

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Intensity-modulated radiotherapy (IMRT) is widely used to increase the radiation dose to the tumor while reducing the dose to the surrounding organs. For inverse optimization of treatment planning, assignment of the appropriate dose constraints and priorities is important and needs to be optimized for each individual case. Therefore, the skills and experience of the planner significantly affect the duration of treatment planning as well as the plan quality.12) Plan quality can be improved as planning time increases, but it then reaches a certain plateau, which may differ across planners; furthermore, it is difficult to assess whether a given plan is optimal.3) To overcome such inter-planner variation in plan quality and to improve the efficiency of current treatment planning procedures, efforts have been made to generate high-quality plans automatically and objectively, on the basis of the existing high-quality treatment plans.456) Using these methods, a model by which achievable dose-volume constraints for both the target and the organs at risk (OARs) can be predicted is created by learning dosimetric features from various geometric relationships between the target and the surrounding normal organs in previous treatment plans. The clinical efficacy of knowledge-based treatment planning (KBP),7) also known as model-based treatment planning, has been demonstrated for many cancer sites, including liver cancer,8) prostate cancer,9) lung cancer,10) pancreatic cancer,11) and head and neck cancer.12) One such commercially available KBP system is the RapidPlan of the Eclipse treatment planning system (Varian Medical Systems, Palo Alto, CA, USA).
Stereotactic body radiotherapy (SBRT) for spine metastases has mainly been conducted in patients with a longer life expectancy.1314) However, the low tolerance of the spinal cord to radiation is often a factor limiting the delivery of a sufficient tumor cell-killing dose.15) According to the Quantitative Analyses of Normal Tissue Effects in the Clinic, the radiation dose limit of the spinal cord is usually 50 Gy in conventional fractionated irradiation, 20 Gy in three fractions, and 10 Gy in a single fraction.16) The prescription doses for spine SBRT are from 18 Gy in a single fraction to 24–27 Gy in three fractions.17) Spine SBRT has been delivered using linear accelerator-based methods of IMRT, TomoTherapy, and CyberKnife.
In most previous studies, KBP was focused on treatment plans with OARs in parallel rather than serial structures, and which overlapped with the target volume. However, the spinal cord is a representative serial organ where the high-dose region is more critical, while overall dose reduction is important in parallel organs. In addition, since the position of the spinal cord is usually located very close to the PTV and is sometimes surrounded by the PTV, most cases require a high-quality plan, which is technically very demanding. Therefore, in this study, we aimed to evaluate the clinical feasibility of using KBP in spine SBRT.
Materials and Methods
1. Contouring and treatment planning
Contouring was performed for 48 spinal metastases. For each patient the gross tumor volume (GTV) was contoured on a planning computed tomography scan, and the clinical target volume (CTV) was delineated according to the guidelines of the International Spine Radiosurgery Consortium (ISRC).18) Two planning target volumes (PTVs) were defined for simultaneous integrated boost (SIB): PTV-B (PTV for boost: 27Gy/3fractions) and PTV-E (PTV for elective: 24Gy/3fractions). PTV-B was created with a 3-mm margin on the GTV, while maintaining a 2 mm–3 mm margin from the spinal cord when it was adjacent to the spinal cord. PTV-E was extended by a 3-mm margin to the CTV, while maintaining at least a 2 mm–3-mm margin from the spinal cord and with PTV-B subtracted. The prescription doses for PTV-B and PTV-E were 27 Gy and 24 Gy, each delivered in three fractions. As OARs, the spinal cord and esophagus were contoured 2 cm above and below the target volume, respectively.
The baseline treatment plans, called the “expert plan” hereafter, were generated by experienced dosimetrists. In spine SBRT, VMAT with dual arc beams has been demonstrated to be an efficient technique, providing plan quality comparable with that of conventional IMRT.19) Therefore, in this study, all plans were generated using VMAT with two 6-MV arc beams. The first arc rotated in a counterclockwise direction, from 179 to 181 degrees, with a collimator angle of 45 degrees, while the second arc rotated in the clockwise direction, from 181 to 179 degrees, with a collimator angle of 45 degrees.
2. Knowledge-based planning
RapidPlan of Eclipse version 13.6 was used for KBP of spine SBRT. The three main components of the model generation process of RapidPlan were as follows:
Among the 48 spine SBRT plans, 26 cases were randomly selected for KBP model training. According to the geometric relationships between the target and OARs, the so-called “geometry-based expected dose” (GED) was computed and the contributing features, such as the volume-surface distance and geometric shape of a structure, were determined. These features consisted of a GED histogram, OAR volume, overlap volume with targets, out-field volume, and target volume. During training, the model was created through principal component analysis (PCA) and a PCA regression technique, the standard deviation for the OAR.
When the training was completed, the performance of the model was evaluated. Possible outliers which might be excluded from the model were determined based on the Cook's distance according to the PCA regression. The model was considered inaccurate if there were more than 4 outliers.
3. Model validation
The model was validated as follows:
1) Closed-loop validation
The 26 treatment plans that were used for training were re-optimized using the KBP-generated model. The KBP-generated plans were compared with the expert plans to evaluate the reproducibility of the model.
2) Open-loop validation
The remaining 22 treatment plans that were not used for training were re-optimized using the KBP-predicted model. The KBP-generated plans were compared with the expert treatment plans to evaluate the clinical applicability of the KBP plan (Fig. 1).
4. RapidPlan-based treatment planning process
The RapidPlan treatment planning process was carried out as follows. The generated model was applied to a new spine SBRT plan to yield a generalized estimated DVH for the spinal cord and esophagus. The priority of dose constraint was assigned to this predictive DVH. Priorities for the upper and lower limits for the target volumes (PTV-B and PTV-E) were manually assigned on a case-by-case basis. For spine SBRT, the maximum dose or 1-cc dose to the spinal cord was considered important. Because the dose limit of the predicted DVH alone was difficult to achieve with the maximum dose constraint, an upper dose limit was additionally applied on a case-by-case basis (Fig. 2). The RapidPlan was used by two planners who had little experience with VMAT plan optimization.
To improve the dose distribution and uniformity in the treatment plan, the treatment planner often creates certain virtual volumes to assign dose-volume constraints for optimization. The virtual volumes included a ring structure surrounding the PTV to increase rapid dose fall-off outside the PTV and an expanded structure from the spinal cord to reduce the dose to the spinal cord. To analyze the effect of these virtual volumes on RapidPlan, statistical tests were performed with the KBP-generated plans generated with and without virtual volumes.
5. Statistical analysis
To evaluate the target dose coverage and uniformity, the minimum dose (Dmin), mean dose (Dmean), and maximum dose (Dmax) of the KBP-generated plans were compared with the expert plans. For OARs, D0.35cc and D1.2cc of the spinal cord and D5cc of the esophagus were compared, as suggested by the RTOG0915 protocol.20) Paired t-test was then used to evaluate the statistical difference between the expert plan and the corresponding KBP-generated plan. SPSS version 22.0 (IBM Corp., Armonk, NY, USA) was used and P<0.05 was considered statistically significant.
Results
Among the 48 patients, the tumor involved the cervical spine in 4 patients, thoracic spine in 36 patients, and lumbar spine in 8 patients. Only the spinal cord was considered as an OAR; therefore, we excluded the region below the second lumbar vertebra. The average volumes of PTV-B and PTV-E were 17.4 cm3 (range: 3.0 cm3–76.5 cm3) and 23.8 cm3 (range: 0.8 cm3–98.4 cm3), respectively. Fig. 3 shows a representative KBP plan. In terms of dose distributions and DVHs, the KBP plan was more suitable for clinical use than the expert plan. None of the expert plans were excluded in the KBP model as outliers. The goodness of fit for the spinal cord and esophagus was 0.999 and 1.0, respectively.
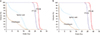
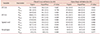
Table 1 summarizes comparisons of dosimetric parameters between the RapidPlans and the expert plans in the closed- and open-loop validations. In the closed-loop validation, the maximum dose to the target was higher in the KBP plans than in the expert plans. On the other hand, the minimum dose to the target was lower in KBP plans, although the difference did not exceed the maximum of 0.6 Gy. The maximum dose to the spinal cord and esophagus was significantly lower in the KBP plans. The dose to the target in the open-loop showed a similar pattern as that in the closed-loop, while the difference was not more than 0.7 Gy. However, no significant dose reduction was observed in the spinal cord and the esophagus in the KBP plans, in contrast to the closed-loop validation. Although the average dose reduction in the spinal cord and the esophagus was observed in the DVHs, the maximum dose was similar to that of the expert plans in both closed- and open-loop validations (Fig. 4).
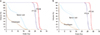
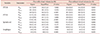
Table 2 and Fig. 5 show the dosimetric parameters for the expert and KBP plans with and without use of virtual volumes. Virtual volumes were used in 38 of 48 expert treatment plans. Regardless of the use of the virtual volume in the dose parameters for PTV-B, the KBP plans significantly increased the maximum dose and reduced the minimum dose, compared with the expert plans. There was no significant difference in the dose variables for PTV-E, regardless of whether the virtual volume was used.
For the OARs, a significant dose reduction was observed only in the esophagus when a RapidPlan was used with a virtual volume. In the DVH, the KBP plan without the virtual volume showed similar results to those of the expert plan.
The dose homogeneity of the target was slightly, yet statistically significantly, worse in RapidPlans for both openand closed-loop validations. The difference in uniformity reached 0.03 between the expert and KBP plans with virtual volumes but was less than 0.01 between the expert and KBP plans without virtual volumes (Table 3).
Discussion
The basic concept of KBP is to learn, from previous high-quality plans, the achievable dose distributions by analyzing the geometric relationship between targets and OARs in these plans, and then to apply this knowledge to manage the quality of the treatment plan and to achieve a high level of plan quality, regardless of the experience of the treatment planners.
This geometric relationship is analyzed using the overlapping volume histogram (OVH)5) and the distance to the target histogram (DTH).21) In previous KBP studies on patients with pancreatic cancer,11) prostate cancer,5) lung cancer,9) liver cancer,8) and head and neck cancer,22) the dose of the OAR could be reduced while maintaining the dose distribution to the target. However, there have been only a few studies on KBP for spine SBRT.
Because this study was conducted on spine SBRT, there are some differences from previous studies. Firstly, because the spinal cord and esophagus are both serial OARs, the reduction of the higher dose region is more important than the average organ dose reduction. Secondly the application of SIB treatment with VMAT is another unique feature of this study. Finally, the spine varies from the cervical spine to the lumbar spine, and according to the outline drawing guidelines proposed by the IRSG, the shape of the target varies greatly, depending on the location of the tumor.
Nevertheless, RapidPlan, the commercially available KBP software used in this study, makes it possible to create a clinically usable treatment plan easily, rapidly, and by less experienced treatment planners. If high-quality plans are available, it is also easy to generate the KBP model rapidly. According to a study by Chung et al.,1) which compared the treatment plans for IMRT for gastric cancer at the National University Hospital of Singapore and the University of California-San Francisco, the mean dose to the right kidney, V20%, and the mean dose to the left kidney, the maximal dose to the spinal cord, and the mean dose to the liver were all smaller at the University of California-San Francisco Hospital, which has more experience in this technique. This indicates that the quality of the IMRT plan may vary according to experience. In contrast, the present study demonstrated that KBP plans can maintain good plan quality regardless of the experience of the planners.
In this study, using the RapidPlan, the dose coverage and uniformity of the target were slightly inferior to those of the expert plans. However, the dose to the spinal cord in D1.2cc was decreased by 0.9 Gy, by 0.8 Gy in D0.35cc, and by 0.6 Gy in the esophagus in the closed-loop test. In the open-loop test, D1.2cc of the spinal cord and D5cc of the esophagus was decreased by 0.3 Gy without statistical significance from the expert plan. The mean dose of the spinal cord was statistically significantly decreased. According to Fogliata et al.,8) RapidPlan was successfully modeled and applied to liver cancer, but no dose reduction was observed to the normal liver. Later, when applied to lung cancer and prostate cancer, the overall doses to OARs were reduced, except for an increased dose to the bladder in the open-loop validation.9) The bladder volume receiving more than 70 Gy was relatively increased in the open-loop validation, similar to the observation in this study. Although a decrease in the maximum dose or in hot spots is more important in serial organs, such as the spinal cord, RapidPlan may limit the predicted dose as a DVH line, and since the weights for the points on the DVH line are all equal, an average dose decrease is likely to be more common. This is not an effective approach for serial organ, where reduction of the maximum dose is more important. To overcome this limitation, a normal tissue complication probability model23) or generalized equivalent uniform dose24) can be used, because these models incorporate the biological effect of the radiation on each organ.
In this study, the closed-loop and open-loop tests showed that the minimum dose of the target was decreased while the maximum dose were increased in the RapidPlans compared with the expert plans, but the difference in dose was less than 0.7 Gy for both PTV-B and PTV-E. The difference in the homogeneity index was as small as 0.02. While the improvement in target dose uniformity were reported in head and neck cancer, liver cancer, and lung cancer, in prostate cancer studies, the D99% (99% volume dose) was decreased by 0.6 Gy in the closed-loop test. (1 standard deviation: 0.7 Gy), and by 0.7 Gy (1 standard deviation: 1.1 Gy) in the open-loop test. Therefore, the improvement of target dose homogeneity in the KBP plan is not universal and may be a consequence of the target dose distribution that is affected by surrounding OARs. RapidPlan only provides the expected dose for the OARs; therefore, the target dose must be passively imposed, and as a result, the uniformity of the target can be affected by the imposed target dose constraints.
In this study, we evaluated the effect of virtual volume on KBP plan quality. For IMRT plan optimization, virtual volumes are widely generated and used to increase the minimum dose or decrease the maximum dose to the target, or to decrease the dose of the OARs. In the expert plans, virtual volumes were used in 38 of the 48 cases, while the RapidPlan did not use any virtual volumes. Consequently, the maximum dose of PTV-B was significantly lower in the expert plans utilizing the virtual volumes and the difference was 0.7 Gy. However, the difference was reduced to 0.4 Gy when virtual volumes were not used in the expert plans. In addition, for PTV-E, there was no statistically significant difference for plans in which virtual volumes were not used. Wu et al. reported that imposing a dose constraint on the virtual volume improved the dose uniformity of the target.25) Therefore, the inclusion of clinically used virtual volumes in the KBP model should be studied in future in order to improve plan quality further.
Conclusions
The dose coverage and uniformity for PTV was slightly worse in the KBP for spine SBRT while the dose to the spinal cord was reduced, but the differences were not clinically significant, demonstrating non-inferior plan quality. Even less-skilled treatment planners can easily create clinically feasible treatment plans with the RapidPlan, which can mitigate the difficulty associated with designing treatment plans or the effect of the treatment planners' skill on plan quality.




 XML Download
XML Download