

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Supplemental ultrasound (US) is an effective imaging method to detect mammography-negative, early-stage invasive breast cancer in women with dense breasts (123). However, performing supplemental whole-breast US with hand-held devices has some limitations. Hand-held US system (HHUS) screening is operator-dependent and time-consuming, and records only representative images of the detected lesions that cannot be easily compared with the results of past examinations (4). The automated breast US system (ABUS) has capability to overcome some of those limitations by allowing structured image acquisition, which enables whole-breast evaluation with multiplanar reformation (MPR) and temporal comparisons (5). Reports have indicated that ABUS devices have similar detection ability for mammography-negative invasive breast cancers as compared to HHUS (678910).
Although the large-transducer breast scanning system of ABUS can cover larger areas of the breasts, the examination is performed on patients in supine position with movement of the transducer in a straight line; therefore, such scans require breast compression, and single scan is not enough to cover the whole breasts (11). The number of scan volume depends on the breast size, especially, for large breasts, scan volume of five per breast is required (12). Reports have indicated the performance levels of four-view technique with coverage of the upper-outer, lower-outer, lower-inner, and upper-inner breast regions (11), and conventional three-view scanning technique according to manufacturers' guidelines (13141516171819).
Scanning and reading times vary according to the number of views; reduction of the number of views allows more rapid screening, but diagnostic ability should be maintained the to the level achieved by a minimum of three scanning views. For women with small breasts, scanning the entire breast with two scanning views may be feasible, and can reduce the scan time and discomfort due to compression. However, an optimal, operator-independent scanning technique with coverage of the entire breast has not been well investigated.
This study aimed to compare the breast coverage between the ABUS two-view scan technique (2-VST) and the conventional three-view scan technique (3-VST), and evaluate the diagnostic performance of both techniques for breast cancer detection in women with small breasts.
MATERIALS AND METHODS
Participants
This prospective study was approved by our Institutional Review Board, and written informed consent was obtained from all subjects. From March 2016 to May 2017, ABUS and HHUS was offered to asymptomatic women with small breasts who wanted whole-breast screening US or were referred for US examination for further evaluation of US-detected lesions. Small breasts were characterized based on a bra cup size A or less and cup diameter of 20 cm or less. For comparison of breast-scan coverage and evaluation of diagnostic performance, women scheduled for US for diagnostic purpose and those referred to our breast clinic with abnormalities detected by US screening at another hospital, were included. Women with breast implants, previous breast surgery, pregnant women, and breastfeeding women were excluded.
ABUS Image Acquisition and Interpretation
ABUS was performed by two technologists (minimum 3 years' experience with the technique, each). A three-dimensional (3D) ABUS system (Invenia ABUS, GE Healthcare, Sunnyvale, CA, USA) was used, which consists of Invenia ABUS Scan Station with wide field-of-view transducer (Reverse Curve™ ultra-broadband transducer, GE Healthcare; frequency range, 6–15 MHz; aperture length, 15.4 cm; transducer bandwidth, 85%; imaging depth, up to 5.0 cm) and Invenia ABUS workstation. The volume data were acquired at 0.5-mm slice interval, and the images were reconstructed in coronal plane.
Details of the scanning technique are as follows: anteroposterior (AP), lateral (LAT), and medial (MED) views were acquired for 3-VST. For the AP views, the nipple was centered, and the views of the central breast tissue and nipple were acquired. For the LAT views, the lateral and superior breast tissue including the axillary tail were acquired, with the nipple in the inferior-medial corner. For the MED views, the medial and inferior tissue including the inframammary folds were acquired, with the nipple in the superior-lateral corner. Conversely, the scanning range of 2-VST was comprised of the modified AP and modified LAT views. For the modified AP views, the central breast tissue including the nipple and the medial and inferior-medial portions of the breast were scanned. For the modified LAT views, the central tissue including the nipple and the lateral and superior-lateral breasts were scanned. The technologists were instructed not to exclude any of the breast tissue during the scanning procedure: LAT or modified LAT views, for coverage of the most lateral fatty tissue located at the outer aspect of the fibroglandular tissue; MED or modified AP views, for coverage of the most medial fatty tissue at the inner aspect of the fibroglandular tissue. Combined 2-VST and 3-VST was applied in all patients by simultaneous 2-VST at the right breast and 3-VST at the left breast, and the reverse order of scan alternatively in the participants according to enrollment sequence with blinding of clinical information.
Subsequently, the ABUS images acquired were evaluated on the Invenia ABUS workstation by one of six radiologists (5–15 years' experience in breast imaging) who was blinded to the clinical information and results of HHUS but not to the recent mammographic and previous HHUS information. Radiologists were instructed to document each lesion with a marker on the representative images, estimate the maximal lesion diameter in the transverse plane, and record the clock-face position and distance from the nipple. ABUS data were interpreted by the same radiologists using the breast imaging reporting and data system (BI-RADS) classification, and each lesion was assigned a BI-RADS assessment category. The following lesion characteristics were recorded: lesion type (mass, mass with calcifications, or calcifications only); shape (oval, round, or irregular); margin (circumscribed or not circumscribed); echogenicity (hypoechoic, isoechoic, or hyperechoic). The final BI-RADS category of the breast was determined according to the highest BI-RADS assessment category among the lesions.
HHUS Evaluation and Result Integration
After acquisition of the ABUS scan, HHUS was performed in all participants for clinical purposes. HHUS images were obtained by one of the six radiologists who was not involved in the interpretation of ABUS scan, using one of two scanner types (Aixplorer, Supersonic Imagine, Aix-en-Provence, France; HI VISION Ascendus, Hitachi Medical, Tokyo, Japan) equipped with a 6–14 MHz or 5–10 MHz linear transducer. The radiologist was blinded to the recent HHUS results, but allowed access to recent mammographic information and results of previous HHUS when available.
For each lesion detected, the clock-face position, distance from the nipple, and maximal diameter were recorded. Finally, the findings and reports of ABUS and HHUS examinations were compared and integrated by two radiologists (5 and 15 years' experience in breast imaging, respectively) who had not participated in the HHUS and ABUS image interpretation. In case of discrepancy between ABUS and HHUS, HHUS was reevaluated for the suspicious findings of ABUS to confirm the final decision for clinical purposes.
Breast Coverage and Scan Time Evaluation
To evaluate whether the whole breasts were properly covered by both 2-VST and 3-VST of ABUS, the scan views and areas were retrospectively analyzed by two breast radiologists. Proper coverage of the breast tissue was defined as an absence of abrupt cutoff of the fibroglandular tissue at the margin of each view, and inclusion of the fatty tissue at the lateral margin on LAT or modified LAT views and the medial margin on the MED or modified AP views. Additionally, HHUS-detected lesions were considered as the landmarks in the ABUS scans, and visualization of those on the scan views of ABUS was evaluated.
The scan times for ABUS 2-VST and 3-VST were retrospectively retrieved from the workstation, and evaluated according to each scan technique.
Data and Statistical Analysis
For the diagnostic performances, the findings and final BI-RADS categories of ABUS in each breast were collected; biopsy or at least 1 year of follow-up was used as the reference standard, and tissue diagnosis of ductal carcinoma in situ, or invasive cancer within 1 year after breast US, were considered disease-positive.
BI-RADS category 4A or higher was considered as a positive test result for malignancy; in addition, the sensitivities, specificities, number of scan views with proper breast coverage, and comparison of the HHUS lesion's visibility between 2-VST and 3-VST was performed with generalized estimating equations applied for within-subject correlation. The characteristics of malignant or benign lesions in each scan group were compared using Fisher's exact tests and Mann-Whitney U tests for categorical and continuous variables, respectively. Independent t test was used to compare the scan times between 2-VST and 3-VST.
Statistical analyses were performed using SAS (version 9.4; SAS Institute Inc., Cary, NC, USA) and SPSS (version 25 for Windows; IBM Corp., Armonk, NY, USA). Two-tailed p value of < 0.05 was considered as statistical significance.
RESULTS
Participants and Lesions
Of the 160 patients screened, 24 were unavailable for follow-up with additional biopsy or imaging studies. Finally, 272 breasts of 136 women (mean age, 44.4 years; range, 29–81 years) were included in the study. All the participants were asymptomatic. Indications for US included routine screening (n = 118), and diagnostic workup for abnormalities (n = 18). Of the 136 participants, data of previous mammograms were available in 90 women. The breast tissue composition was as follows: almost entirely fatty in two individuals, with scattered areas of fibroglandular density in eight women, heterogeneously dense breasts in 48 women, and extremely dense breasts in 32 women. In total, 64 previous HHUS examinations were available for review.
The characteristics of the lesions according to the scan techniques are summarized in Table 1. For 27 lesions in 27 breasts, histologic confirmation was done by surgical excision (n = 20) or US-guided core-needle biopsy (n = 7). In the 2-VST group, eight malignant lesions (Fig. 1) and 128 normal or benign cases including three biopsy-proven lesions were observed; whereas, in the 3-VST group, ten malignant lesions and 126 normal or benign cases, including six biopsy-proven lesions, were observed. Of the malignant lesions, breast-conserving surgery was performed for 10 lesions, and mastectomy for the remaining eight lesions, respectively. For atypical ductal hyperplasia and lobular carcinoma in situ lesions, wide excision was performed, which confirmed the same pathology.
In all participants, immediate concurrent HHUS and follow-up HHUS examination (mean follow-up time, 727.9 days; range, 306–1043 days) was performed. Overall, discrepancy between ABUS and HHUS was observed in four cases (mean size, 7.25 mm; range, 4–10 mm). One lesion of category 4A on ABUS with 3-VST was considered as a pseudo lesion on concurrent HHUS. For the two lesions of category 4A and 4B on ABUS with 2-VST and one lesion of category 4A on ABUS with 3-VST, benign features were observed on concurrent HHUS, and hence, the lesions were downgraded to category 3; follow-up HHUS was performed for those lesions, and no interval change was noted during the follow-up period (range, 677–1022 days). In addition, lesion stability was confirmed for the other lesions of benign or probably benign categories, and the benign category was confirmed through biopsy during the follow-up period.
Image Findings on ABUS
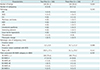
The mean size of the eight malignant lesions was 18.0 ± 10.5 mm in the 2-VST group, and 18.1 ± 7.9 mm for the 10 malignant lesions in the 3-VST group (p = 0.688). The mean size of the benign lesions was 7.0 ± 4.6 mm in the 2-VST group (n = 51), and 7.2 ± 4.7 mm in the 3-VST group (n = 52) (p = 0.852). Imaging characteristics of the malignant and benign lesions visualized on ABUS are summarized in Table 2.
Breast Coverage and Scan Time
Proper coverage, defined as absence of abrupt cutoff of the fibroglandular tissue at the margin of view and including the fatty tissue at the lateral or medial margin of each view, was attained in 94.1% and 91.9% of 2-VST and 3-VST, respectively. Unsatisfactory breast coverage was more frequent in 3-VST, without statistical significance (p = 0.318); however, all 105 HHUS-detected lesions (52 lesions on 2-VST and 53 lesions on 3-VST) were visualized through ABUS regardless of scan technique (Table 3). The mean scan time of 2-VST and 3-VST was 202.6 ± 64.4 seconds and 315.8 ± 109.3 seconds, respectively.
Diagnostic Performance
With regard to positivity for malignancy based on BI-RADS category 4A or higher, the sensitivity and specificity of ABUS with 2-VST was 100% (8/8) and 97.7% (125/128), respectively, and that of 3-VST was 100% (10/10) and 95.2% (120/126), respectively, with no significant differences of the values between scan techniques (p > 0.999, sensitivity; p = 0.306, specificity) (Table 3). All of the malignant lesions were detected on ABUS, and no false-negative cases were obtained in either scan group. With regard to false-positive cases, a total of nine benign lesions (3.3%) were assessed as BI-RADS category 4A or higher through ABUS; of those, three lesions were identified with 2-VST, and six lesions, with 3-VST. The most frequent US features of these lesions were as follows: mass type (9/9), irregular shape (7/9), circumscribed margin (6/9), and low echogenicity (8/9).
DISCUSSION
To the best of our knowledge, this is the first study to comparatively evaluate the diagnostic performance between 2-VST of ABUS and conventional 3-VST, for breast cancer detection in women with small breasts. The results revealed similar diagnostic performance between 2-VST and 3-VST with high sensitivity and specificity (100% vs. 100%; 97.7% vs. 95.2%, respectively), and no significant difference of the scan coverage between the two scan techniques.
In general, 3-VST including the AP, LAT, and MED volumes are commonly used, and sufficient for the whole-breast scan excluding the axilla. However, ABUS imaging should be performed with selection of suitable settings according to the breast size of the individual patient (1215161718); for coverage of the entire field of interest, more than three scans may be required in patients with larger breasts, whereas two-volume scans (medial and lateral) in those with the breasts of bra cup size A or B (1314). An et al. (19) reported that ABUS achieved reduced diagnostic performance for detection of peripherally situated lesions, particularly in the large breasts, which highlights the importance of breast coverage to prevent misdiagnosis of cancer. Adjustment of scan technique according to the breast size should aim at capture of the entire breast in the acquired image, and maintenance of high image quality. In our study, 2-VST of ABUS provided adequate coverage of the entire breast tissue in women with small breasts, and achieved reduction of the total scan time.
In ABUS scans with multiple volumes, each volume scan automatically generates sequential transverse images at coronal and sagittal planes using MPR. The system allows radiologists to view the images manually in multiple orientations. Moreover, ABUS can generate coronal image planes, while HHUS lacks this feature. The coronal view allows rapid and comprehensive analysis of the whole breast (13152021). Previous reports indicated that augmentation of the transverse plane views with 3D coronal views improves differentiation of the breast lesions based on superior visualization of spiculation and retraction patterns in the coronal reconstruction (22).
Supplemental screening with ABUS detected 1.9 more cancers per 1000 screens in mammographically negative, asymptomatic women, but resulted in a high rate of false positives (6). Our study cohort comprised a majority of patients with cancer, and the results may not reflect the actual screening performance; nevertheless, the imaging approach achieved higher sensitivities and specificities regardless of the scan number. Radiologists using ABUS should consider the possibility of both false positives and false negatives. False negatives are partly due to interpretation and oversight errors by the reporting radiologist, who may miss small invasive cancers when reviewing many images (5). Multi-view images can reduce the incidence of false positives through visualization of the detected lesions in more than one view, but an increase of other false-positive interpretations could occur. Therefore, more imaging data may not lead to consistent improvement of the diagnostic performance; contrarily, the increased workload may induce early fatigue in the radiologists interpreting the images.
This study has several limitations. First, it is a single center study with a relatively small number of patients. Both screening and diagnostic examinations were included, and the final study population comprised a majority number of patients with cancer; hence, our results may not accurately reflect those of a screening population. Nevertheless, to compare the detection ability of 2-VST and 3-VST with sufficient statistical power, substantial numbers of cancer cases were needed. Second, 2-VST and 3-VST were randomly applied at either of the patient's breasts. Since the number of benign and malignant lesions can differ according to the scan technique, and due to technologists' preference in scan techniques, selection bias may have occurred. Third, the diagnostic performance was compared between 2-VST and 3-VST; however, the total time for reading was not calculated, since it was not the primary purpose of our study. Finally, proper coverage was assessed by image evaluation for the anatomical structures and lesion inclusion, which is not an objective method. Currently, there is no automatic or objective quality control or assessment system for coverage in ABUS. Studies are needed to develop quality control system of ABUS similar to that used in mammography.
In conclusion, the breast coverage in 2-VST was comparable to that in 3-VST. In women with small breasts, ABUS with 2-VST achieved similar diagnostic performance for breast cancer detection as conventional 3-VST. Further research is required to establish the optimal image acquisition technique for ABUS in clinical settings.



 XML Download
XML Download