

 PDF
PDF ePub
ePub Citation
Citation Print
Print



HIGHLIGHTS
• Patient survival in the reoperation group was significantly lower than that in the non-reoperation group.
• Patient with gastrointestinal (GI)-tract releted complications requiring reoperation had lower survival rates than patients with non-GI related complications requiring reoperation.
• Prolonged hospitalization days, operation time and a history of previous hepatocellular carcinoma related operation were significant risk factors for reoperation after living-donor liver transplantation.
INTRODUCTION
Living-donor liver transplantation (LDLT) is a widely-accepted treatment option for patients with end-stage liver disease [12]. The shortage of cadaveric donors and the high number of liver transplantations required have increased the prevalence of LDLT. LDLT is especially prevalent in Asian countries for several reasons—including religious beliefs, cultural traditions, and politics [3]. LDLT is a complicated surgery that requires skilled and well-trained surgeons. However, despite improvements in surgical techniques and postoperative management practices, the rate of postoperative complications in LDLT remains substantial.
The diverse postoperative complications following LDLT depend on various factors including the features of the selected liver graft, the major surgical intervention implemented, accompanying problems in the recipient, and the adverse effects of immunosuppressive treatment. Among these, early complications include primary non-function (PNF), acute rejection, infection, vascular complications, and biliary complications [4]. Certain types of postoperative complications require prompt surgical intervention to save both the patient and the graft. Furthermore, patients who require reoperation are more likely to develop additional complications and, in general, have increased morbidity and mortality [256]. Several recent studies have reported that reoperation rates are higher among LDLT patients than among deceased-donor liver transplantation (DDLT) cases [789]. Therefore, for complications requiring reoperation in LDLT patients, appropriate decision-making and treatment plans remain important and time-sensitive issues. In this study, we analyzed the causes, risk factors, and outcomes in patients requiring reoperation within 30 days of adult-to-adult LDLT. In addition, we classified the causes of reoperation by level of risk.
METHODS
Study Design and Population
Patient data were prospectively collected from the electronic medical records of the Samsung Medical Center (SMC; Seoul, Korea). A total of 577 LDLTs were performed between January 2010 and December 2016 at SMC, of which 66 pediatric patients and five cases of retransplantation were excluded from this study. In total, 506 adult-to-adult LDLT recipients were retrospectively analyzed. The following characteristics were reviewed for the chosen patients: sex, age, body mass index (BMI), Child-Pugh classification, the model for end-stage liver disease (MELD) score, length of hospital stay, length of postoperative intensive care unit stay, and requirement for intraoperative transfusion. A history of previous operations was collected, including abdominal operations involving intraperitoneal operations, and hepatocellular carcinoma (HCC)-related operations involving liver resection due to HCC (both open and laparoscopic operative techniques). Early reoperation was defined as any surgical intervention within 30 days after LDLT. All operations were performed after obtaining informed consent from the patients and approval by the Ethical Committee and Institutional Review Board of SMC (IRB No. 2019-09-009-001).
Statistical Methods
Baseline characteristics were analyzed using Pearson's chi-square test for categorical variables and the Wilcoxon rank sum test for continuous variables. The association of potential risk factors with reoperation was tested using a logistic regression analysis. Variables with P<0.05 in a univariate analysis were included in the multivariate logistic regression. For rare events, a logistic regression model using Firth's penalized maximum likelihood estimation was applied. A stepwise selection method was used to identify co-variables in the logistic regression model. Patient survival rates were estimated using Kaplan-Meier survival curves, and a log-rank test was used to determine significant differences (P<0.05) between cohorts. All data handling and analyses were performed using the SAS ver. 9.4 (SAS Institute Inc., Cary, NC, USA) and supported by the Biostatistics & Clinical Epidemiology Center in SMC. The P-values <0.05 were considered statistically significant.
RESULTS
Baseline Characteristics of the Recipients
The baseline characteristics of adult LDLT recipients are shown in Table 1. Among 506 patients, 98 underwent reoperation (19.4%). The mean age, sex, BMI, past medical history, and conditions associated with liver disease were not significantly different between the reoperation and non-reoperation groups. However, the reoperation group had significantly higher mean operation time during liver transplantation, length of hospitalization (days), and history of previous HCC-related operations compared to the non-reoperation group.
Overall Survival Rate
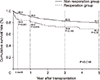
Patient survival rates after 3 months, 1 year, 3 years, and 5 years after LDLT were 95.9%, 82.6%, 72.8%, and 69.3% in patients who underwent reoperation and 96.3%, 90.6%, 82.5%, and 79.4% in patients who did not undergo reoperation, respectively (P=0.018). The 3-month and 1-year survival rates (i.e., early survival after LDLT) were significantly lower in the reoperation group (P< 0.001, P=0.016, respectively). The 3-year and 5-year survival rates were also lower in the reoperation group, but the differences were not statistically significant (P=0.153, P=0.28, respectively) (Fig. 1).
The causes for reoperation were divided into subgroups as follows: bleeding (n=39, 39.8%), vascular complications (n=26, 26.5%), wound complications (n=12, 12.2%), bile leakage (n=7, 7.1%), gastrointestinal (GI) complications (n=6, 6.1%), and others (n=8, 8.1%). The survival rates based on cause for reoperation are shown in Fig. 2. At the 3-year follow-up, the patient survival rates were 79.5% for bleeding, 73.1% for vascular complications, 91.7% for wound complications, 28.6% for bile leakage, 33.3% for GI complications, and 87.5% for other causes of reoperation.
To clarify outcome severity, the study population was divided into two groups based on GI tract-related complications: patients with GI tract-related complications such as bile leakage and GI perforation, and patients with non-GI tract-related complications such as bleeding, vascular complications, wound complications, and other causes. In this analysis, patients with GI-tract related complications requiring reoperation had lower survival rates than patients with non-GI tract-related complications requiring reoperation (P<0.001) (Fig. 2).
Related Factors for Reoperation
The results of univariate and multivariate analyses for reoperation within 30 days after adult-to-adult LDLT are shown in Table 2. Age<50 years, prolonged hospitalization, and total operation time for liver transplantation were considered as potential risk factors. A multivariate logistic regression model showed that prolonged hospitalization days (odds ratio [OR], 1.007; 95% confidence interval [CI], 1.001 to 1.013; P=0.028), operation time (OR, 1.003; 95% CI, 1.000 to 1.005; P=0.002), and a history of previous HCC-related operation (OR, 1.999; 95% CI, 1.050 to 3.808; P=0.035) were significantly associated with early reoperation.
DISCUSSION
The postoperative complications following LDLT include PNF, acute rejection, infection, vascular complications, and biliary complications [4]. The rate of occurrence of complications may be different from the rate of complications requiring reoperation, as some complications can be solved by non-surgical radiologic or endoscopic interventions. PNF following LDLT—one complication that requires surgical intervention—usually requires a liver retransplantation (re-LT). Therefore, PNF was excluded from the list of complications that required reoperation, and five patients who received re-LT with PNF were also excluded from the study population in this study.
The rates of relaparotomy after LT range from 9.2%–26.2% in LDLT [578] and 14.8%–34.2% in DDLT [510] patients. In this study, 19.4% of LDLT patients required reoperation, and had significantly lower survival rates than the patients who did not (P=0.018). Detailed comparisons of survival rates revealed that the 3-month and 1-year survival rates were significantly lower in the reoperation group, but that the 3-year and 5-year survival rates were comparable across groups. These results suggest that survival rates after LDLT are usually affected by complications that occur in the short term. In addition, survival rates did not appear to correlate with the frequency of complications. However, patients with complications such as bile leakage and GI perforation had lower survival rates.
Several previous studies have reported the risk factors for reoperation after adult LDLT. A portal vein flow rate of <1.0 L/min, a history of upper abdominal surgery, prolonged operation time, severely illness, a MELD score >20, a history of hemodialysis before LT, government insurance, and an increased risk index of donor organs have been variously reported as risk factors for reoperation after LDLT [71112]. However, no study has reported the critical risk factors for early reoperation after LDLT. Based on a multivariate analysis, we show here that the length of hospitalization, operation time, and a history of HCC-related operations were significant independent risk factors for reoperation after LDLT. A history of HCC-related surgery can lead to adhesions between the liver and surrounding organs or tissues, which can in turn increase surgery duration, promote the development of other complications, and lengthen hospitalization.
However, it is difficult to determine whether these two are predisposing factors for reoperation after LDLT. A long operation time and lengthy hospitalization were both reasonable factors identified in the reoperation group. Therefore, it would be appropriate to refer to them as related factors rather than risk factors.
Although we did not identify any risk factors for reoperation found in other studies, we successfully identified high risk groups among the causes of reoperation. When the study population was divided into two groups based on GI tract-related complications, the group with GI tract-related complications showed relatively poorer survival rates compared to the group with non-GI tract-related complications. The survival rate for patients who required reoperation for GI tract-related complications was significantly lower than for patients who required reoperation for non-GI tract-related complications. To the best of our knowledge, this is the first study to focus on classifying risk groups based on survival rates associated with the cause of reoperation after LDLT. Among the causes of reoperation in this study, patients with bile leakage and GI perforation were identified as being at especially high risk of reoperation.
In the present analysis, GI-related complications mainly consisted of GI perforation and bile leakage. Previous studies have reported GI perforation as a rare complication of liver transplantation, with an incidence rate of 1%–5.3% [131415]. In this, there were four cases of small bowel perforation, one case of stomach perforation, and one case of ischemic colitis among patients with GI perforation. Of the six patients with GI perforation, four died. In several studies, GI perforation following liver transplantation occurred mainly due to the use of immunosuppressive agents, leading to intestinal wall necrosis, and perforation [16]. There are various hypotheses regarding the mechanism by which immunosuppressive agents cause GI perforation; however, there is no definitive evidence [17]. Since immunosuppressants are essential for the management of liver transplantation, further investigations are needed to elucidate the role of immunosuppressants in bowel perforation.
Biliary complications are common after liver transplantation, with bile leakage representing the most common complication with a reported incidence of 2%–25% [18]. Biliary leakage usually develops within 30 days of right lobe-LDLT. A bile leak can occur from the anastomosis, the percutaneous transhepatic cholangiography tube tract, the cut surface of the liver (Luschka's duct), or from the cystic duct remnant [19]. The reported risk factors for biliary complications following LDLT include age, sex, ABO compatibility, cytomegalovirus infection, multiple ducts for anastomosis, and the type of reconstruction performed [202122]. In this study, all seven cases of biliary complications requiring reoperation within 30 days after LDLT were due to biliary leakage; one occurred on the cut surface of the liver graft, and the other six were associated with multiple bile duct orifices, similar to those reported in other studies.
The main limitation of this study was its retrospective, single-center design. Because patient data were collected over a long period of time, the indications for reoperation and details of postoperative management may have differed among cases. Although the GI tract-related group was classified as a high-risk group and clearly showed statistically significant differences in outcomes, it was difficult to conduct more detailed analyses due to the small sample size. In addition, we did not analyze the anatomical complexity of the vascular system and bile duct, which may affect the results. Further research and analysis will be needed to examine and explain the poor prognosis of the high risk group. Although this study was performed at a single institution, the results are meaningful because they were obtained from a relatively larger number of patients compared to previous studies. Finally, future studies with more data are needed to clarify the high-risk groups by analyzing and identifying factors of significant relevance to causes and outcomes.
In conclusion, a long hospitalization period, prolonged operation time, and a history of HCC-related operations were independent factors associated with early reoperation after LDLT. Patients who required reoperation after LDLT had significantly lower rates of survival than patients who did not. Survival analysis based on the cause of reoperation following LDLT revealed that patients with bile leakage and GI perforation had higher mortality than those with other causes; thus, patients with these complications were classified into the high-risk group. Understanding the risk factors for reoperation after LDLT in different patient groups will help clinicians identify and adopt proper intervention practices, help reduce patient morbidity and mortality caused by reoperation, and improve patient outcomes.



 XML Download
XML Download