

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Proteinuria is a risk factor for cardiovascular (CV) and all-cause mortality in patients with diabetes mellitus (DM) and hypertension1). In addition, microalbuminuria (often defined as 30mg/g≤albumin-creatinine ratio<300mg/g) also predicts mortality independent of the presence of DM and hypertension2). Randomized trials on proteinuria-lowering treatment have emphasized the importance of intervention in slowing the progression of chronic kidney disease (CKD) and reducing the development of CV events3456). However, as patients with proteinuria are typically asymptomatic, screening tests are needed to detect proteinuria7). Dipstick urinalysis is widely used as an initial screening tool for the evaluation of proteinuria owing to its low cost, wide availability, and ability to provide rapid point-of-care information to clinicians and patients89). These attributes suggest that a simple dipstick test for proteinuria is an ideal population-level screening tool for identifying individuals at a high risk of all-cause and/or CV mortality10).
Hypertension can be both a cause and a complication of CKD11) and has been identified as a key modifiable risk factor in patients with decreased renal function12). Proteinuria develops easily in damaged kidneys131415). Moreover, uncontrolled blood pressure (BP) leading to rapid renal dysfunction can cause increased proteinuria1617). Increased proteinuria accelerates the decline of kidney function and the development of CV events15181920). Therefore, several clinical trials have highlighted the importance of strict BP control in slowing the progression of kidney disease and reducing the risk of CV disease82122). However, physicians must be aware of the presence of proteinuria as well as the current BP status when caring for hypertensive patients. In addition, they should carefully consider which antihypertensive agents to prescribe for decreasing BP and proteinuria, as the ideal treatment will produce better renal and CV outcomes.
Antihypertensive agents that interfere with the reninangiotensin system(RAS), including angiotensin-converting enzyme inhibitors (ACEis) and angiotensin receptor blockers (ARBs), have been consistently shown to reduce proteinuria and the rate of renal function deterioration in patients with diabetic and non-diabetic kidney disease, independent of BP. Therefore, RAS blockade is recommended for its renoprotective benefits in hypertensive patients with proteinuria, in addition to its BP-lowering effect2324252627). However, the frequency with which RAS blockade is prescribed in hypertensive patients with proteinuria in Korea has not been reported. In addition, to our knowledge, there have been no studies on the benefit of RAS blockade in patients with hypertension and proteinuria in comparison with the non-use of RAS blockade. We investigated the clinical utility of RAS blockade by dividing the study population into two groups based on the use or non-use of RAS blockade treatment.
Materials and Methods
1. Source of data
The National Health Insurance Service (NHIS) operates the National Health Insurance Sharing Service to provide sufficient support to policy and academic research. The National Health Information database contains records of 1.5 trillion cases and includes data on insurance eligibility, insurance contribution, health examination results, details of medical treatment, long-term care insurance for the elderly, and medical care institutions, as well as a registry of cancers and rare diseases.
We obtained data of the NHIS-Health Screening (NHIS-HEALS) cohort from the NHIS database. The NHIS-HEALS cohort database is a 12-year cohort dataset that includes socioeconomic variables (residence, year and month of death, cause of death, income level), details of medical treatment, and health examination results of approximately 500,000 individuals from 2002 to 2013. The dataset was constructed by randomly selecting 10% of the Korean population who underwent a health examination between 2002 and 2003. This dataset allows longtime observations for investigating causal relationships.
The study was approved by the NHIS review committee and the institutional review board (IRB) of Ewha Womans University Mokdong Hospital (approval no. NHIS-2016-2-066, IRB file: EUMC 2016-03-048).
2. Subjects
For the purposes of the current study, the subjects were restricted to hypertensive patients (defined by the presence of one diagnostic code of hypertension: International Classification of Diseases, 10th revision [ICD10] code I10–I15) with proteinuria (defined as dipstick test result ≥2+). We determined an index date for each patient, defined as the earliest date at which an individual was identified to have hypertension and had a qualifying proteinuria test. All cases were classified between January 1, 2002 and December 31, 2013 in Korea.
The following baseline covariates and comorbidities were considered: age, sex, health insurance type (National Health Insurance System and Medical Aid), disability type (none, light, and severe), history of acute myocardial infarction, congestive heart failure, peripheral vascular disease, cerebral vascular accident, dementia, chronic pulmonary disease, connective tissue disorder, peptic ulcer, liver disease, DM, CKD(defined by the presence of one diagnostic code of CKD: ICD10 code N18), cancer, and paraplegia. Systolic BP (SBP) and diastolic BP (DBP) were also considered. Patients with SBP <140mmHg and DBP <90 mmHg at the time of BP measurement were considered to have well-controlled hypertension, whereas patients with SBP ≥140mmHg or DBP ≥90mmHg at the time of BP measurement were defined as having poorly controlled hypertension.
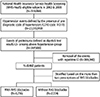
The process of patient enrollment is shown in the schematic flow diagram in Figure 1. The main study outcome was overall survival, which was further divided into all-cause and/or CV mortality (defined by the presence of one diagnostic code of CV mortality: ICD10 code I00-I78) in the absence of ESRD(defined by the presence of one diagnostic code of ESRD: ICD10 code N18.6 or the presence of one therapeutic code of dialysis: O701-O708). Patients were excluded if they had undergone dialysis before the index date. RAS blockade was defined as having at least two prescriptions for an ACEi or ARB medication during the study period.
3. Statistical analysis
In the overall study population, continuous variables and categorical variables were compared between patients with RAS blockade and those without RAS blockade using t-tests and chi-square tests, respectively. Cox proportional hazard regression and Kaplan-Meier analyses were performed to examine the effects of RAS blockade on the development of all-cause mortality, CV mortality, and ESRD. The analyses were performed in a backward stepwise manner. Moreover, we conducted an additional analysis to confirm the multicollinearity between the variables in the final models with three different outcomes. The values of the variation inflation factors (VIFs) were further confirmed. VIF measures the magnitude of the spread of the estimated accounting coefficients when the predictors are correlated. As the spread increases, the regression model becomes unreliable. Empirically, multicollinearity can present potential problems when VIFs are >4. The largest VIF in our model was 1.108, which shows some multicollinearity but was not large enough to be a cause of concern. All reported p-values were two-tailed, and p<0.05 was considered significant. All statistical analyses were conducted using SAS (version 9.3; SAS Institute Inc., Cary, NC, USA) and R version 3.01 for Windows (http://cran.r-project.org/).
Results
1. Baseline characteristics
A total of 6,236 of 8,460 (73.7%) patients were prescribed with RAS blockade. The overall mean age was 56.2 years, and 5,263 (62.2%) of the patients were men. The mean age in the RAS blockade group was significantly lower than that in the non-RAS blockade group. There were significantly more men in the RAS blockade group than in the non-RAS blockade group. With respect to comorbidities, the RAS blockade group had a significantly higher incidence of congestive heart failure and DM but a lower incidence of cancer than the non-RAS blockade group. SBP and DBP were significantly increased in the RAS blockade group compared with the non-RAS blockade group. Moreover, the ratio of patients with poorly controlled hypertension to those with well-controlled hypertension was higher in the RAS blockade group than in the non-RAS blockade group (3,084/3,152 [97.8%] vs. 995/1,227 [81.1%]) (Table 1).
2. Cox proportional hazard analysis for all-cause and/or CV mortality or ESRD
The mean follow-up duration was 129 months. A total of 1,003 patients (11.9%) died during the study period, of whom 273 (3.2%) died of CV events.
The incidence rate ratio, which was calculated as the incidence rate of RAS blockade divided by the incidence rate of non-RAS blockade, was 0.526 (95% confidence interval [CI] 0.463–0.598, p<0.001) for all-cause mortality and 0.587 (95% CI 0.458–0.752, p<0.001) for CV mortality, whereas the incidence rate ratio for ESRD was 1.213 (95% CI 1.012–1.454, p<0.05), which means that the use of RAS blockade may have a protective effect against the risk of all-cause and CV mortality but a detrimental effect on the incident risk of ESRD compared with the non-use of RAS blockade (Supplementary Table 1).
The Kaplan-Meier curves for all-cause and/or CV mortality showed that the survival probability in the RAS blockade group was significantly higher than that in the non-RAS blockade group (Fig. 2A and B).
Cox proportional regression analysis showed that all-cause mortality was decreased by 48.5% in the RAS blockade group compared with the non-RAS blockade group (hazard ratio [HR] 0.515, 95% CI 0.454–0.585, p<0.001). Moreover, RAS blockade significantly reduced the all-cause mortality rate by 39.1%(HR 0.609, 95% CI 0.534–0.693, p<0.001), even after adjusting for age, sex, health insurance system, comorbid diseases, and BP management (Table 2). CV mortality was also significantly decreased by 33.7% in the RAS blockade group compared with the non-RAS blockade group after adjusting for the same variables (HR 0.663, 95% CI 0.515–0.854, p=0.002) (Table 3).
In contrast, 682 patients (8.1%) progressed to ESRD during the follow-up period. Unlike all-cause and/or CV mortality, RAS blockade was not significantly associated with a decrease in the incidence of ESRD compared with non-RAS blockade after adjusting for the same variables. Only Kaplan-Meier analysis showed that ESRD was significantly increased in the RAS blockade group compared with the non-RAS blockade group (Fig. 2C).
Discussion
In this study, 73.7% of patients with hypertension and proteinuria were treated with RAS blockade, whereas 26.3% were not. In addition, RAS blockade was significantly related to reducing the all-cause and/or CV mortality by 39.1% and 33.7%, respectively. However, RAS blockade was not more effective in reducing the development of ESRD than non-RAS blockade (Table 4).
Proteinuria in a person with high BP is indicative of declining kidney function and accelerates the development of CV events151617181920). Therefore, emphasis should be placed on reducing proteinuria and strictly controlling BP for better renal and CV outcomes82122). To date, RAS blockade is known to have an effect of decreasing proteinuria and lowering the rate of renal function aggravation in patients with diabetic and non-diabetic kidney disease, independent of BP control. Therefore, in hypertensive patients with proteinuria, RAS blockade is recommended for its renoprotective benefits in addition to its effects on BP2324252627). Moreover, RAS blockade is well known to reduce CV and all-cause mortality and morbidity by preventing or reversing endothelial dysfunction and atherosclerosis282930313233). Thereby, RAS blockade reduces the risk of CV events and has been shown to be beneficial in patients at all stages of hypertension and in those with a risk of progression to atherosclerosis, target organ damage, and ultimately myocardial infarction, heart failure, stroke, or death.
Although we could not investigate the change of BP, atherosclerosis, and other conditions, we surmise that the benefit of RAS blockade in terms of preventing mortality may be explained by the above findings.
Consistent with previous studies2324252627), the incidence of all-cause and/or CV mortality in our study was significantly lower in the RAS blockade group than in the non-RAS blockade group. However, unlike previous renal function trials15182034353637), RAS blockade was not superior in terms of reducing the incidence of ESRD compared with non-RAS blockade. Concerning the renoprotective effect of RAS blockade, there are several papers showing different results. According to Rahman et al.38), there is no difference between lisinopril and chlorthalidone with respect to reducing the incidence of ESRD in hypertensive patients. Moreover, Lewis et al.39) showed that in patients with serum creatinine (sCr) level <1.0mg/dL, captopril was associated with only a 4% reduction in the risk of doubling of sCr level compared with that in the placebo group, whereas patients with baseline sCr >2.0mg/dL derived the greatest benefit from captopril, with a 74% reduction in the same endpoint. These findings suggested that the stage of kidney disease might be important in determining who would obtain benefit from RAS blockade. A meta-analysis by Jafar et al.40) also supported the observation that RAS blockade provides better renoprotection in individuals with heavier proteinuria. Owing to the design of the present study, we were unable to determine the baseline proteinuria or sCr level, which made it difficult to determine the specific degree of proteinuria and the severity of renal dysfunction. As a result, we could not delineate the effect of RAS blockade on the progression of ESRD in this study. However, only 6.5% of the patients enrolled in our study had a history of CKD(Table 1), which could be interpreted to mean that most patients had normal renal function at the start of the study. A longer follow-up duration is needed to reveal the effect of RAS blockade on the incidence of ESRD.
Although our findings were not consistent with previous results showing that the use of RAS blockade provides protection against adverse renal outcomes15203436394142), there are some other studies that failed to show the beneficial effects of RAS blockade on renal outcomes. In a prospective diabetes study on patients with hypertension and type 2 DM in the United Kingdom, the incidence of renal failure was not different between the captopril and atenolol groups43). Moreover, Suissa et al.44) reported that ACEi use did not seem to decrease the long-term risk of ESRD in patients with diabetes. In addition, combination treatments with ACEis and ARBs worsened the renal outcomes45). Moreover, a recent study by Oh et al.46) showed that habitual use of RAS blockade in predialysis patients with advanced CKD may have a detrimental effect on renal outcomes without improving all-cause mortality. We could not investigate how many patients had advanced CKD and how many patients had received combination treatment (ACEi and ARB), which is one of the limitations of the current study. Thus, our results on the renoprotective effects of RAS blockade should be carefully interpreted. In contrast, considering the above-mentioned previous studies, evidence supporting the renoprotective effects of RAS blockade might also need to be carefully reconsidered.
Furthermore, we also conducted the same analysis after stratifying patients into four groups according to RAS blockade treatment: ACEi or ARB users, ARB only users, ACEi only users, and non-users of RAS blockade. As seen in Supplementary Table 2, all-cause mortality and CV mortality were significantly reduced when the patients used ARB only or either ACEi or ARB compared with non-use of RAS blockade. However, we did not observe a protective effect against all-cause mortality and CV mortality in ACEi only users. Moreover, RAS blockade had no benefit with respect to the incidence of ESRD.
We investigated the number of annual prescriptions of RAS blockers (Supplementary Fig. 1). Although the number of prescriptions of ACEi only was decreased during the follow-up period, the number of prescriptions of ARB only was remarkably increased from 2007. The prominent increase in the prescription of ARBs cannot be precisely explained; however, the preference of physicians might have led to the above results. Considering such a skewed prescription between ACEis and ARBs, we surmise that these data are limited in indicating the protective effect of each of ACEis and ARBs on the clinical outcomes. The purpose of this study was to provide a comprehensive review of the effects of ACEis and ARBs in Korea. To identify factors associated with the effectiveness of commonly used antihypertensive drugs, further precise studies including patient-matching analysis and considering additional hypertensive drug use, frequency of drug use, and other factors will be needed in the future.
This study has several limitations. First, this was a retrospective cohort study. Thus, it was difficult to determine the effects of baseline variables on the final clinical outcomes. Second, we could not identify the exact causal effect of RAS blockade on the clinical benefit in patients because we did not investigate serial proteinuria levels during RAS blockade treatment. Third, we were unable to determine why some patients were not treated with RAS blockade because of the observational nature of the study. Fourth, as we could not measure sCr levels, we were unable to determine the detailed renal status at baseline. Despite these limitations, this large cohort study describes the frequency and effects of RAS blockade prescription in Korean hypertensive patients with proteinuria.





 XML Download
XML Download