

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Eosinophilic esophagitis (EoE) is an emerging disease in the field of pediatric gastroenterology. While evidence of this condition has been present since the 1960s, characterization of the disease did not occur until 1993 [1]. Kelly et al. [2] were the first to show that an elemental diet was effective in treating esophageal eosinophilia that was unresponsive to anti-reflux therapy. At the most basic level, EoE is characterized by the abnormal presence of eosinophils in the squamous epithelium of the esophagus. The diagnosis of EoE requires a combination of both clinical and pathologic findings, including the following: symptoms related to esophageal dysfunction, the presence of eosinophils on esophageal mucosal biopsy (≥15 eosinophils per high-power field), isolated eosinophilia in the esophagus, and the absence of any secondary causes [3]. Since the recognition of EoE in the 1990s, our understanding of this condition has improved but many questions remain unanswered, including the exact pathophysiology, characteristic histological findings, therapeutic endpoints, as well as biomarkers and molecular signatures that can aid in diagnosis [34].
Increased interest in more specific treatment guidelines has spurred research into the efficacy of current recommendations. Treatment options for this condition currently include medical therapies such as high-dose proton pump inhibitors (PPIs) [567], topical corticosteroids [89101112], and elimination diets such as elemental [13], empiric [14151617], and specific or directed elimination diets [15161819]. End points for treatment of EoE include improvements in both clinical symptoms as well as evidence of histologic response [316182021]. Treatment of EoE frequently requires a combination of both dietary and medical therapy. Two common dietary interventions include the dairy-free diet (DFD) [19] and the costly six-food elimination diet (SFED) [22]. The efficacies of these interventions were first demonstrated in 2006 and 2012, respectively, and they have shown continued success since their introduction [16182021]. Milk has been identified as the most common food trigger, followed by wheat [20]. Recent research has demonstrated the efficacy of additional diets such as the 4-food elimination diet, which has the advantage of covering major allergens while at the same time being less restrictive than SFED [16]. Given the multiple treatment strategies available, it has been difficult to validate a specific treatment protocol. Nowhere is this more apparent than in selecting a dietary elimination protocol for a patient, since in addition to nutrition, the clinician must consider patient lifestyle, adherence to therapy, and caregiver resources [322].
In this retrospective study, we aimed to evaluate treatment responses to DFD and SFED as initial therapies. We also sought to identify factors that may contribute to the success or failure of treatment, and specifically analyzed the following: treatment duration, age, sex, concurrent medical therapy, and objective findings on endoscopy and histology prior to and after therapy.
Go to : 
MATERIALS AND METHODS
We conducted a retrospective study of patients who had been treated for EoE (n=345). Retrospective and prospective data were entered into a Microsoft Access database by a single individual in the department of pediatric gastroenterology at Connecticut Children's Medical Center, Hartford, CT, USA. This database was approved by the institutional review board at Connecticut Children's Medical Center (IRB#: 15-046-CCMC). This database included demographic information, therapies (both dietary and medical), patient-reported compliance, endoscopy results, histology/biopsy results, and laboratory results. A single user abstracted the data elements listed below into an Excel spreadsheet. Potential confounders in this study included compliance and ancillary therapies such as medications. Patients were treated by various providers in our practice, and dietary therapies were determined based on both provider and patient preferences.
Patient demographics and clinical data
Patients included in the study were compared in terms of their demographic, endoscopic, and histological characteristics. Demographic characteristics included age, sex, and ethnicity/race. Clinical characteristics included concomitant medication usage (PPI's) and history of atopic disease (asthma, eczema, and seasonal allergies).
Gross endoscopic findings such as trachealization, furrowing, abscesses, exudates, specks, and erosions were noted both before and after elimination diets. We also examined pre- and post-treatment histologic characteristics, including peak eosinophils per high-power field (eos/hpf) on esophageal biopsy. Histologic examination was performed using 2–3 biopsies from both the proximal and distal esophagus.
Inclusion and exclusion criteria
The main study inclusion criterion was the diagnosis of EoE as per guidelines and consensus statements [34], mainly the presence of ≥15 eos/hpf on esophageal biopsy. Additional criteria included utilization of any of the aforementioned dietary therapies as first-line treatment, endoscopy interval ≥6 weeks, and no evidence of outright non-compliance (patients admitting to not following the diet). Exclusion criteria were age ≥21 years at the time of diagnosis, lack of follow-up, second biopsy obtained >6 months after initiation of therapy (usually because of non-adherence to therapy), or the presence of inflammatory bowel disease. None of the patients in this cohort had Eosinophilic gastritis or Helicobacter pylori infection.
Outcomes
The primary outcome was histological response, defined as a decrease in eos/hpf to <15 after dietary therapy. Patients noted to have ≥15 eos/hpf were defined as treatment failures. An advantage of this study is that a single pediatric pathologist at our institution reviewed the pathology sections. We chose to assess response histologically rather than based on symptoms because histological improvement is an objective finding in a retrospective study, whereas symptoms cannot be reliably assessed.
The secondary outcome was improvement of gross endoscopic appearance. Endoscopic improvement was based on the resolution of noted furrowing, trachealization, abscesses, exudates, specks, and erosions.
Outcomes were further analyzed by duration of therapy prior to repeat endoscopy and by age. Patients were categorized into 3 groups based on therapy duration: <10 weeks, 10–12 weeks, and >12 weeks. Similarly, patients were separated into 3 age groups: <6 years, 6–12 years, and >12 years.
Statistical analysis
Statistical analysis was performed using Prism Software version 6.0 (GraphPad Software Inc., La Jolla, CA, USA) and the R program (version 3.0.1; R Development Core Team, 2013; http://www.r-project.org) from the R foundation for statistical computing (http://www.R-project.org). Data were described using mean±standard error of the mean. We utilized the t-test for continuous variables to determine statistical significance when comparing 2 groups. We also used the χ2 method or contingency tables for categorical variables. We performed bivariate logistic and multivariate logistic regressions to identify predictors of response. Results were considered statistically significant at p<0.05.
Go to :
RESULTS
Demographic and clinical characteristics of study groups
A total of 345 patients with confirmed EoE were included in the database. Of these, 234 were treated with dietary elimination and 111 were treated mainly with topical steroids (n=78), directed elimination based on positive allergy tests (n=7), or other dietary elimination combinations such as milk/soy- or milk/soy/wheat-free diets (n=26). Of the 234 patients treated with DFD or SFED, 82 were excluded due to non-compliance or insufficient data. Examples of non-compliance included failure to adhere to diet, failure to obtain repeat biopsy, or failure to follow up. Thus, a total of 152 patients were included in this study (DFD=102 and SFED=50). Patient characteristics and demographics are presented in Table 1. Two notable findings were that older patients were more likely to be started on DFD vs. SFED (p=0.0070), and overall treatment duration prior to repeat endoscopy was significantly longer in the DFD group compared to the SFED group (p≤0.0001).
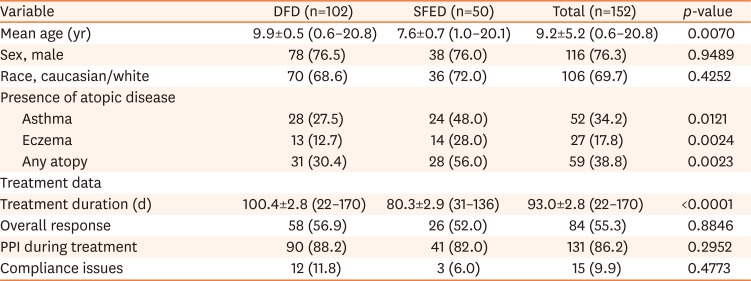
Table 1
Patient demographics and clinical characteristics
Values are presented as mean±standard error of the mean (range) or number (%).
DFD: dairy free diet, SFED: 6-food elimination diet, PPI: proton pump inhibitor.
p-values were computed using t-test for numerical variables and χ2 for categorical variables.
![]()
Histological findings
The average pre-treatment eosinophil count was 45.9±2.0 eos/hpf in the overall sample, 42.2±2.3 eos/hpf in the DFD group, and 52.4±4.2 eos/hpf in the SFED group (p=0.0069). The average post-treatment eosinophil counts were 21.3±1.9 eos/hpf in the overall sample, 20.6±2.3 in the DFD group, and 19.0±4.1 in the SFED group. Eosinophil counts decreased significantly after treatment in the overall sample, in the DFD group, and in the SFED group; p≤0.0001, p≤0.0001, and p≤0.0001, respectively (Table 2).
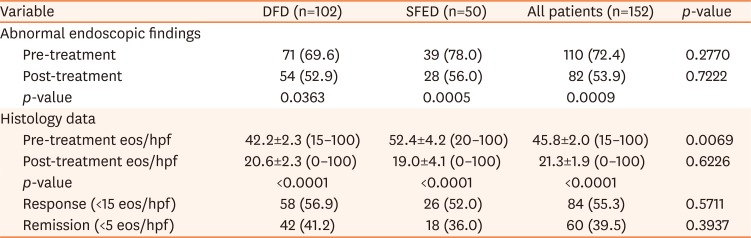
Table 2
Endoscopic and histologic data
Values are presented as number (%) or mean±standard error of the mean (range).
DFD: dairy free diet, SFED: 6-food elimination diet, eos/hpf: eosinophils per high-power field.
p-values were computed using t-test for numerical variables and χ2 for categorical variables.
![]()
Endoscopic findings
In the overall patient sample, abnormal endoscopic findings were observed in 72.4% (110/152) of patients before treatment, and persisted in 53.9% (82/152) of patients after treatment. In the DFD and SFED groups, pre-treatment abnormalities were identified in 69.6% (71/102) and 78.0% (39/50) of patients, respectively, and post-treatment abnormalities were noted in 52.9% (54/102) and 56.0% (28/50) of patients, respectively. There were significant improvements in post-treatment endoscopic findings in the overall sample, in the DFD group, and in the SFED group; p=0.0009, p=0.0363, and p=0.0005, respectively (Table 2).
Response to treatment with regard to treatment duration and patient age
The response across all treatment groups was 55.3% (84/152). There was no significant difference in treatment response when DFD 56.9% (58/102) and SFED 52.0% (26/50) were used as primary therapies (p=0.8846). Among responders to DFD, SFED, or either, there were no significant differences when comparing patient groups defined by treatment duration (<10 weeks, 10–12 weeks, and >12 weeks) or by age (<6 years, 6–12 years, and >12 years) (Table 3).

Table 3
Response based on treatment duration and patient age
Values are presented as number (%).
DFD: dairy free diet, SFED: 6-food elimination diet.
p-values were computed using χ2 for categorical variables.
![]()
In the DFD group (n=102), the therapy duration was <10 weeks in 11 patients, 10–12 weeks in 22 patients, and >12 weeks in 69 patients; the respective response rates in these 3 groups were 81.8% (9/11), 50.0% (11/22), and 55.1% (38/69). In the SFED group (n=50), the therapy duration was <10 weeks in 16 patients, 10-12 weeks in 14 patients, and >12 weeks in 20 patients; the respective response rates in these 3 groups were 68.8% (11/16), 50.0% (7/14), and 40.0% (8/20).
The response rate to DFD, based on age, was 59.3% (16/27) for age <6 years, 42.9% (15/35) for age 6–12 years, and 67.5% (27/40) for age >12 years. The response rate to SFED was 36.4% (8/22) for age <6 years, 58.8% (10/17) for age 6–12 years, and 72.7% (8/11) for age >12 years.
Treatment response in the presence or absence of atopy
Patients treated with SFED were significantly more likely to have asthma (p=0.0121), eczema (p=0.0024), or any atopy (p=0.0023) compared to patients treated with DFD (Table 1). The presence or absence of atopy was not significantly associated with treatment success, either in the overall patient sample or in patients categorized by response to DFD and SFED (Table 4).

Table 4
Response based on other patient clinical characteristics and treatments
Values are presented as number (%).
PPI: proton pump inhibitor, DFD: dairy free diet, SFED: 6-food elimination diet.
p-values were computed using χ2 for categorical variables.
![]()
Treatment response with or without concomitant PPI therapy
Of the 152 patients on DFD or SFED, 131 (86.2%) underwent concurrent PPI therapy (Table 1). Treatment success was not significantly associated with PPI therapy in the overall patient sample (Table 4). However, patients treated with both DFD and concurrent PPI therapy (88%) had a significantly higher rate of treatment success than those on DFD alone (p=0.0177). This was confirmed with bivariate logistic regression analysis (p=0.0491) but not in the multivariate logistic regression (Table 5). This difference was not observed in patients who received SFED with or without PPI therapy. None of our patients were treated with what is considered high dose PPI therapy while on dietary therapy.

Table 5
Determinants of resolution/remission after treatment
Bivariate and multivariate regression model demonstrating determinants of response to treatment with outcome of resolution/remission.
*p-value <0.05 (statistically significant).
![]()
Go to :
DISCUSSION
In this retrospective study, we sought to evaluate the efficacy of DFD and SFED as first-line therapies for the treatment of EoE in our practice. This was not intended to be a head-to-head comparison but rather a comparison of first line options. Treatment with DFD and SFED as first-line therapies resulted in responses in 57% and 52% of children, respectively. These response rates were not surprising given the results of previous studies. In a retrospective study, Kagalwalla et al. [19] showed that the response to DFD was 65% when used as the initial therapy for EoE treatment. In a second retrospective study, this same group found that 75% of patients responded to SFED [18]. In a meta-regression analysis, Cotton et al. [23] showed an overall response rate of 69% to SFED (95% prediction limits 31.9–91.4%).
While multiple therapies have been shown to be effective for EoE, optimal treatment protocols remain elusive due to the need to tailor treatment to individual patients. We anticipated that patients with longer intervals between endoscopies would have increased response rates due to decreased antigen loads. However, as noted above, there was no significant difference between treatment groups with regards to treatment duration; patients treated <10 weeks had the highest response rate, but this finding was not statistically significant. Given this finding, decisions on the duration of therapy prior to repeat endoscopy should be based on a combination of factors, including patient adherence and the complexity of dietary therapy. We suspect that the longer the endoscopy interval, the more likely it is that the patient will become non-adherent, as seen in those who underwent repeat endoscopy after very long intervals (>6 months) and were eventually excluded. Most studies on dietary management of EoE performed endoscopies at intervals of 6–8 weeks. The consensus statements from 2007 and 2011 recommended treatment of 6–12 weeks (depending on the treatment) between endoscopies [324]. The 2018 AGREE conference was not clear nor specific with regards to the duration between endoscopies [3]. Our practice is to do endoscopies at intervals of 8–12 weeks to minimize the number of endoscopies and anesthesia done in a short period of time.
Additionally, and surprisingly, response rates in the treatment groups did not differ with respect to age. We hypothesized that since parents would be more likely to manage younger patients' diets, these patients might have better compliance and thus, higher response rates. In fact, there was no significant difference between age groups, but surprisingly, older patients had numerically higher response rates. Additionally, older patients were more likely to be started on DFD rather than SFED (p=0.0070). This is generally done to minimize the difficulties that teenagers may face with dietary restrictions and to improve compliance.
The majority of patients (85%) underwent concomitant PPI therapy with the dietary elimination. Patients treated with both DFD and PPI therapy fared better than those who did not receive PPI therapy (p=0.0177). This was confirmed with bivariate logistic regression analysis (Table 5). There was no difference in the SFED group with respect to concomitant PPI therapy. PPIs have been shown to significantly inhibit IL-4–stimulated eotaxin-3 expression in EoE esophageal cells and to block STAT6 binding to the eotaxin-3 promoter [25]. Additionally, PPIs might have eosinophil-reducing effects independent of their influence on acid reflux, and response to PPIs might not distinguish EoE from gastroesophageal reflux disease [26]. Therefore, it is not surprising that patients who underwent an elimination diet with concomitant PPI therapy responded more favorably.
Since an association between atopic diseases and EoE has previously been demonstrated [272829], we compared treatment outcomes between those with and without evidence of atopic disease. There was no significant association, either in the overall sample or in treatment subgroups (Table 4). While atopy is helpful in the diagnosis of EoE, it does not appear to be applicable as a predictor of treatment response.
Significant improvement of gross endoscopic appearance was noted in the overall sample as well as in treatment subgroups (Table 2). It would have been optimal to compare these results with associated symptomatology, but the database did not include sufficient data on symptoms.
This study has several strengths. It reflects the comprehensive nature of real-life practice at a single major children's healthcare facility. The sample size is one of the largest in any pediatric or adult studies. While treatment approaches vary from practice to practice, we report on a single department experience where clinical decisions were similar among the providers. Retrospective and prospective data input was performed by a single individual, which decreased variability in reported patient profiles. Furthermore, an advantage of the database is that the same information was available for all patients.
A major exclusion criterion for this study was compliance with dietary therapy; while the database provided evidence on many occasions, these were restricted to subjective observations and patient admittance. As in any study, compliance is difficult to measure. In multiple instances, issues with compliance did not become apparent until the follow-up endoscopy, which voided the usefulness of the follow-up biopsy.
One of the weaknesses of this study was the lack of uniformity in treatment courses between patients. Despite having limited therapeutic options for EoE, general pediatric and adult practices across the country vary in their treatment approaches. On secondary analysis of our data it was noted that a significant number of patients (52%) started on DFD and a PPI had no prior PPI exposure. This makes it difficult to interpret response rates as this subset of patients were exposed to two recognized forms of treatment for EoE simultaneously. However, we would like to highlight the fact that none of our patients received what is considered to be high dose PPI therapy before or during treatment with dietary therapy. Standardized dosing was also difficult to identify as patients were noted to be on multiple formulations of PPI (i.e. omeprazole, lansoprazole) which have variable dosing based on age and weight. Lastly, our database did not include actual dosing of PPI therapy. Given this, PPI administration in these cases should be viewed as an adjunctive therapy vs dual therapy.
A major area of future research is the development of stepwise treatment protocols. Developing and validating a step-up treatment approach to EoE, in contrast to the commonly used top-down methods, would be a valuable tool for practitioners. We believe that starting with a dairy free diet as first line therapy, with or without PPI, is warranted. This should be followed by a 4- or 6-food elimination diet or oral topical steroids. Optimization of such a protocol could lead to decreased time to remission along with potential decreases in endoscopic procedures. These diets should be tried in addition to directed elimination diets based on allergy testing in patients with multiple food allergies. In these patients, it is not unreasonable to proceed with SFED or even more restrictive diets such as a hypoallergenic diet or an elemental diet if necessary. Further prospective studies are warranted to identify the most effective treatment approach.
Go to :
CONCLUSION
DFD is an effective initial therapy for EoE and should be attempted before more extensive and costly elimination diets [22]. This has the advantage of eliminating one of the most common offending agents in EoE while remaining minimally restrictive. High-dose PPI therapy remains an important treatment option for EoE, however, adverse effects with long term use of PPI's has raised concerns. Concomitant use of PPIs with dietary therapy is also advised until a repeat endoscopy is performed. We believe that this warrants further studies and a prospective trial to evaluate a step-up approach to treating EoE in children and adults.
Go to :
 XML Download
XML Download