

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Children with delayed language development are frequently encountered by pediatricians, but their parents have a lot of anxiety. Several studies have shown that the prevalence of language delay in preschool children is known to be 2–19%.12345 Law et al.6 also reported a high prevalence rate of 2–15% in children two to five years old in the United Kingdom.
Language performance in early childhood is highly related to school age cognitive ability and educational performance as well as predicting verbal and nonverbal language ability after growth.78 It is very important to diagnose this condition early with proper language screening tests because through early language intervention of children with language impairment language function can be expected to show improvement.
Language specific tests, such as the Sequenced Language Scale for Infant (SELSI), the Preschool Receptive-Expressive language Scale (PRES), and the Receptive and Expressive Vocabulary Test (REVT) are usually used as standardized tests for language ability evaluation in the pediatric age group. However, it is difficult to use in pediatric clinics because these tests require well-trained language therapists and take more than 40 minutes per test. On the other hand, clinical screening tests such as the Korean Infant and Child Developmental Test (KICDT) take less time and are relatively simple to be used by pediatricians in primary medical institutions.
The KICDT is designed to assess a child's developmental age in 5 functional domains, 1) gross motor, 2) fine motor, 3) social-personal, 4) language, and 5) cognitive-adaptive skills.9 The language domain of the KICDT can be used to quickly screen children for developmental language delays.
This study aims to investigate the usefulness of the clinical screening test (KICDT) compared to language specific tests such as SELSI and PRES in language evaluation. Here, we compare and analyze the relationship between the language domain Developmental Quotients (DQs) of the KICDT and SELSI/PRES in children aged 8–60 months.
MATERIALS AND METHODS
The participants were 615 children (M:F=459:156, mean age=35.3±11.6 months) with developmental delays who visited the Department of Pediatrics at Chonbuk National University Hospital from January 2013 to December 2016. This study was performed with approval from the Institutional Review Board of Chonbuk National University Research Council (CUH 2018-08-030).
All participants underwent the KICDT and SELSI or PRES at the same time, and the test results were acquired through a retrospective chart review. All patients were divided into two groups according to their age. 340 children aged 8–36 months underwent KICDT and SELSI, and 275 children aged 37–60 months were tested using the KICDT and PRES at the same time.
The language DQ of KICDT which is obtained from each patient was compared with the DQs of SELSI or PRES of the patient. The DQs of SELSI or PRES include receptive language quotient (RLQ), expressive language quotient (ELQ) and total language quotient (TLQ). The sum of the RLQ and ELQ is defined as the total language quotient (TLQ).1011
Each developmental quotient of SELSI or PRES was converted into percentile ratio of the age equivalent so that the language developmental status (normal, borderline, or delay) can be suggested through the ratio. Then the agreement between suggested language developmental status from SELSI or PRES and LDQ of KICDT was checked. In KICDT a cut-off value is indicated with a language developmental quotient (LDQ). LDQ ≥115 is advanced, 85≤LDQ≤114 is normal, 70≤LDQ<85 is borderline, and LDQ<70 is delay in KICDT. In SELSI or PRES a cut-off value is indicated with a percentile ratio of DQ. Percentile ratio of DQ (P. ratio of DQ) ≥84 is advanced, 16≤P. ratio of DQ<84 is normal, 2.3≤P. ratio of DQ<16 is borderline, and P. ratio of DQ<2.3 is delay in SELSI and PRES.
According to the two kinds of cut-off values, all participants were divided into two groups: the normal group and the retardation group. We estimated the sensitivity, specificity, and predictive values of LDQ of KICDT relative to SELSI/PRES based on the cut-off values of the LDQ (85) and the percentile ratio of DQ (16).101112
We used Pearson's correlation coefficient to analyze the relationship between the LDQs of the KICDT and the RLQ and ELQ of the SELSI or PRES. We also used a Chi-square test to cross analyze the correlation between language developmental status from LDQs in KICDT and from the percentile ratio of DQ in SELSI/PRES. All statistical evaluations were completed with PASW Statistics 18, and a p<0.05 was considered significant.
RESULTS
Among the 615 participants who were assessed with the KICDT and SELSI/PRES, 459 (74.6%) were male and 156 (25.4%) were female, and their mean age is 35.3±11.6 months (8–60 months).
The group that performed KICDT and SELSI was composed of 340 children aged 8–36 (mean age, 26.6±6.1) months. 247 (40.2%) were male and 93 (15.1%) were female of them. The other group performed KICDT and PRES was composed of 275 children aged 37–60 (mean age, 46.1±6.6) months. Among them, there were 212 (34.5%) males and 63 (10.2%) females.
For the 615 participants, the correlation coefficients between the LDQs of the KICDT and the RLQs (r=0.706), ELQs (r=0.768), and TLQs (r=0.766) from the SELSI/PRES were indicated in Fig. 1A–C. On the other hand, among the 340 participants less than or equal to 36 months old, the correlation coefficient between LDQs of the KICDT and the RLQs (r=0.674), ELQs (r=0.737), and TLQs (r=0.746) from the SELSI were indicated in Fig. 2A–C. Also, among the 275 participants greater than or equal to 37 months old, the correlation coefficient between LDQs of the KICDT and the RLQs (r=0.729), ELQs (r=0.786), and TLQs (r=0.773) from the PRES were indicated in Fig. 3A–C. Statistically, there was a positive correlation between the RLQs, ELQs, and TLQs of the SELSI/PRES and the LDQs of the KICDT (p<0.05).
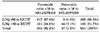
In cross tabulation, the patients belonging to the retardation groups in both KICDT and SELSI/PRES numbered 417 (67.8%). Otherwise, patients belonging to the normal groups in KICDT but not in SELSI/PRES were 151 (24.6%). We derived sensitivity (73.4%), specificity (93.6%), positive predictive value (99.3%), and negative predictive value (22.6%) from the cut-off value of LDQ (85) in KICDT. Calculated χ2 value was 90.1 which was greater than the critical χ2 value (14.9). Based on the results, we can state a significant association between language developmental status from LDQs in KICDT and from percentile ratio of DQ in SELSI/PRES (Table 1).
DISCUSSION
Speech and language issues are the most common problems seen in children with developmental delays. About 20% of these children learn to talk or use words later than other children of their age.13 Although some of the delays might be spontaneously resolved, early detection and treatment are required because early language intervention has a positive impact on linguistic functioning.8 Therefore, developmental screening tests are very important for the early diagnosis of developmental delay.121415
Currently, the SELSI and PRES are the language developmental screening tools most commonly used in Korea. Children under 36 months old are primarily evaluated with the SELSI; whereas, children over 36 months old are assessed with the PRES. The SELSI evaluates children with a total of 112 questions; 56 questions refer to receptive language, and 56 refer to expressive language skills. For children under 36 months old, their caregivers respond to the questionnaires.10 The PRES has a total of 90 questions, in which 45 refer to receptive language and 45 to expressive language. Three questions are selected for children aged 2–3 years every 3 months of development and for those aged 4–6 years every 6 months of development. The PRES uses various methods, such as pictures, objects, instructions, and interviews to examine semantics, syntax, and pragmatics. The results estimate the language developmental age (receptive language age, expressive language age, and combined language age) through the chronological age.11
The SELSI and PRES are useful for evaluating overall language, but they are very time consuming to administer in primary clinics. However, the clinical screening test such as the KICDT takes less time and is relatively simple to administer. KICDT is a developmental screening test for infants under the age of 5 years and was developed at the Korean Pediatric Society in 2002. This test is subdivided into 5 sub-domains (gross motor, fine motor, personal-social, language, cognitive-adaptive) and each domain consists of 28 items. The KICDT takes only 10–15 minutes and its scores are described with developmental quotients.161718
Therefore, here we investigated whether the language development category of the KICDT had a close relationship with the SELSI/PRES. Our results suggest that the language development category of the KICDT could be used for screening language developmental delays. Indeed, we found that the LDQs of the KICDT were strongly correlated with the ELQs of the SELSI/PRES. Also, we found the correlation between language developmental status from LDQs in KICDT and from percentile ratios of DQ in SELSI/PRES. The sensitivity, specificity, positive predictive values of LDQ of KICDT relative to SELSI/PRES showed that KICDT was a valid screening test for children with language developmental delay.
The KICDT might hold some practical advantages over the SELSI/PRES, including being less time consuming and relatively easier to use. This is very important for pediatricians. The administration requires a language voucher certificate or a language disability certificate to be provided with a diagnostic language test such as SELSI or PRES when supporting language therapy. However, most pediatricians cannot do this in the outpatient clinic. Under these circumstances, pediatricians are excluded because they cannot perform language tests.
In this study, KICDT was discussed among various screening tests, but what we focused on is the usefulness of screening tests that could be used for patients with language delay. However, most of the previous studies have analyzed the correlations with the Korean Bayley Scales of Infant Development, Social Maturity Scale, Korean-Wechsler Preschool and Primary Scale of Intelligence to confirm the usefulness of KICDT as a screening test in the overall development evaluation.91920
The significance of this study is that we did not confine patients in our study to a specific disease group such as epilepsy or autism spectrum disease, but involved more than 600 patients who had developmental delays with or without other diseases for 4 years from January 2013 to December 2016. In addition, the sensitivity, specificity and predictive values derived from LDQ of KICDT relative to SELSI/PRES were used to confirm the validity of KICDT as a screening test.
There are several limitations to the current study. First, this study was based on retrospective data and conducted in a single center. Second, since our hospital is a tertiary hospital, most of the patients are transferred from the primary clinic and their chief complaints were developmental delay, so there is a sample bias in which this study contains very few normal children. As shown in Table 1, the number of patients with language delay was 12 times higher than normal children. Third, this study was not conducted with a new screening test. The Korean Developmental Screening Test (K-DST) is a new screening test, revised in 2017 and has replaced previous developmental screening tests. Since this study included developmental screening tests conducted from 2013 to 2016, new screening tools were not available. Finally, we also need to examine data from normal control groups to determine the accuracy of this investigation.
The KICDT is a relatively simple appropriate screening that can be performed easily in primary clinics. Further, it is not surprising that the KICDT shows a strong correlation with the SELSI/PRES, as it originated from these instruments. Overall, the LDQ of the KICDT has such a strong correlation with the SELSI/PRES that it could be a useful screening tool for detecting language development delay. Importantly, it can be administered relatively quickly by clinicians.



 XML Download
XML Download