

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Schwannoma or neurilemmoma is an uncommon encapsulated soft tissue tumor arising from Schwann cells. Schwannomas can be found throughout any cranial, peripheral or autonomic nerves containing Schwann cells that make the myelin sheath over the nerve fibers (1). About 25–45% of the all schwannomas take place in the head and neck areas, with only 1% of the intraoral presentation. In previous reports, 84 case reports have been described about the tongue base schwannoma (2). In this report, we describe a rare case of a patient with schwannoma of the tongue base. We also included the review of the literature, concentrating on radiologic imaging findings of tongue base schwannoma and its differential diagnosis.
CASE REPORT
A 16-year-old man with nasal obstruction and snoring was admitted to the otorhinolaryngology outpatient department of the hospital. There was no history of pain while opening or swallowing the mouth, and bleeding from the mouth. However, the patient was suspicious of hot potato voice. Physical examination by an otorhinolaryngologist revealed oropharyngeal mass without any neurologic symptoms. He had no significant past medical or family history and laboratory examination results.
In the pre-contrast neck CT scan, a localized lobulated mass was found at the tongue base. The mass was measured to be approximately 36 × 23 × 41 mm in size. The mass showed relatively homogeneous soft tissue attenuation on the pre-contrast scan. On the CT scans acquired after contrast material administration, multiple nodular rim enhancing lesions were scattered at the peripheral portion of the mass. There was no calcification and intratumoral fat component. The presence of adjacent soft tissue invasion was not definite (Fig. 1). These CT findings of the mass may indicate a benign soft tissue tumor.
On the magnetic resonance imaging, the central portion of the mass showed heterogeneous high signal intensity on the T2-weighted (T2WI) images (Fig. 2b) and similar signal intensity to that of adjacent muscles on the T1-weighted (T1WI) images (Fig. 2a). Peripheral high signal lining was detected on T1WI (Fig. 2c). Multiple nodular rim enhancing lesions were also found on the gadolinium-enhanced fat-suppressed T1-weighted images (Fig. 2d). There was no invasion to the adjacent soft tissue on the MRI like CT scan. The MRI findings also suggested that the mass was a benign solid tumor, such as neurofibroma, leiomyoma and schwannoma. It could rule out the possibility of congenital lesion, such as thyroglossal duct and dermoid cysts, and malignant lesion like the rhabdomyosarcoma.
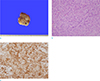
The patient underwent mass excision, and the surgery was successfully completed without any complications. The mass was about 3 × 5 cm sized and located at the tongue base. There was no bleeding tendency on mass, suggesting hypervascularity. Pathologically, the mass proved to be a schwannoma. It showed a bulging contour and brownish tan color in the gross findings (Fig. 3a). In the section, the mass was 42 × 40 × 30 mm sized in dimension. On the microscopic evaluation, most of the tissue from the tongue base mass is composed of spindle cells (Antoni A, 50%) and more myxomatous loosely arranged tissue (Antoni B, 50%) (Fig. 3b). In immunohistochemical stains, tumor cells are strongly positive with S-100 protein (Fig. 3c).
DISCUSSION
The schwannoma, less commonly neurilemmomas or neurinomas, is slow growing and an asymptomatic benign tumor. Despite indistinct etiology of schwannoma, it is suggested that the tumor originates from Schwann cells surrounding cranial, peripheral and autonomic nerves. The tumor was first described by Verocay in 1908 and it has been known to be associated with neurofibromatosis type 2 (3). Around 25-40% of all schwannomas occur in the head and neck regions. Out of these, the incidence of intraoral presentation is about 1–12% (1). Intraoral schwannoma is most common in the tongue. The schwannoma emerges in the following order; palate, mouth floor, buccal mucosa, gingiva, lip and vestibule. Schwannoma in the head and neck commonly develops between the second and third decade of a person's life, but it can occur at any age. It has similar prevalence in men and women. Patients with schwannoma in the tongue usually have clinical presentations as painless lumps (45). Histologically, the tumor is composed of more organized areas with cellular spindle cells (Antoni A) and hypocellular areas with myxoid lesions (Antoni B) (6).
Previous literature has described the general CT findings of the tongue base schwannoma as a well-defined mass with heterogeneous enhancement and it can have cystic or fatty degeneration (7). In our case, a well-demarcated mass with internal heterogeneous enhancing nodular lesions was well visualized and there was no cystic or fatty component in it. These findings make a consideration of differential diagnosis for benign tumor, such as leiomyoma and neurofibroma.
On the MRI, the typical finding is a smooth and well-defined lesion with low to intermediate signal intensities (compared to that of the muscle) on T1WI and high signal intensity on T2WI. If a cystic degeneration, a very high signal intensity on T2WI is shown. A thin peripheral rim of fat on the T1WI (split fat sign), central low signal within the lesion (central sign), and multiple internal small ring-like lesions (fascicular sign) are useful distinguishing features of schwannoma (7). Out of these signs, the fascicular sign was well-visualized, and the split fat sign was suspected in our presented case. However, the central sign was not demonstrated. In general, schwannomas do not undergo malignant transformation (8). So, it typically shows no invasion to the adjacent tissue. However, when the lesion shows a large size, irregular borders and rapid growth in interval imaging, these findings are favoring the malignancy. There has been a few reports about the malignant transformation of schwannoma in the tongue (9). Even if these morphologic characteristics are present, it is difficult to consider the tumor at the first impression when it originates from the tongue base because of its rarity. Our case of schwannoma on the tongue base showed general features on the CT and MR as mentioned above. However, these imaging features are not confirmative for diagnosis of schwannoma because the most acquired benign neoplasms in the tongue, such as leiomyoma and neurofibroma, show similar imaging manifestations as well-circumscribed, enhancing soft-tissue lesions. In this case, CT and MR were performed. CT is helpful for the evaluation of tumors, such as their sizes, shapes, margin, and intratumoral calcification. However, taking into consideration the rarity of the disease, there are limitations regarding accurate information and diagnosis of the lesion only through CT because of dental artifacts in the intraoral area. Therefore, MRI is superior to CT for characterizing the tongue base schwannoma and can provide supplementary information about the tumor. Although theses radiologic multimodalities might be useful for the diagnosis, it cannot be confirmed only by radiologic study, and definitive diagnosis requires biopsy or excision.
Complete surgical excision with intraoral approach is recommended as the best current treatment modality to avoid extra oral scarring (10). However, local recurrence is possible with inadequate complete removal of the tumor. Thus, Post surgery follow ups are necessary.
In conclusion, we report a rare case of tongue base schwannoma with CT and MRI findings. The schwannoma on the tongue base is presented as a well circumscribed, heterogeneously enhanced soft tissue mass on CT and MRI shows fascicular sign with a suspected split fat sign. As these imaging features of the tongue base schwannoma are nonspecific, radiologists need to consider schwannoma as a diagnosis when differentiating the tongue base mass that shows benign looking features. Proper surgical resection with pathologic reports is important to distinguish a tongue base schwannoma from other neoplasms.


 XML Download
XML Download