

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
With an increasing aging population, it becomes increasingly important to ensure that older adults have an independent life. Most older adults want to live in a place where they have lived, rather than in a nursing home or hospital, while maintaining a sense of attachment and social connections.1 This concept is called “Aging in place,” which is defined as the ability to live in one's own home and community safely and independently as one ages.2 To fulfill the goal of aging in place, maintaining the autonomy and independence of older adults has become a key agenda for both individuals and policy makers.34
Preventing frailty and functional dependency in older adults has been one of the ultimate targets of geriatric medicine. Exploring possibilities of interventions to meet these targets, several approaches have been proposed by clinical trials.56 Well-organized exercise programs and nutritional interventions have showed effects in preventing frailty and functional deterioration.57 Additionally, some pharmacological agents such as angiotensin-converting enzyme inhibitors and Vitamin D have been investigated for frailty prevention.89
In order to ensure effective prevention, it is also important to identify older adults who are at risk of functional dependency earlier. A number of studies have been conducted to identify these risk groups, and most studies have attempted to identify the relationship between frailty and subsequent dependency.1011 However, assessing the frailty spectrum often takes more than 30 minutes using various questionnaires and physical examinations. Because of this complexity, assessing frailty might be not feasible in most primary care settings. Furthermore, frailty has multidimensional facets such as physical, emotional, cognitive and social aspects, and identifying the relationship between each element and dependency is complex in a practical sense. Thus, for easier application in real world clinics, a simpler tool is definitely needed.
Recently, some studies have explored the predictability of gait speed as a marker for physical frailty.1213 Numerous studies have shown that gait speed can predict further functional and cognitive decline, mortality, falls, and institutionalization.1415 However, in most studies, gait speed has been measured at a distance of 4 m or 6 m; this measurement is usually difficult to implement in the confined space of clinics, especially in primary care settings. One prior study has examined the association between baseline values on the Timed Up and Go (TUG) test and functional dependency occurrence.16 However, the sample size was small, and the follow-up period was only two years. Therefore, the observation period was relatively short to assess the early prediction ability of the TUG test.
Thus, this study aimed to confirm the association between baseline TUG test results and subsequent functional dependency occurrence in the real world using a large, nationally representative Korean sample from national health screening and insurance data.
METHODS
Study setting
This study used TUG test results from the Korean National Screening Program for Transitional Ages (NSPTA). The NSPTA is a part of the Korean National Health Insurance (KNHI) service that is a nationwide single-payer, government-based mandatory system of healthcare delivery. When people reach the age of 66, the NSPTA program is provided by KNHI, to screen chronic diseases and to assess the health risks associated with aging. The NSPTA includes medical questionnaires (past medical history and health behavior), laboratory tests (blood sugar, cholesterol, and etc.), questionnaires for screening of cognitive function and depression, and the TUG test.17
Functional dependency occurrence was defined as having begun to receive Long-Term Care Insurance (LTCI) services. LTCI is a Korean mandatory public insurance for older adults aged 65 years and above or for persons who are younger than 65 who have specific geriatric syndromes with functional impairment.18 Following an assessment process certifying the presence of a certain level of disability in physical and cognitive functioning, supporting services are provided. These services include various home cares to assist functional impairments or admission to long-term care facilities.
Data source and study population
This study used the National Health Insurance Service-Senior Cohort database, which comprises a total of 558,147 randomly sampled people of KNHI who were over the age of 60 in 2002.
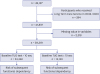
For this study, the people who were 66 years old who had participated in the NSPTA program during 2007–2008 were selected. The initial population was 42,131 participants. Among the population, the participants who received the LTCI service before 2010 were excluded (n = 294), because as the LTCI began in 2008, the people who already had functional dependency were thought to have received LTCI service earlier. This study aimed to analyze the occurrence of dependency, so we did not include them in order to exclude baseline dependency. Participants with missing records of the TUG test or other covariates (n = 2,318) were also excluded. Ultimately, 39,519 participants were included in the final analysis (Fig. 1).
Variates
Independent variate
The TUG test was performed on the examination day of the NSPTA at community hospitals. Following the protocol, the time a participant took to rise from a chair, walk at a comfortable pace to a marking on the floor three meters away, make a turn, walk back to the chair, and sit down was recorded with the timer starting when the participant asked to begin. Regular footwear and customary walking aids were allowed, if needed. Mobility impairment was defined as taking 10 seconds or longer to perform the TUG test.
The cut-off of the TUG test has not been clearly defined yet, and distributions of TUG test results depend on specific protocols (usual pace or maximal effort for walking speed) and demographic backgrounds according to studies.1920 However, 9–10 seconds has been mostly used as the cut-off for this test in different populations.212223 In this population, when we plotted a Receiver Operating Characteristic curve for predicting functional dependency, the cut-off that maximizes sensitivity and specificity was found to be 9.5 seconds (area under curve 0.57, sensitivity 52%, and specificity 62%). This cut-off was similar to a study in Japan that is ethnically similar to Korean.16 Also, the cut-off was consistent with the recent studies which showed that TUG test predicts fracture and dementia–known risk factors of dependency.2224 Because the actual measurements were made in integer units in this population, we rounded it up and selected 10 seconds as the cut-off for the final analysis.
Outcome variate
Dependency occurrence was defined as having begun to receive LTCI services. In the LTCI system, if people apply for the services, well-trained assessors visit the applicant’s home and interview the applicant or his/her primary caregivers. A structured questionnaire is used to evaluate physical and mental status. This questionnaire is a 52-item assessment instrument containing five domains of function and conditions, namely, activities of daily living (ADL), cognitive function, behavior problems, nursing care needs, and musculoskeletal conditions. The questionnaire was developed by the Korean Elderly Care Planning Project in 2004, and was evaluated by the Korean Ministry of Health and Welfare as an appropriate item for measuring elderly care needs.25 Results of the assessment are entered into the computer to calculate the applicant' s standardized scores for care needs. A Community Needs Assessment Committee composed of physicians, nurses, and other experts in health and social services reviews the assigned scores of the applicant, medical statement of the primary care physician, and specified comments by the assessors. If the need for an LTCI service is recognized, the committee decides to provide the services to the applicants.18
Covariates
The following variates that can affect functional dependency were included in the analysis: gender; past medical history, including hypertension, diabetes mellitus, dyslipidemia, stroke, and heart disease; baseline cognitive function; depressive mood; and baseline ADL.26
Information on relevant comorbid conditions (hypertension, diabetes mellitus, dyslipidemia, stroke, and heart disease) was obtained from the screening questionnaire. Depressive symptoms were assessed with a three-item questionnaire extracted from the Geriatric Depression Scale, namely Items 2, 17, and 22, which relate to loss of interest, feelings of uselessness, and feelings of hopelessness, respectively.27 A negative response to any of the three items was regarded as evidence of depressive symptoms. Baseline cognitive function was assessed using the Prescreening Korean Dementia Screening Questionnaire (KDSQ-P), which is scored from 0 to 10; a higher KDSQ-P score indicates more severe cognitive decline.28 Patients with total scores ≥ 4 are recommended to receive further evaluation for cognitive function. The KDSQ-P has shown a significant correlation with the Korean version of the Mini-Mental State Examination.28 Baseline ADL was also obtained from the questionnaire; six ability-related items for feeding, dressing, toileting, bathing, meal preparation, and ambulation were administered. A negative response to any of the six items was regarded as indicating impaired ADL function.
Statistical analyses
Data were summarized as numbers with percentages for each variable. For clinical characteristics based on TUG test results, we conducted a group-wise comparison using a chi-squared test. Statistical differences between the two groups were represented using P values (Table 1).
Table 1
Characteristics of study population according to baseline TUG test results
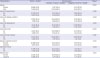
Values are presented as number (%).
TUG test = Timed Up and Go test, ADL = activities of daily living.
aTaking 10 seconds or longer to perform the TUG test was regarded as being functionally impaired; bComparison was performed using the χ2 test for each variable; cTotal percentages may not equal 100% because of rounding; dInformation about hypertension, diabetes mellitus, dyslipidemia, stroke, and heart disease was sought in the questionnaire; eBaseline cognitive function was assessed using the Prescreening Korean Dementia Screening Questionnaire scored on 0–10 points. Higher score indicates cognitive decline. 4 points or more were assessed to indicate decreased cognitive function; fDepressive mood was defined by a negative answer to any of the three screening questions extracted from the Geriatric Depression Scale; gADL was considered impaired if a negative answer was provided to any of the six screening questions.
![]()
We followed up with participants from the day of NSPTA screening until the occurrence of dependency, death, or the last follow-up day (December 31, 2013), according to which came first. However, because we excluded the participants who received LTCI before 2010, we could observe the first occurrence only since January 1, 2010.
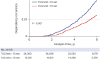
The association between the previously known risk factors of dependency (men gender, past medical history of hypertension, diabetes mellitus, dyslipidemia, stroke, heart disease, baseline cognitive function, depressive mood, and baseline ADL)26 and subsequent functional dependency was assessed using the Cox proportional hazard regression model with univariate and multivariate analysis (Table 2). The association between baseline TUG test results and subsequent functional dependency occurrence was assessed using the Cox proportional hazard regression model with univariate and multivariate analysis, including previously known risk factors of dependency. In addition, the same analyses were repeated for the population with an intact baseline ADL. The associations were represented as hazard ratios (HRs) and 95% confidence intervals (CIs) (Table 3). A Kaplan–Meier curve was used to assess the relationship between TUG test results and dependency occurrence. The statistical significance of the Kaplan–Meier curve was tested using a log-rank test (Fig. 2). Stata software (version 14; Stata Corp., College Station, TX, USA) was used for all statistical analyses.
Table 2
Association between known risk factors and subsequent functional dependency
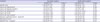
ADL = activities of daily living, HR = hazard ratio, CI = confidence interval, aHR = adjusted hazard ratio.
aMultivariate analysis included gender, past medical history (hypertension, diabetes mellitus, dyslipidemia, stroke, and heart disease), baseline cognitive function, depressive mood, and baseline ADL; bInformation about hypertension, diabetes mellitus, dyslipidemia, stroke, and heart disease was sought in the questionnaire; cBaseline cognitive function was assessed by the Prescreening Korean Dementia Screening Questionnaire scored on 0–10 points. Higher score indicates cognitive decline. 4 points or more were assessed to indicate decreased cognitive function; dDepressive mood was defined by a negative answer to any of the three screening questions extracted from the Geriatric Depression Scale; eADL was considered impaired if a negative answer was provided to any of the six screening questions.
![]()
Table 3
Association between baseline TUG test result and subsequent functional dependency

TUG test = Timed Up and Go, HR = hazard ratio, CI = confidence interval, aHR = adjusted hazard ratio, ADL = activities of daily living.
aMultivariate analysis included gender, past medical history (hypertension, diabetes mellitus, dyslipidemia, stroke, and heart disease), baseline cognitive function, depressive mood, baseline ADL, and baseline TUG test result; bTaking 10 seconds or longer to perform the TUG test was regarded as being functionally impaired; cADL was considered impaired if a negative answer was provided to any of the six screening questions.
![]()
RESULTS
Study population characteristics
Among the 39,519 participants included in the analysis, 15,159 showed mobility impairment according to their baseline TUG test. The percentage of women was higher in the impaired TUG group than in the normal TUG group (57.8% vs. 50.5%). The rate of stroke (12.8% vs. 11.4%) was significantly higher in the impaired TUG group. The rates for declined baseline cognitive function (22.8% vs. 21.4%), depressive mood (46.3% vs. 44.8%), and impaired baseline ADL (37.7% vs. 36.0%) were also significantly higher in the impaired TUG group (Table 1).
Association between known risk factors and subsequent functional dependency
Among previously known risk factors, past medical history of diabetes mellitus (adjusted HR [aHR], 1.45; 95% CI, 1.16–1.83), stroke (aHR, 2.66; 95% CI, 1.94–3.64), and declined baseline cognitive function (aHR, 1.81; 95% CI, 1.52–2.16) showed higher risks of functional dependency occurrence. A past medical history of dyslipidemia showed a lower risk of dependency occurrence (aHR, 0.58; 95% CI, 0.40–0.84) (Table 2).
Association between TUG test and subsequent functional dependency
The mean follow-up period was 5.7 years. Occurrence rates of dependency were 2.0 and 3.4 cases per 1,000 person-years in the normal and impaired TUG groups, respectively. In the univariate analysis, the impaired TUG group showed a higher risk of dependency occurrence than the normal TUG group (HR, 1.70; 95% CI, 1.45–2.01). In the multivariate analysis, including previously known risk factors, impairment in the TUG test was still associated with higher risk of dependency occurrence (aHR, 1.65; 95% CI, 1.40–1.95), independent of other risk factors. Additionally, in the subgroup of participants with an intact baseline ADL, the impaired TUG group showed a higher risk of dependency occurrence (HR, 1.67; 95% CI, 1.35–2.07). The risk was also higher in the multivariate analysis (aHR, 1.65; 95% CI, 1.33–2.04) (Table 3 and Fig. 2).
DISCUSSION
This study showed that older adults who took more than 10 seconds on the baseline TUG test had a higher risk of subsequent functional dependency occurrence. The predictability of the TUG test was similar or even higher than the known risk factors of dependency—men gender, chronic disease, history of stroke, cognitive impairment, depressive mood, and ADL impairment.
The TUG test is a composite measure of functional mobility. It includes executive function (listening and initiating movements), transfer tasks (standing up and sitting down), walking, and balance.19 The test is a simple and much-studied test, and the test protocol is well established.21 TUG test does not require much time and space - less than a minute and only a 3 m distance and an ordinary chair; therefore, it is easy to perform in an ordinary clinic. From previous studies, the TUG test predicted fall risks,29 deterioration in ADL,30 and nursing home admission.31 In addition, in a recent study, the TUG test showed predictive ability for subsequent dementia occurrence.22
Functional dependency may be caused by both cognitive and physical impairment.11 In a previous systematic review on risk factors of nursing home admission,26 96% of studies found a significant effect of functional impairment on risk of nursing home admission. Additionally, dementia was considered the most common cause for institutionalization. Studies showed up to a 17-fold increased impact of dementia on nursing home admission.26 The TUG test is predictive for both physical impairment and dementia in previous studies.222930 This explains the higher predictive ability of TUG test than other risk factors that only reflect physical or cognitive function.
In this study, the TUG test was predictive for functional dependency even in the population with intact baseline ADL. This means that the TUG test might be more useful than the ADL questionnaire or other risk factor screenings for early detection of risk group. Thus, this study supports the predictive ability of TUG test, and recommends it as a useful predictive tool for the early detection of risk group for future functional dependency.
Physical activity intervention and nutritional support have been shown to be effective in preventing disability and functional dependency.532 Cognitive training and pharmacologic interventions such as Vitamin D are also potential candidates. However, in order for these interventions to have an appropriate effect, it is necessary to identify the risk group and to individualize them.33 The study results indicate that the TUG test would help identify the risk group of future dependency. It would be helpful to provide physical and nutritional intervention to those who show impairment in the TUG test.
Additionally, this study confirmed the effects of previously known risk factors (diabetes mellitus, stroke and declined baseline cognitive function) on the occurrence of functional dependency. Dyslipidemia showed a lower risk for dependency occurrence in this study. This is probably because this study defined dyslipidemia by physician diagnosis or medication using a questionnaire. Dyslipidemia is a strong risk factor for both stroke and dementia that are known risk factors of functional dependency. Early diagnosis and control of dyslipidemia may lower the risk of dependency. However, further investigation by another study is required.
The strengths of this study include the large, nationally representative sample of the older population. Additionally, one of the great strengths of this study is that dependency was defined as initiation of supportive services in the real world, not in a research setting, eliminating potential investigator bias. Additionally, the services include not only institutionalization but also various home-visit cares, so this definition could include varying degrees of dependency.
However, this study has some limitations. First, all the participants were 66 years old at screening, which is a relatively young age for dependency occurrence. Therefore, we could not confirm the usefulness of the TUG test for an older population in their 70s or 80s. However, because more abnormal findings for the TUG test are expected for older age groups, the test is expected to be more useful in those populations. Nevertheless, a future study on a population of a higher age group would be necessary. Second, we could not include some possible risk factors for dependency, namely, socioeconomic status, prior hospital use, and potentially inappropriate medications. We included past medical history of hypertension, diabetes mellitus, dyslipidemia, stroke and heart disease, which were considered to replace prior hospital use. Third, the TUG test protocol in NSPTA manual did not specify the exact shape of the chair. It may have influenced the standardization of the TUG test. However, many studies do not specify chair shape,3435 and there is some opinion that the shape of the chair does not affect the TUG test results.36
In conclusion, impairment in TUG test results increased the risk of subsequent functional dependency occurrence. This suggests that the TUG test might be a useful predictive marker for dependency occurrence. Intervention to prevent functional dependency would be helpful for older adults who are identified as having impairment in the TUG test.
 XML Download
XML Download