

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Manual thrombus aspiration (TA) during primary percutaneous coronary intervention (PCI) reduces thrombus burden and improves markers of myocardial reperfusion in patients with acute ST-elevation myocardial infarction (STEMI).12 However, its clinical benefits have been a controversial issue of debate. Thrombus Aspiration during Percutaneous coronary intervention in acute myocardial infarction Study (TAPAS) trial3 and other several studies456 showed a mortality reduction with TA. In contrast, in 2 recent multi-center randomized trials, the Trial of Routine Aspiration Thrombectomy with PCI versus PCI Alone in Patients with STEMI (TOTAL)7 and the Thrombus Aspiration in ST-Elevation myocardial infarction in Scandinavia (TASTE)89 failed to show a significant reduction in clinical events including mortality. As a result, the recent guidelines did not recommend routine TA.1011
There is no well-designed Korean data about the clinical impact of intracoronary TA during primary PCI in patients with STEMI. In this study, we sought to evaluate the clinical impact of TA during primary PCI in STEMI patients with pre-procedural Thrombolysis in Myocardial Infarction (TIMI) flow 0, 1.
MATERIALS AND METHODS
1. Study design and population
The study population was derived from the Korea Acute Myocardial Infarction Registry-National Institutes of Health (KAMIR-NIH) from November 2011 to December 2015. The KAMIR-NIH is a prospective, multicenter, web-based observational cohort study to develop the prognostic and surveillance index of Korean patients with acute myocardial infarction (AMI) from 20 centers in Korea and has been supported by a grant from Korea Centers for Disease Control and Prevention since November 2011.
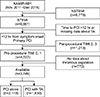
We analyzed a total of 13,516 patients with AMI undergoing primary PCI. The inclusion criteria for the current study were as follows.
We, therefore, enrolled patients in the current study. The study flow diagram is shown in Fig. 1. All patients submitted the written informed consent forms for participating in the registry. Trained study coordinators at each of the participating institutions collected the data using a standardized format. Standardized definitions of all variables were determined by the steering committee board of KAMIR-NIH. The present study was conducted according to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the institution's human research committee.
2. Classification of coronary angiographic findings and interventional procedures
Coronary angiography findings were graded based on the ACC/AHA (American College of Cardiology/American Heart Association) classification system.12 This is also associated with the complexity of the lesions. Blood flow on coronary angiography was evaluated based on the TIMI flow.13 Primary PCI was performed according to the standard guideline.1415
3. Study endpoints
The primary efficacy end-points were major adverse cardiac event (MACE), defined as a composite of the cardiovascular death (CVD), myocardial infarction (MI) or stroke at 30-day and 1-year. The secondary efficacy end-points were all-cause mortality and CVD during 30-days and 1-year.
4. Statistical analysis
Continuous variables were expressed as mean±SD (SD: standard deviation) or the median and interquartile range, and they were compared using the independent t test or Mann-Whitney U test between the two groups. Categorical variables were compared with Pearson's Chi-square or Fisher's exact tests between the two groups. Due to the significant baseline differences between the PCI with TA group and the PCI only group, the propensity score matching method was used. Before using propensity score matching method, we performed multiple imputation procedures to fill in the missing data of several important variables such as the left ventricular ejection fraction, initial systolic blood pressure and initial heart rate. The propensity scores were estimated using a multiple logistic regression model that contained 32 covariates in Table 1. The matching ratio was 1 to 2. Model discrimination was measured using c-statistic, and calibration was assessed by the Hosmer-Lemeshow goodness-of-fit test (c-statistic: 0.647, Hosmer-Lemshow: p=0.169). The results of the multivariable models were verified using propensity score matching method. All statistical tests were 2-tailed, and a p value<0.05 was considered statistically significant. Statistical analysis was done using the SPSS version 21.0 (Statistical Package for Social Science, SPSS Inc., Chicago, IL, USA).
RESULTS
1. Baseline characteristics
A total of 3749 patients were enrolled in this study. Enrolled patients were divided into 2 groups: PCI with TA group (n=1630) and PCI alone group (n=2119). The TA during PCI procedure was performed in 43.7 percent of the total patients.
Baseline characteristics of patients before and after propensity score matching were shown in Table 1. Patients in the PCI with TA group were younger and had higher body mass indexes (BMI). In laboratory data, creatinine clearance and high-density lipoprotein (HDL) levels were significantly higher in the PCI with TA group. In hemodynamic and procedural characteristics analysis, patients in the PCI with TA group had lower Killip classes, heart rates and shorter door-to-balloon time at admission. More patients in the PCI with TA group had right coronary artery disease as the infarct-related vessel and many more cases of single vessel diseases. The higher number of transfemoral vascular approaches and culprit only PCI were found in the PCI with TA group. Glycoprotein IIb/IIIa inhibitor, statin and clopidogrel were used more often in the PCI with TA group than the PCI alone group.
After propensity-score matching, the differences in clinical variables between the PCI with TA group and the PCI alone group were less significant. Higher levels of HDL and creatine kinase-MB (CK-MB) were observed in the PCI with TA group. More cases of transfemoral vascular approaches were performed in the PCI alone group. In addition, glycoprotein IIb/IIIa inhibitors were used more often in the PCI with TA group than the PCI alone group.
2. Clinical outcomes
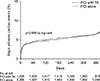
Clinical outcomes of the 30-day and 1-year follow-up before and after propensity matching are shown in Table 2. MACE and all-cause mortality were observed in 308 (8.2%) and 271 (7.2%) patients during the 1-year follow up respectively. With respect to the primary efficacy outcome, there was no significant difference in the incidence of MACE between the PCI alone and the PCI with TA groups at the 30-day and 1-year follow up in all patients. After propensity-score matching, there were also no significant differences in the incidence of MACE between the two groups at 30-days (5.3% vs. 5.3%, adjusted HR with 95% CI: 1.342 [0.826-2.179], p value=0.235 for TA use) and 1-year (8.2% vs. 8.2%, adjusted HR with 95% CI: 1.187 [0.863-1.633], p value=0.291 for TA use). Fig. 2 shows the Kaplan-Meier curves for 1-year MACE between the PCI alone and the PCI with TA groups in propensity-matched cohorts. There was no difference between the two groups in the rate of MACE at 1-year follow-up. Furthermore, the secondary efficacy outcomes, CVD and all-cause mortality were not different between the two groups at the 30-day and 1-year follow up before and after propensity-score matching.
Hazard ratios of various subgroups were analyzed in propensity score matched patients during a 1-year follow up. The frequency of MACE did not decrease in the PCI with TA group in all subgroup analyses (Fig. 3).
DISCUSSION
The major finding of our study is that PCI with TA in patients of STEMI who underwent primary PCI within 12 hours and pre-procedural TIMI flow 0, 1 did not reduce the risk of the adverse clinical outcomes at the 1-year follow up. Moreover, there was no improvement in clinical outcomes in the various subgroup analyses.
The result of our study corresponded well with several large-scale trials.7891617 In the randomized clinical trial of TASTE, routine thrombus aspiration before PCI did not reduce 30-day mortality, rate of death from any cause or the composite of death from any cause, re-hospitalization for myocardial infarction, or stent thrombosis at 1-year.89 The Trial of TOTAL also pointed out that thrombus aspiration did not significantly improve cardiovascular mortality at 180 days. Rather, the investigators of the TOTAL trial found that the risk of stroke in the patients treated with thrombus aspiration was significantly higher within 30 days.7
However, several previous reports disagreed with our findings. In the TAPAS trial,3 1-year cardiac death was reduced in the TA group (HR: 1.93; 95% CI [1.11-3.37], p=0.020). Burzotta et al.6 showed individual patients-data pooled analysis of randomized studies, in which thrombectomy significantly improved the clinical outcomes in patients with STEMI undergoing mechanical reperfusion. Also, Costopoulos et al.2 documented that the use of manual thrombectomy devices was associated with significant improvements in ST-segment resolution, Myocardial Blush Grade (MBG) 3, TIMI grade 3 flow as well as clinical parameters (43% reduction in mortality, p=0.04) in patients undergoing primary PCI.
Some KAMIR data demonstrated that TA showed clinical benefits only in special subgroups. Hachinohe et al.18 compared clinical outcomes between the PCI with TA and the PCI alone groups. Although TA did not improve the clinical outcomes in all patients, TA for LAD occlusion and the use of GP IIb/IIIa inhibitors with TA showed an improvement in 12-month MACE. Sim et al.19 also reported that manual TA during primary PCI did not improve the clinical outcomes at 12-months; manual TA was associated with a higher risk-adjusted MACE rate compared to PCI alone in patients with longer total ischemic times.
The use of glycoprotein IIb/IIIa inhibitors and manual thrombectomy has been debated in previous studies.6182021 In the Intracoronary Abciximab and Aspiration Thrombectomy in Patients With Large Anterior Myocardial Infarction (INFUSE-AMI) trial, an intracoronary bolus infection of the glycoprotein IIb/IIIa inhibitor abciximab was effective in reducing the infarct size, whereas thrombectomy through manual aspiration was not. Reduced embolization and improved myocardial perfusion may improve clinical outcomes. A similar result was also reported in a study published in Korean, in which manual TA was not associated with reduced infarct size assessed by cardiac computed tomography.22 TA may not be a safe procedure and distal embolization including cerebral embolization can occur.717 Coronary thrombus material triggers thrombotic, inflammatory, vasoconstrictor, and other pathways. Evacuating a portion of the thrombus and plaque material resolves only a part of the pathophysiological problem. Disrupting thrombus formation pharmacologically may be more effective.8
Based on the results of the INFUSE-AMI, TASTE and TOTAL trials, The 2015 ACC/AHA guidelines for management of STEMI patients has been recently revised to show that the effectiveness of selective and bailout aspiration thrombectomy in patients undergoing primary PCI is not well established (Class IIB, level of evidence C). Also, routine aspiration thrombectomy before primary PCI is not useful (Class III, level of evidence A).11 Routine thrombus aspiration is not recommended (Class III, level of evidence A), but in cases of large residual thrombus burden after opening the vessel with a guide wire or a balloon, thrombus aspiration may be considered in the 2017 ESC guidelines.10
Our results didn't show any benefit of TA during PCI at the 30-days and 1-year follow-ups. In addition, TA with concomitant use of glycoprotein IIb/IIIa inhibitors did not improve the clinical outcomes. These results imply that TA might have been performed more often in patients with a larger burden of thrombus or in patients with higher risk, resulting in worse clinical outcomes. Types of thrombus can affect mortality during PCI. Some studies have focused on the macroscopic appearance of the aspirated material, subdivided into white (fibrin-rich) and red (erythrocyte-rich) thrombus. White thrombus was typically found in patients with a small thrombus burden and a short ischemic time. By contrast, red thrombus tends to be found in late-presenting patients with a higher risk of distal embolization and cardiac mortality.23 In our study, we could not analyze the burden or the type of thrombus.
This study has several limitations. First, although it was conducted in the patients with MI registered with the KAMIR-NIH and although statistical adjustment including propensity score matching was performed, some confounding factors still existed. Second, we only used TIMI flow grading, which is a subjective categorical variable, and other predictive markers of myocardial perfusion such as corrected TIMI frame count and myocardial brush grade, were unavailable.2425 Third, as we analyzed the events limited within one year, the study might be underpowered to demonstrate the clinical usefulness of TA in STEMI patients.
In conclusion, our study showed that TA during primary PCI as compared to PCI alone did not reduce the incidence of MACE and all-cause mortality and CVD among the Korean patients with STEMI and pre-procedural TIMI flow 0, 1 at the 30-day and 1-year follow-ups.



 XML Download
XML Download