

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
A cardiac implantable electronic device (CIED) is a medical device designed for arrhythmia patients. It is placed under the skin, in the chest, to adjust an irregular heartbeat through electrical signals until it returns to normal.1) Because the implantation rate of CIEDs has progressively increased, the CIED patients who are also treated with radiotherapy have increased as well.234) The CIED can be damaged by radiation, during radiotherapy, and the degree of damage on the CIED is dependent on the radiation intensity. Previous studies have shown that a CIED can incur significant permanent damage if subjected to irradiation over 10 Gy; however, minor changes in CIED function are noticed for doses over 2 Gy.5678) This resulted in the establishment of guidelines suggesting that the dose to the CIED should be limited to 2 Gy.9) Therefore, treatment plans should be designed with regard to this limitation and the expected dose should be accurately delivered to the patient, as per the treatment plan.
However, there are some uncertainties in calculating the dosage absorbed by the CIED by using the treatment planning system (TPS). The CIED's boundary is unclear owing to artifacts on the patient's computed tomography (CT) image.101112) It is therefore difficult to accurately assess the dose distribution for the CIED. In addition, several previous studies have reported that the calculated out-of-field doses are different from the actual delivered doses.131415) For Eclipse's analytic anisotropic algorithm (version 8.6), the calculated values showed more than 40% difference compared with the measured values at 4–11 cm from the field edge.16) For Pinnacle (version 9.0), the calculations underestimated the measured values by approximately 50%. The difference was more than 30%, even at a relatively close distance from the field (3–4 cm).17)
It is important to deliver doses below the tolerance level to the CIED during radiotherapy; however, it is difficult to assess the dose of the CIED, due to the uncertainties of the TPS. There is a need for another method of assessing the actual dose delivered to the CIED. Therefore, in this study, we measured the doses delivered to the CIED using the in vivo dosimeter and compared them to the doses calculated by the TPS.
Materials and Methods
1. Information of treatment plan
We conducted this study on three patients, who were fitted with the CIED and were to be treated with radiotherapy at Seoul National University Hospital. The treatment sites were the lungs, for two patients, and the thymus for the third patient. The location of the CIED in the first two patients was outside the treatment area; however, the CIED was in the treatment area for the third patient, as shown in Fig. 1. The treatments planned were volumetric modulated arc therapy (VMAT) for two patients and VMAT-stereotactic body radiotherapy (VMAT-SBRT) for one patient. For each patient, the treatment plans were generated using the Eclipse system, with a progressive resolution photon optimizer algorithm (PO, ver. 13.7; Varian Medical System, Palo Alto, CA, USA) and the Acuros XB dose calculation algorithm (AXB, ver. 13.7; Varian Medical Systems). The details of the treatment plans are shown in Table 1.
2. Measurement using the optically stimulated luminescence detector
The optically stimulated luminescence detector (OSLD) (Landauer, Inc., Glenwood, IL, USA), which is an in vivo dosimeter, was used to measure the radiation dose delivered to the CIED. To measure the delivered dose, the calibration was performed with a calibrated ion chamber whose absolute doses were determined according to the American Association of Physicists in Medicine TG-51 protocol. The linac was calibrated such that a 1 cGy per monitor unit was delivered at a Dmax with a 10×10 cm2 field size and a source-to-surface distance of 100 cm.18) The calibration of the OSLD was applied according to the dose level from 0 to 5 Gy. The dose calibration curve was obtained by plotting the doses as a function of the OSLD reading, for each OSLD. In order to acquire the statistical uncertainty, each calibration point was analyzed 3 times. Each curve was fitted to a respective second-order polynomial function. For all measurements, the OSLDs were read 1 hour after irradiation, using the MicroStar reader (Landauer, Inc.).
3. Comparing calculated doses with measured doses
Measurements were performed for the three patients using the OSLDs, which were placed on the skin near the CIED. The position of the OSLDs is shown in Fig. 1. The OSLD measurements were recorded during the first treatment and the total measured doses were obtained from the OSLD readings, multiplied by the number of fractions, to estimate the total radiation dose over the entire course. The calculated doses were obtained using the TPS. We contoured the area on the axial CT images similarly to the measured area, and obtained the mean absorbed doses for the area.
Results and Discussion
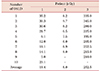
In vivo dosimetry on the CIED were performed using the OSLDs. Table 2 shows the measured doses for the 3 patients. The measured doses were obtained using the OSLD readings multiplied by the number of fractions to estimate the total dose over the entire course. The average of the total dosage measurement points were 19.4, 8.0, and 252.5 cGy, respectively, for the 3 patients. The average measured dose of patient 3 was higher than those of patients 1 and 2 owing to the location of the CIED, as mentioned in the previous section. Because of the high radiation dosage expected for the CIED, in the case of patient 3, a 1-mm lead was placed on the CIED to shield it from the delivered radiation. As a result, the dose reduction of the CIED was approximately 77%.
Table 3 shows the difference between the doses calculated from the TPS and those measured by the OSLDs. In all cases of the investigation, the calculated doses were lower than the measured doses. There are two reasons for this occurrence. Firstly, as mentioned in the Introduction, the TPS has an uncertainty associated with out-of-field dose calculations. As the distance from the treatment field increased, the TPS underestimated the dose with increasing magnitude—up to 55% at 11.25 cm from the treatment field border.16) Secondly, the TPS also has an uncertainty associated with the calculation of surface doses, within ±25%.19) In addition, the differences can also be attributed to the measurement dimension. The OSLD measured the point dose, but calculated doses from the TPS extracted the area doses. To consider the dimension differences in this study, we compared the mean point doses, measured by the OSLD, to calculated values from the TPS. In future studies, we intend to measure the doses in 2D, using other dosimeter types, and compare the maximum doses of the measured and calculated values.
Conclusion
In this study, we measured the doses delivered to a CIED during radiotherapy and compared them with those calculated from the TPS. The results showed that the calculated doses had associated uncertainties that underestimated the actual dosage absorbed by the CIED. To prevent a malfunction of the CIED, it is safer for the CIED patients to use in vivo dosimetry during radiotherapy.



 XML Download
XML Download