

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Autoimmune hepatitis (AIH) is a chronic, relapsing disease with hepatocellular injury resulting from the loss of immune tolerance to liver antigens [12]. It often presents itself acutely in children and adolescents [34]. Currently, the basic treatment of AIH is prednisone and/or azathioprine. The treatment aims at obtaining full remission defined by disappearance of symptoms, lack of biochemical indices of inflammation, and lack of activity or presence of minimal activity in liver histology [456].
Pathogenesis of AIH requires genetic predisposition [7] and environmental triggers [8]. The nature of, and the relationship between the key autoimmune inflammatory pathways in AIH are not fully understood. The immunologic response mainly includes T-cell mediated mechanism, B-cell, macrophage and natural killer cells [9].
Macrophage migration inhibitory factor (MIF) is a pro-inflammatory cytokine that critically modulates key innate and adaptive immune pathways [9]. Its specific properties, including T-cell induction and counter-regulation of endogenous glucocorticoid activity [10], has been evaluated for its role in various autoimmune and inflammatory disorders [11].
Assis et al. [12] have evaluated MIF expression in adults with AIH and primary biliary cirrhosis. They concluded that MIF plays a key role in the pathogenesis of AIH. Two polymorphisms of clinical significance: -173 GC (rs755622) and −794 CATT5-8 (rs5844572) were tested in adult AIH, and were correlated to the disease severity and steroid responsiveness [13].
To the best of our knowledge, no previous studies considering MIF polymorphism have been performed in children with AIH. Our aim in the current study was to examine the MIF polymorphism, -173GC (rs755622), in pediatric AIH patients.
Go to : 
MATERIALS AND METHODS
This case-control study was conducted at the Hepatology Unit of Mansoura University Children's Hospital, Egypt. Patients were enrolled in a consecutive manner with definite diagnosis of AIH based on the simplified scoring system of AIH [14]. Age and sex matched control subjects were included. Parents or guardians of all patients signed informed consents allowing the patient's participation in the study. The study was approved by the Institutional Review Board of Mansoura faculty of medicine (code number: R/17.12.198) and followed the principles of Helsinki Declaration. Patients with chronic viral hepatitis, metabolic diseases, or co- morbidities were excluded from the study.
All patients included in the study were subjected to:
1. Thorough history and physical examination.
2. Laboratory work-up including serum bilirubin (total and direct), aspartate aminotransferase, alanine aminotransferase (ALT), prothrombin time, international normalization ratio, hemoglobin, and platelet count. Serological tests performed for the diagnosis included tests for total IgG, serum antinuclear antibody, anti-smooth muscle antibody, anti-liver kidney microsomal antibody.
3. Abdominal ultrasonography to evaluate liver echogenicity.
4. Percutaneous liver biopsy for necroinflammatory and fibrosis staging.
5. Clinical and laboratory follow up after the initiation of the standard treatment regimen for signs of remission+/or relapse.
Liver histology
All biopsy specimens were analyzed by an experienced pathologist blinded to the clinical and lab results of the patients. Specimens were examined for the diagnostic criteria of AIH, with the criteria being presence of portal lymphocytes and plasma cell infiltrate with interphase hepatitis. Necroinflammatory changes and fibrosis were graded according to the Ishak and METAVIR scoring systems [15].
Macrophage migration inhibitory factor genotyping
Single nucleotide polymorphism in MIF gene -173GC promoter region (rs755622) was genotyped by polymerase chain reaction (PCR)-based restriction fragment length polymorphismtechnique. DNA was isolated using Quick-DNA (Zymo research, Orange, CA, USA, Cat. No D3024).
Primers sequences used for DNA amplification were: Forward primer: (5´-ACT AAG AAA GAC CCG AGG C-3´), and Reverse primer: (5´-GGG GCA CGT TGG TGT TTA C-3´). For amplification of each sample, the following mix was prepared:12.5 μL of PCR Master mix (2X), 2 μL (10 pmoL) of forward primer, 2 μL (10 pmoL) of reverse primer, 5 μL (200 ng) of DNA template, and 3.5 μL of distilled water.
Thermal cycler (TECHNE, FTC3102D; Barloworld Scientific Ltd., Staffordshire, UK) was programmed according to the following amplification program: initial denaturation at 94°C for 5 minutes (One cycle), denaturation at 94°C for 45 seconds (35 cycles), annealing at 60°C for 45 seconds (35 cycles), extension at 70°C for 45 seconds (35 cycles),and final extension at 70°C for 7 minutes (One cycle). After amplification, the PCR products were fractionated on 2% agarose gel using 50 bp DNA ladder markers (Fermentas life science, Burlington, ON, Canada). A positive sharp band was identified in each well, and the size of the amplicon was 366 bp.
PCR-amplified DNA was digested with AluI in a 15 µL reaction solution containing 10 µL of PCR product, 1.5 µL of 10× buffer, and three units of AluI at 37°C for 10 minutes. Products were visualized by electrophoresis on a 2% agarose gel stained with ethidium bromide and photographed on an ultraviolet transilluminator. Two fragments (268 and 97 bp) were seen, where the G allele was present at position -173, and 3 fragments (206, 97, and 62 bp) were present, corresponding to the C allele (Fig. 1).
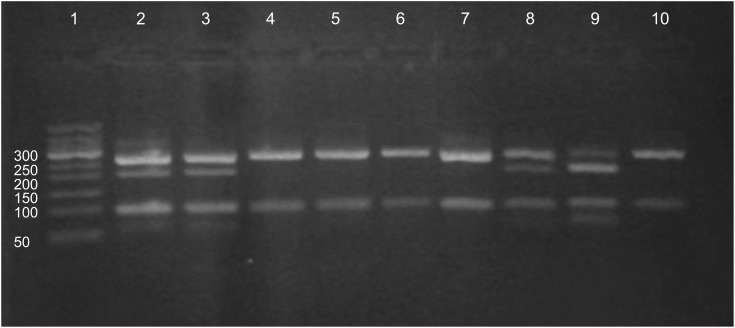 | Fig. 1Gel electrophoresis of polymerase chain reaction product. Lane 1 contains 50 bp DNA ladder. Lanes 4, 5, 6, 7, and 10 contain two bands of 268 and 97 bp that are indicators of GG genotype, lanes 2, 3, 8, and 9 contain four bands (268, 206, 97, and 62 bp) that represent GC genotype, while 3 bands (206, 97, and 62 bp) of CC genotype are absent.
|
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Co., Armonk, NY, USA), with the statistical significance set at p<0.05. Baseline characteristics were described using mean±SD for continuous parametric data, median and interquartile range (IQR) for nonparametric, and frequency (n%) for categorical data. The unpaired t-test and the paired-sample t-tests were applied for comparing continuous parametric variables, while Mann-Whitney test was applied for the non-parametric data. The Chi-squared or Fisher's exact probability test was applied for categorical data. Correlations were performed using Spearman's correlation.
Go to :
RESULTS
The study groups included 42 patients (27 females and 15 males) with definitive diagnosis of AIH. Their mean age (in years) was 13.5±2.7. Age and sex matched control group comprised 100 healthy children (mean age 12.6±2.8, p=0.090). Table 1 lists the results of distribution of polymorphism of MIF gene at -173GC between the patient and control groups. There was no statistically significant difference in the frequency of the genotypes GG and GC or G/C allele distribution in both patient and control groups (p=0.590). No CC genotype was detected in the both groups.
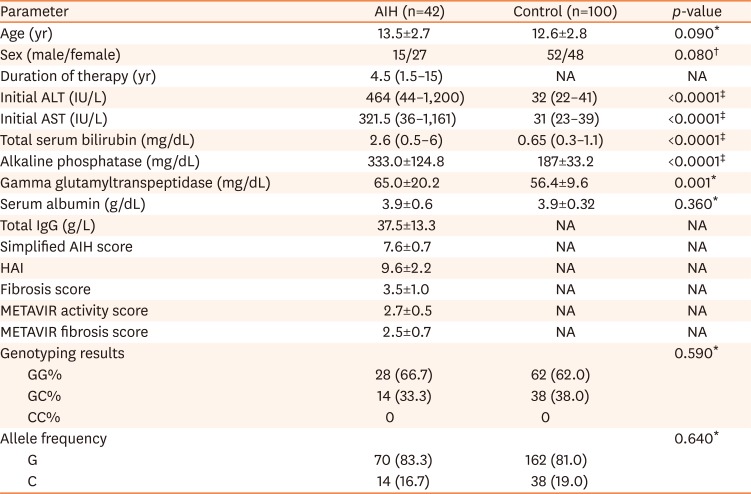
Table 1
Demographic, initial laboratory data, and MIF Gene -173GC polymorphism among patient and control groups
Values are presented as mean±standard deviation, number only, or median (range).
MIF: macrophage migration inhibitory factor, AIH: autoimmune hepatitis, ALT: alanine aminotransferase, AST: aspartate aminotransferase, HAI: histologic activity index, NA: not available.
*Independent sample t-test. †Chi-square test. ‡Mann-Whitney test.
![]()
Initial ALT levels at the time of presentation were significantly higher in the GC group (median and IQR were 743, 670) in comparison to the GG group (median and IQR were 375, 294, p=0.020). Other laboratory parameters showed no significant difference between the two groups. The different genotypes showed no significant differences regarding the scores for inflammation and fibrosis in the initial liver biopsy (Table 2).
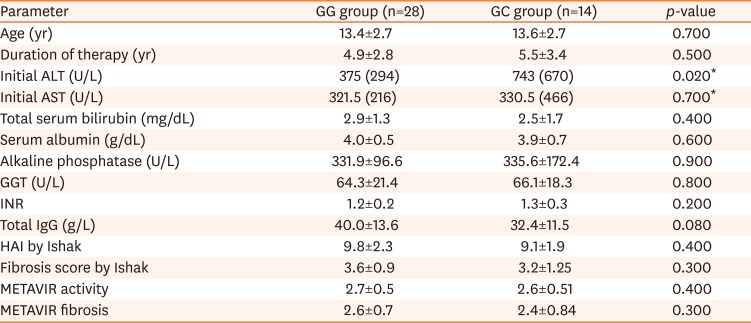
Table 2
Laboratory and histologic parameters of the patient group in different genotypes
Values are presented as mean±standard deviation or median (interquartile range).
ALT: alanine aminotransf, AST: aspartate aminotransferase, GGT: gammaglutamyltranspeptidase, INR: international normalization ratio, HAI: histologic activity index.
*Mann-Whitney test for ALT and AST, independent sample t-test for other parameters.
![]()
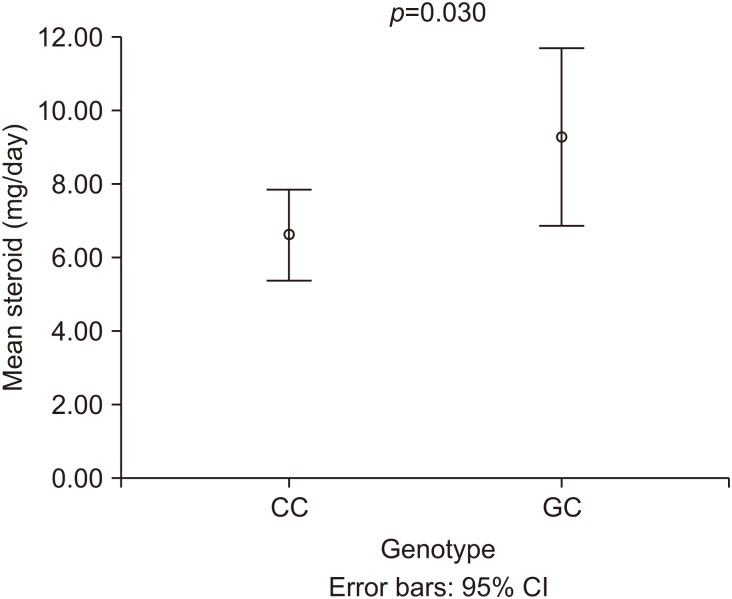
All patients were administered a combination therapy with systemic steroids (oral prednisolone) and azathioprine with gradual withdrawal of steroid guided by serum transaminases and IgG. The on-treatment ALT levels were higher in GC compared to the GG genotype group (median and IQR 38, 41 vs. 33, 11 respectively) but with no statistically significant difference (p=0.160). Mean prednisolone maintenance dose (in mg/d) was significantly higher in GC rather than the GG group (9.3±4.2 vs. 6.6±3.2, p=0.030) as in Fig. 2.
Out of the 42 patients, 18 had undergone a second liver biopsy for reassessment of the regression/progression of necroinflammatory and fibrosis criteria as compared to the initial biopsy performed at the time of diagnosis. The time interval between the two biopsies was 28.1±3.6 months (mean±SD). There was a significant regression in inflammation and fibrosis in the GG group in the 2nd biopsy. On the other hand, the regression of both necroinflammation and fibrosis in the GC group was not significant (Table 3).

Table 3
Comparison of necroinflammatory and fibrosis changes in the two genotypes of patients after receiving the AIH specific protocol
![]()
The clinical outcome and number of relapses defined by the increase of on-treatment ALT levels were compared in the two genotypic groups. Remission was observed in 20/28 (71.4%) of the GG group and in 4/14 (28.6%) of the GC group. The relapse was significantly higher in patients with GC genotype (10/14, 71.4%) than in the patients in the GG group (8/28, 28.6%) (Fisher's Exact test p=0.019). Spearman's correlation showed a significant correlation between the GC genotype and relapse (r=0.41, p=0.007).
Go to :
DISCUSSION
This is the first study of MIF gene -173GC polymorphism (rs755622) in AIH in pediatric patients. Although the MIF gene polymorphism was not statistically different between patients and the control group, the GC genotype showed significant higher values of initial ALT levels, and the C allele was correlated to relapse in the disease activity on therapy. On-treatment levels of ALT and mean steroid doses showed higher values in the GC group. The necroinflammation and fibrosis score were quite similar initially between both genotypic groups, but necroinflammatory and fibrosis regression was significant in the GG group on 2nd liver biopsy, while there was no significant change in the GC group for both necroinflammation and the fibrosis score.
MIF enhances both innate and adaptive immune systems and particularly promotes T-helper cell type 1 and the IFN-γ–mediated proinflammatory phenotype, which plays an essential role in AIH pathophysiology [9]. Animal studies have supported the potential role of MIF in T cell-induced inflammatory response in AIH, and the subsequent inhibition of T cell proliferation by the anti-MIF antibody which is in development pharmacologically to be used selectively in AIH with high MIF expression [16]. Moreover, MIF is now known to play an important role in a variety of autoimmune disorders including systemic lupus erythematosus [1718], rheumatoid arthritis [19], inflammatory bowel disease [20], and nephrotic syndrome [21]. MIF -173GC polymorphism was studied in different liver disorders such as biliary atresia [2223], nonalcoholic fatty liver disease [24], and hepatitis B viral infection [252627].
Frequency of MIF gene polymorphism has been studied in different populations. Results showed high frequencies of the C allele in Africans (43.4%) compared with Europeans (18.6%), East Asians (19.6%), mixed Americans (23.6%), and South Asians (21.8%) [23]. Studies in Egyptian population showed different results according to the differences in the nature of the disease of interest, but none was directed to AIH patients [232829]. In our study, the C allele frequency was 16.3% in patients vs. 19% in control group. The difference in frequency of genotypes GG and GC between patients and control was not significant (p=0.590). This non-significant difference was in agreement with the result obtained by Assis et al. [13] who found the frequency of GG, GC, CC to be 69.8%, 28.3%, 1.9%, respectively, in 53 adult AIH patients versus 60%, 40%, 0%, respectively, in the control group. We didn't find the CC genotype in our patients or in the control group and the reason for this could be small sample size.
MIF -173GC polymorphism was found to be correlated to disease severity and activity in many autoimmune disorders such as inflammatory bowel disease [20] and rheumatoid arthritis [30]. It can serve as an assessment tool of AIH disease severity. In our study, we found significant higher initial ALT levels in the GC group than the GG group (p=0.020). Similar results were found in the Japanese cohort of adult AIH patients, with non GG genotype, included in the study by Assis et al. [13]. In the aforementioned study, the authors also found higher on-treatment ALT levels in the American cohort of adult AIH patients who expressed a non-GG genotype in the same study. In our study, the on-treatment ALT was higher in the GC group but the difference was not significant (p=0.160). The mean steroid dose was significantly higher in GC group of our patients (p=0.030), which is in agreement with a previous study [13].
Moreover, relapse of AIH, which is defined by elevated liver transaminases on treatment, was significantly correlated to C allele. These findings may collectively encourage the potential role of MIF polymorphism in AIH activity and severity. MIF polymorphism in AIH may be a future candidate to tailor different treatment protocols and avoid the undue use of high doses of steroids, which are known to have significant adverse effects on the growth of children.
The unique finding in our study is the correlation of the C allele to the histological parameters in liver biopsy of our patients. Although there was no significant difference in the necroinflammation and fibrosis score in the two genotypic groups at time of the diagnosis and initial biopsy, the regression of histologic inflammatory score in response to treatment as observed on the second liver biopsy was significant in the GG (p<0.0001) but not in the GC group (p=0.090). This observation adds to the negative role of the C allele in hepatocyte inflammation in AIH. Additionally, the GG group showed a significant decline in the fibrosis score on 2nd liver biopsy (p=0.010). To the best of our knowledge, this is the first study that has tested the relation of histological changes in liver biopsy, in response to treatment, and with respect to MIF -173GC polymorphism in AIH patients.
Limitations of the current study include small sample size and lack of the study of MIF expression at the hepatocyte level. Further studies encompassing larger number of patients and a more longitudinal follow up are needed to explore the definitive role of MIF in pathophysiology, as well as regressionor progression of AIH notably in pediatric patients. This is particularly important, given the vulnerable nature of this age group and the effect of chronic AIH relapse that may compromise their adult life.
In conclusion, in the present study, the MIF -173GC polymorphism was associated with clinically significant markers of pediatric AIH including increased initial serum ALT levels and served as an effective predictor of necroinflammatory and fibrosis regression post immunosuppressive treatment. The prognostic value of MIF -173GC polymorphism still needs to be discovered as it will be of immeasurable value in the justification of AIH therapy.
Go to :
 XML Download
XML Download