

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Image guided radiation therapy (IGRT) is a recent development in radiotherapy technology. It uses imaging techniques, such as kV imaging, megavoltage (MV) imaging, and cone beam computed tomography, during radiation therapy to improve the precision and accuracy of treatment delivery.1) However, IGRT with computed tomography (CT) imaging remains a challenge, owing to inadequate soft tissue contrast and imaging dose.2)
Recently, a magnetic resonance image guided radiation therapy (MRgRT) system was introduced to the field of radiotherapy.34) Particularly, the MRIdian (ViewRay Inc., Oakwood Village, OH, USA) integrates a 0.35 T split superconducting magnet with a 6 MV flattening filter free linear accelerator, or three Co-60 heads, and has been in clinical use since 2014.5) Magnetic resonance (MR) images show superior soft tissue contrast than conventional CT images and MRgRT also has the added advantage of providing real-time anatomic motion tracking.26) Similar to a conventional radiotherapy machine (e.g., MV LINAC), accurate and precise in vivo dosimetry is required to confirm what extent of the planned dose is delivered to the volume of interest during the MRgRT treatment.789) To accurately compare the planned dose and delivered dose for MRgRT, information on the position of the in vivo dosimeter is necessary.10) Commercial metallic fiducial markers, made of iron, gold, and platinum, can be utilized as reference points in MR images.1112) However, commercial markers are difficult to deform and almost impossible to attach to various types of in vivo dosimeters without air gaps. The presence of air near the markers may significantly degrade the fiducial visibility.13) In addition, the metallic elements have an inherent toxicity.
In the current study, new markers for MR images were suggested for the assessment of accurate positioning of the in vivo dosimeter. The new markers, composed of silicone rubber or urethane rubber, can be fabricated into various shapes and attached to the in vivo dosimeter without air gaps. The signal intensities from the MR images using the new markers were acquired and compared to each other. Additionally, the enhancement of the MR signal intensity, due to the addition of silicone oil to the markers, was also evaluated.
Materials and Methods
1. Materials
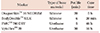
Four types of markers were fabricated using two different base materials. The first base material was silicone rubber. Two commercial silicone rubbers, DragonSkin™ 10 MEDIUM and BodyDouble™ SILK, were used to fabricate the markers. The second base material was urethane rubber and the commercially available PMC™ 780 DRY and VytaFlex™ 20 were used for the markers. All these materials are made by Smooth-On Inc. (Macungie, PA, USA).14) Fig. 1 shows the fabrication of the markers and Table 1 shows the type of base material, pot life, and curing time of each marker. We followed the same fabrication processes outlined in previous work done by other groups.1516) The markers were contained in 50 mL plastic conical tubes, the diameter and length of which were 3 cm and 11.5 cm, respectively. The tubes were then placed in a vacuum chamber to remove the air bubbles produced during mixing and curing the markers. The curing time varied with respect to the marker type (Table 1); however, all the markers were subject to air pressure of 60 psi in the vacuum chamber. For the fabrication of the markers with silicone oil (KF 96 1000cs; Shin-Etsu Inc., Tokyo, Japan), the amount of oil was measured at 20% of the respective marker weight and was added to each marker before the markers were contained in the plastic tubes.
2. Acquisition of magnetic resonance image
The MR images of the markers were acquired by MRIdian with 0.35 T. A true fast imaging was used with a steady state precession sequence, yielding a T2/T1-weighted contrast for all MR scanning.5) The resolution of the MR images was 1.5×1.5×1.5 mm3, with an imaging time of 128 seconds, and the field of view was 40×43×40 cm3.
The acquired MR images were saved in DICOM format and the signal intensity of the images was analyzed. The analysis was conducted using ImageJ (NIH, Bethesda, MD, USA), which has been widely used as a software tool for MR image evaluation.10) The signal intensities were averaged over circular regions of interest (ROIs,) with a diameter of 2 cm at the central region of the marker image, from 20 slices per marker.
Results
Fig. 2 and Table 2 show the MR images and the signal intensities and standard deviations of ROIs for each marker, respectively. Among the markers without the added silicone oil, VytaFlex™ 20 had the highest signal intensity in arbitrary units (a.u.). BodyDouble™ SILK and PMC™ 780 DRY had similar levels of signal intensity. The maximum relative difference of signal intensity between two markers (i.e., VytaFlex™ 20 and BodyDouble™ SILK) was 627%. However, of the markers with the added silicone oil, DragonSkin™ 10 MEDIUM had the highest signal intensity. Its signal intensity increased by 1.26 times, compared to its signal intensity without the silicone oil. The signal intensities of BodyDouble™ SILK and PMC™ 780 DRY, which were originally low, were significantly increased when the silicone oil was added. Particularly, the signal intensity of BodyDouble™ SILK increased by 5.85 times after the silicone oil was added. Furthermore, the relative difference between the signal intensities from the markers with the silicone oil was below 62%.
Discussion
In this study, new markers for MR images were fabricated using silicone rubber- and urethane rubber-based materials and their feasibility as reference points in MR images was demonstrated. In order to improve visibility, silicone oil was added to the fabricated markers and the results showed increased signal intensity for all marker types.
Among the material used for fabricating the markers, DragonSkin™ 10 MEDIUM was proven to be safe and can potentially be used in clinical practice.17) BodyDouble™ SILK was reported to be safe to use for skin.18) However, the toxicity of PMC™ 780 DRY and VytaFlex™ 20, of which the base material is urethane rubber, has not yet been studied for clinical practice. Therefore, one should carefully consider the implementation of those materials in clinical practice.
In contrast to the commercial metallic fiducial markers, the markers in our study can be fabricated with regard to any dimension and design. Since a variety of marker shapes can be fabricated, the markers can be directly attached to in vivo dosimeters, or can encapsulate small-sized in vivo dosimeters.819)
In order to compare the planned dose to the delivered dose during the process of MRgRT, the MR images with the markers should be registered with CT images on the same plane by matching the locations of the markers.20) In future work, we will investigate the effectiveness of the fabricated markers in CT images. Furthermore, to compare the capability of the markers with that of the commercial markers, in terms of image quality from various types of MRI and sequential images, the signal to noise ratio will be evaluated, instead of the signal intensity.
Conclusions
We investigated the feasibility of the use of new markers, based on silicone rubber and urethane rubber, for low magnetic field MR images. Among the four types of markers investigated, DragonSkin™ 10 MEDIUM with added silicone oil displayed the highest MR signal intensity. By adding silicone oil to the markers, it was established that all marker types used in our study have the potential to be used as markers in MRI.



 XML Download
XML Download