

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Food allergy is a worldwide problem, and its prevalence is rising, particularly in infants and children. In addition, food-induced allergic reactions cause a variety of symptoms ranging from minor to fatal reactions, such as anaphylaxis.1 Among the foods that cause allergies, cereal grains are produced and consumed in large quantities worldwide. Cereals, such as wheat, barley, oats, rye, and, rarely, rice, are the causes of immunoglobulin E (IgE)-mediated food allergic reactions in infants and children.2
Barley (Hordeum vulgare) is taxonomically classified under the Poaceae family, and this plant along with wheat, oat, and rye belongs to the Pooideae subfamily.3 Barley is widely consumed by humans, and it is a source of fermentable material used in producing alcoholic beverages, such as whiskey and beer, worldwide.4 In addition, it is used in stews, soups, bread, and biscuits in the Middle East, Europe, and Asia.56 In Korea, it is consumed as steamed barley, barley tea, or used as an ingredient in a variety of traditional bread, cookies, and cereal bars.7
Several case reports about barley allergy have been published, but most of these cases have focused on adult patients with respiratory allergy known as baker's asthma induced by barley flour, or with allergy from beer containing barley.891011 Only two cases of barley allergy have been reported in children in which severe anaphylactic reactions have been observed.412 Only in a few studies, symptomatic details have been evaluated and analysed in relation with the level of barley-specific IgE (sIgE).41012 However, the association between barley-sIgE levels and clinical symptoms has not been evaluated. In Korean children and adolescents, barley was the cause of 0.2% of immediate type of food allergy between 2014 and 2015 based on a large-scale, multi-center case study.13 However, the prevalence of barley allergy has not been evaluated in a population-based study.
In cereal grains, most major proteins belong to the prolamin superfamily, which includes proteins related to the prolamin storage proteins.14 Among them, barley, wheat, and rye contain structurally similar epitopes in different proteins.15 Barley is cross-reactive with wheat and rye since they are closely related taxonomically.2 In particular, barley and wheat showed high antigenic cross-reaction, and there was a correlation between barley-sIgE and wheat-sIgE in children with wheat allergy.16 However, there has been no study on the correlation between wheat allergy and barley allergy as well as level of sIgE concentration of barley and wheat allergy patients.
Thus, this study aimed to identify the clinical characteristics, diagnostic values of sIgE, and co-sensitization with wheat in Korean children with barley allergy.
METHODS
Forty-two patients with a history of ingesting barley who underwent serum barley-sIgE assay at the Department of Pediatrics in Ajou Medical Center, Suwon, Korea, were enrolled in this study from March 2008 to February 2018. Then, the medical records of the patients were evaluated. The barley-allergic (B-allergic) group consisted of 20 children with a history of immediate reaction after the intake of barley, whereas the barley-tolerant (B-tolerant) group consisted of 22 atopic controls who were asymptomatic after the ingestion of barley. The participants in the B-allergic group were further divided into two subgroups according to their symptoms: barley–induced anaphylaxis (anaphylactic group) and barley allergy without anaphylaxis (non-anaphylactic group). Anaphylaxis was diagnosed according to the clinical criteria presented by the National Institute of Allergy and Infectious Disease and the Food Allergy and Anaphylaxis Network.17 The demographic characteristics, symptoms, and immunologic parameters of the participants were evaluated.
Measurement of total IgE and sIgE antibody levels
The serum levels of the total IgE and sIgE of all the participants were determined using the ImmunoCAP technique (Thermo Fisher Scientific, Uppsala, Sweden). The assay showed that the lower limit of sIgE level was < 0.01 kUA/L and the upper limit was > 100 kUA/L. The values < 0.01 and > 100 kUA/L were considered as 0.01 and 101 kUA/L, respectively.
Statistical analysis
The Mann-Whitney U test was used for comparison of continuous variables in demographics and serologic parameters between the study groups. The receiver operating characteristic (ROC) curves were obtained to assess total IgE and barley-sIgE levels for the diagnosis of clinical barley allergy, and the area under the curve (AUC) was calculated to assess the accuracy of the test. Spearman's rank correlation coefficient was used to evaluate the correlation between barley and wheat-sIgE concentrations. A P value < 0.05 was considered statistically significant.
RESULTS
A total of 42 participants aged between 5 months and 16 years (mean age, 2 years) were included in the study analysis. The median ages of children in the B-allergic group (n = 20) and in the B-tolerant group (n = 22) were 1 year and 3 years, respectively. The distribution of concurrent allergic diseases including food allergy overall showed no significant difference between the two groups. All participants in the B-allergic group and 20 out of 22 in the B-tolerant group had known food allergies, mostly to cereals, other than barley allergy. In particular, 15 (75.0%) participants in the B-allergic group had wheat allergy, compared to 18.2% in B-tolerant group. These food allergies were diagnosed by definite immediate reactions after exposure to single food, and details of food allergies other than barley allergy were not investigated in this study. The median levels of total IgE were 241 kUA/L in the B-allergic group and 204 kUA/L in the B-tolerant group, with no significant difference between the two groups. The median level of barley-sIgE was 13.90 kUA/L (range, 0.14–101.00 kUA/L) for the B-allergic group, which was significantly higher (P < 0.001) than that of the B-tolerant group (0.30 kUA/L; range, 0.01–24.40 kUA/L). The demographic profiles of the participants are summarized in Table 1.
Table 1
Demographic profile of the participants
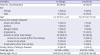
Data are presented as number (%) or median (range).
B-allergic = barley-allergic, B-tolerant = barley-tolerant, FA = food allergy, IgE = immunoglobulin E, sIgE = specific immunoglobulin E.
aP value 0.004; bMost participants had more than one concurrent allergic disease; cP value < 0.001.
![]()
In the B-allergic group, cutaneous symptoms (90.0%) were most common, followed by respiratory symptoms (40.0%) and generalized symptoms (10.0%), and there were no cardiovascular symptoms (Fig. 1A). Moreover, 7 of the 20 (35.0%) children in the B-allergic group experienced anaphylaxis after barley ingestion. Most children (80.0%) in the B-allergic group experienced symptoms within 60 minutes after exposure to barley. The symptom onset times in 10.0%, 40.0%, and 30.0% of the participants were < 5, 5–30, and 30–60 minutes, respectively. Four children in the B-allergic group experienced symptoms after 120 minutes or did not know the symptom onset time (Fig. 1B). All the participants of the B-allergic group developed an allergic reaction after the oral ingestion of barley for the first time. The most common source of barley in the B-allergic group was steamed barley (55.0%), followed by barley tea (15.0%) and breads or cookies (15.0%).
 | Fig. 1Clinical profile of barley allergy. (A) Clinical manifestations of barley allergy. (B) Time interval between exposure to barley and symptom onset in the B-allergic group. Several participants had more than one symptom. Individual symptoms of anaphylaxis were not separately counted as cutaneous, respiratory, cardiovascular, gastrointestinal, or generalized symptoms.B-allergic = barley-allergic.
|
The comparison of the anaphylactic group and the non-anaphylactic group is presented in Table 2. The most common source of barley in the anaphylactic group was steamed barley (71.4%). In the non-anaphylactic group, the most common source of barley was steamed barley (46.2%), followed by barley tea (23.1%) and those breads or cookies (15.4%). The median level of total IgE level was higher in the anaphylactic group than in the non-anaphylactic group (387 vs. 200 kUA/L). The median values of barley-sIgE were 21.00 kUA/L in the Anaphylactic group (range, 9.18–101.00 kUA/L) and 4.41 kUA/L in the Non-anaphylactic group (range, 0.14–101.00 kUA/L). However, all these values were not significantly higher (P > 0.05) than that of the Non-anaphylactic group.
Table 2
The comparison of the anaphylactic and non-anaphylactic groups
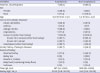
Data are presented as number (%) or median (range). P value > 0.05 for all variables.
FA = food allergy, IgE = immunoglobulin E, sIgE = specific immunoglobulin E.
aMost participants had more than one concurrent allergic disease.
![]()
The ROC curves represented the diagnostic performance of total IgE and barley-sIgE levels in diagnosing clinical barley allergy (Fig. 2). The AUC of barley-sIgE level was 0.882, and barley-sIgE level was a good predictor in distinguishing the B-allergic group from the B-tolerant groups compared to total IgE level (AUC, 0.547). The optimal cut-off value of the barley-sIgE level for the prediction of a clinical barley allergy was > 1.24 kUA/L with a sensitivity of 85.0% and a specificity of 86.4%. The positive decision point of barley-sIgE level with a specificity of 100% in distinguishing the B-allergic group from the B-tolerant group was > 24.4 kUA/L.
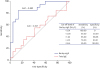 | Fig. 2ROC curves representing the sensitivity and specificity of total IgE and barley-sIgE levels; B-allergic group vs. B-tolerant group.ROC = receiver operating characteristic, B-allergic = barley-allergic, B-tolerant = barley-tolerant, IgE = immunoglobulin E, sIgE = specific immunoglobulin E, AUC = area under the curve.
|
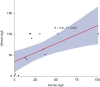
The correlation between the serum levels of barley-sIgE and wheat-sIgE in the B-allergic group with clinical wheat allergy is shown in Fig. 3. Fifteen (75.0%) out of the twenty participants in the B-allergic group experienced clinical wheat allergy, and a positive correlation was found between the concentration of barley-sIgE and wheat-sIgE (Spearman's rho = 0.81, P < 0.001).
DISCUSSION
Barley is widely consumed as an ingredient in a variety of soups, bread, cookies, and alcoholic beverages.567 Barley allergy is less common than wheat or buckwheat allergy, but barley allergy is not uncommon in infants and young children in Korea, and the clinical symptoms are relatively severe.13 However, only a few cases of hypersensitivity to barley have been reported thus far. Thus, this study investigated the clinical characteristics, diagnostic values of barley-sIgE levels, and co-sensitization with wheat in children with clinical barley allergy.
The median age of the patients with clinical barley allergy in this study was 1 year, which possibly reflects the young age of exposure to barley in the form of barley tea and baby food containing barley flour in infants in our region. In this study, the participants in the B-allergic group experienced symptoms extending from skin reactions to anaphylaxis, with a proportion of anaphylaxis of 35.0%. This result was similar to that of previous reports showing that 38.7% and 30.5% of children with food allergy presented with anaphylaxis in the United States and Korea, respectively. Among Korean children with wheat and buckwheat allergy, anaphylaxis was found in 43.5% and 67.3%, respectively, which differs from barley allergy.1318 In a previous study on beer allergy in 20 adults, urticaria was the most common clinical manifestation, and anaphylaxis was reported in 5% of patients.11 The proportion of anaphylaxis to barley in this study is higher than reported in other studies. In adults, barley is mainly consumed as alcoholic beverages, such as beer, which has undergone a complex fermentation process. However, it is often consumed by children as simple cooked food. Food processing methods may cause changes in allergenicity, which causes different symptoms.
Regarding the symptom onset time, all participants (except for four participants who did not know the exact onset time) had symptoms within 60 minutes, and 10.0% presented with symptoms within 5 minutes. This result was consistent with that of a previous study showing that most of IgE-mediated food allergy reactions occur within 2 hours after food consumption.19 Previous reports on the association between the level of barley-sIgE and clinical symptoms are limited. In two cases involving children who experienced anaphylaxis after the ingestion of barley, the levels of barley-sIgE were 35.2 kUA/L and 1.47 kUA/L, respectively.412 From another case report on beer allergy in adults, the levels of barley-sIgE ranged from 0.64 to 6.0 kUA/L.1020 However, studies that evaluate the clinical usefulness and diagnostic value of barley-sIgE measurements in individuals with barley allergy have not been conducted. In this study, the median level of barley-sIgE in the B-allergic group was considerably higher than that in the B-tolerant group, with an optimum cut-off level of 1.24 kUA/L (sensitivity, 85.0% and specificity, 86.4%) and a cut-off level of 24.4 kUA/L has a specificity of 100% in distinguishing the B-allergic group from the B-tolerant group. These results suggest that clinical barley allergy might be diagnosed without conducting the oral food challenge test given that the barley-sIgE level is > 1.24 kUA/L along with a clinical history of barley allergy. Thus, avoidance of barley consumption might be recommended.
Several major barley allergenic components were isolated and identified. The a-amylase/trypsin inhibitor could be the major cause of baker's asthma induced by barley flour.8 In addition, lipid transfer protein 1 and barley protein Z4 are stable toward heat and protease, and they become the major allergens in adults with allergy from beer containing barley.101121 The proteins associated with barley allergy are not fully elucidated. However, recent studies have indicated that 7 kDa,12 9 kDa4 and 14 kDa12 proteins were considered as strong IgE-mediated allergens. Different reports have been published on cross-reaction between grains, such as wheat, barley, and rye,215162223 which taxonomically belong to the Pooideae subfamily, and their seed protein components are structurally similar to IgE-binding epitopes, which could cause a cross-reaction. A high degree of IgE cross-reactivity is observed in barley and wheat, but there has been no study on the correlation between the level of each sIgE concentration of patients with barley and wheat allergy. The results of this study showed that the number of patients with wheat allergy was higher in the B-allergic group than in the B-tolerant group (75.0% vs. 18.2%), and the levels of barley-sIgE and wheat-sIgE showed a positive correlation with wheat allergy in the B-allergic group. Therefore, patients with barley allergy should be cautious when ingesting wheat for the first time, and wheat is not a suitable alternative diet in patients with barley allergy.
The main limitation of this study was its retrospective design. The study divided the groups based on self-reported immediate symptoms after exposure to barely, and oral food challenge test was not conducted. As a result, the development and changes of allergic reactions according to the amount and source of barley could not be investigated in detail. However, to minimize this limitation, this study only included patients with convincing symptoms, recognized by the experienced allergy specialists, and serum barley-sIgE levels above 0.10 kUA/L. Although this is the largest study on barley allergy so far, the results of this study do not reflect differences in age, race, and country because the total number of patients is relatively small, and this study was conducted in a single center. In addition, experiments such as enzyme-linked immunosorbent assay inhibition assay and IgE-immunoblot inhibition assay were not conducted to identify the co-sensitization or cross-reactivity between barley and wheat. However, the outcomes of this study are significant, considering the rarity of barley allergy and the fact that no other studies have been conducted, except for two case reports about children who presented with allergic reactions after barley ingestion.
To the best of our knowledge, this is the foremost study to analyse clinical and immunological profiles, which helps diagnosis of barley allergy, and provides parameters that can aid predicting barley allergy. Additionally, we found that sIgE level was correlated to clinical allergic reactions from barley and wheat ingestion, and results that can help improve the dietary guidelines for children were presented.
In conclusion, barley is consumed in a variety of sources and is an important allergen for children in Korea. This study showed the clinical characteristics of barley allergy and suggested optimal cut-off levels of barley-sIgE for clinical barley allergy. Clinically, cross-reactivity or co-sensitization is often observed between barley and wheat. These results can be helpful in predicting the B-allergic reaction and in dietary guidance in children, while further studies are needed to investigate the prevalence of barley allergy in the population, and cross-reactivities with other grains.
 XML Download
XML Download