aged ≥85 is recommended, but at a weaker level.910 The National Institute for Health and Care Excellence (NICE)-UK guideline suggests that atorvastatin (20 mg) might be beneficial in this age group.26 Only the study by Ramos et al.25 separately analyzed individuals 85 years of age or older separately, and statins showed no benefits in this subgroup.
CONCLUSIONS
Studies performed in the past decade regarding the effects of statin use for primary prevention in individuals aged >75 years have shown possible clinical benefits. The SCOPE-75 study by us and other very recent studies similarly revealed favorable clinical outcomes of statin use in this population. However, a further net-benefit analysis or a study of prospective data would strengthen the evidence base regarding this issue.
 XML Download
XML Download