

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Treating constipation in children is a common and frustrating problem. Constipation comprises an estimated 3-5% of visits to pediatricians and 25% of visits to pediatric gastroenterologists [1]. Constipation is a symptom, not a disease. It can be caused by various organic diseases such as spina bifida, cerebral palsy, intestinal pseudo-obstruction, Hirschsprung's disease, and anal stenosis. However, the most common cause of constipation in children is a chronic functional condition without an organic cause. Chronic constipation affects children's well-being and is correlated with a decreased quality of life. However, constipation is underestimated compared to its severity [234].
Depending on constipation severity, several factors can be considered, such as fecal soiling, decreased bowel frequency, effective medicine type and dose, and colon transit time (CTT) test results. In the CTT test, a prolonged CTT value indicates severe constipation. Children with abnormal CTT test results respond poorly to medication compared to those with normal CTT test results [5]. PEG 4000 (Forlax; Beaufour Ipsen Pharm., Paris, France) has superior efficacy to lactulose (Duphalac syrup; JW Pharmaceutical, Seoul, Korea) for the treatment of childhood constipation [6]. The frequency of PEG 4000 use was higher in the fecal-soiling group than in the non-fecal-soiling group [7].
We hypothesize that both infrequent bowel movements (less than once a week) and fecal soiling represent advanced chronic functional constipation in children. In this study, we compared the clinical and demographic features, diagnostic findings including CTT test, and therapeutic drugs and doses between 2 groups of severely constipated children: one with bowel frequency less than once a week and the other with fecal soiling.
Go to : 
MATERIALS AND METHODS
From January 2008 to August 2018 at the Konkuk University Medical Center (Seoul, Korea), 333 children who met the Rome III (2008–2016.5) or the Rome IV (2016.6–) criteria for constipation with symptoms of infrequent bowel movement (more than 7 days, ≤1/week) or fecal soiling were enrolled in this study. Organic diseases, such as anal stenosis, Hirschsprung's disease, and spinal schwannoma, were excluded by digital rectal examination, barium enema, anorectal manometry, and magnetic resonance imaging. We initially classified the children into 3 groups: infrequent bowel movement without fecal soiling (G3-a), infrequent bowel movement with fecal soiling (G3-b), and fecal soiling only (G3-c). We also divided the children into 2 groups: fecal soiling (G2-b) or not (G2-a). Data including clinical characteristics, CTT test results, and medications were retrospectively collected and analyzed from medical records along with a defecation diary that included bowel movement frequency, stool consistency, soiling, and amount of fluid intake per day. Of the 333 children, 192 underwent CTT testing and 60 were excluded based on the following criteria: (1) abnormal CTT test result (n=52); (2) acute illness during the CTT test (n=2); and (3) underlying disease, including failure of the puborectalis muscle to relax (n=5) on fluoroscopic defecography and imperforate anus (n=1). Thus, the CTT test results of 132 children were compared. The CTT test was performed according to the Metcalf protocol [8], with caution for food, medicine, and acute illness. Based on the medical records and defecation diary, we judged the validity of the CTT test and data.
The initial maintenance dose of laxative was defined as the amount that resulted in a comfortable bowel movement with soft or loose stool for more than 5 days a week for more than 2 months without a change in dose based on the defecation diary.
The results are expressed as median and interquartile range (IQR) values for age. Patient sex and laxative type are described as number and percentage of children. The data were analyzed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The data were not normally distributed (Kolmogorov-Smirnov test, Shapiro-Wilk test, and Q-Q plot), and the results are expressed as median values and IQR. The Wilcoxon rank-sum test, Kruskal-Wallis test, Chi-square test, and Fisher's exact test were used for the statistical analysis. This study got an exemption from the institutional review board of Konkuk University Medical Center (IRB No. KUMC 201904013).
Go to :
RESULTS
Of the 333 children, 189 were male. In the infrequent bowel movement without fecal soiling group (G3-a, n=170), there were 82 (48.2%) male patients. In the infrequent bowel movement with fecal soiling group (G3-b, n=62), there were 39 (62.9%) males. In the fecal soiling group (G3-c, n=101), there were 68 (67.3%) males (p=0.0030). The frequency of bowel movement ranged from once a week to once every 38 days in children with infrequent bowel movement. Patient age ranged from 1 month to 18 years (1 month to 18 years in G3-a, 15 months to 16 years in G3-b, and 26 months to 16 years in G3-c).
The median age and IQR were 33 (45) months in the G3-a group, 54 (40) months in the G3-b group, and 73 (48) months in the G3-c group (p<0.0001). Age at onset (IQR) was 7 (10) months in the G3-a group, 12 (24) months in the G3-b group, and 18 (18) months in the G3-c group (p=0.0219). Symptom duration (IQR) was 12 (18) months in the G3-a group, 24 (12) months in the G3-b group, and 24 (24) months in the G3-c group (p=0.0148). The PEG 4000 was used in 103 (60.6%) in the G3-a group, 60 (96.8%) in the G3-b group, and 84 (83.2%) in the G3-c group (p<0.0001). PEG 4000 was prescribed more frequently than lactulose in all 3 groups (Table 1).

Table 1
Patient demographic and clinical characteristics by study group
Values are presented as median (Interquartile range) or number (%).
G3-a: infrequent bowel movement without fecal soiling group, G3-b: infrequent bowel movement with fecal soiling group, G3-c: fecal soiling group.
![]()
To compare the maintenance doses of the laxatives, each group was further subdivided into 3 subgroups according to age. The median maintenance dose of PEG 4000 was 0.67 g/kg/day (<8 years), 0.56 g/kg/day (8–12 years), and 0.41 g/kg/day (>12 years) in the G3-a group; 0.68 g/kg/day (<8 years), 0.47 g/kg/day (8–12 years), and 0.39 g/kg/day (>12 years) in the G3-b group; and 0.62 g/kg/day (<8 years), 0.46 g/kg/day (8–12 years), and 0.35 g/kg/day (>12 years) in the G3-c group (p=NS). The median maintenance lactulose dose was 2.0 mL/kg/day (<8 years) and 1.1 mL/kg/day (8–12 years) in the G3-a group, 2.5 mL/kg/day (<8 years) and 1.3 mL/kg/day (8–12 years) in the G3-b group, and 1.63 mL/kg/day (<8 years) and 0.93 mL/kg/day (8–12 years) in the G3-c group (p=NS). In all groups, only PEG 4000 was used as a therapeutic agent in children over 12 years of age (Table 2).
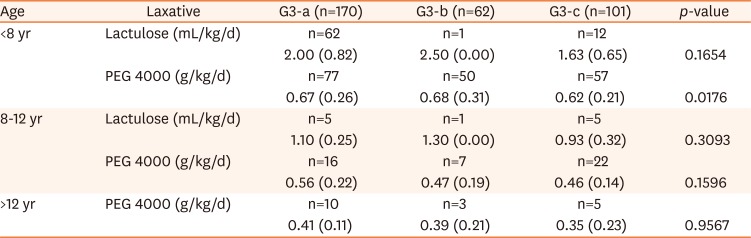
Table 2
Maintenance laxative type and dose by group
G3-a: infrequent bowel movement without fecal soiling group, G3-b: infrequent bowel movement with fecal soiling group, G3-c: fecal soiling group.
![]()
To compare the results of the CTT test, each group was further subdivided into 2 subgroups by age. The results of the CTT test in children under 5 years old were as follows: In the G3-a group, normal in 6 (27.3%), outlet obstruction type in 11 (50.0%), and slow transit type in 5 (22.7%); in the G3-b group, normal in 6 (22.2%), outlet obstruction type in 18 (66.7%), and slow transit type in 3 (11.1%); in the G3-c group, normal in 3 (17.6%), outlet obstruction type in 10 (58.8%), and slow transit type in 4 (23.5%) (p=NS). The CTT in children under 5 years old was 48.6 hours (IQR 39.6) in the G3-a group, 52.8 hours (IQR 32.4) in the G3-b group, and 66.0 hours (IQR 25.2) in the G3-c group (p=NS). The CTT test results in children over 5 years old were as follows: In G3-a group, normal in 10 (43.5%), outlet obstruction type in 9 (39.1%), and slow transit type in 4 (17.4%); in the G3-b group, normal in 4 (26.7%), outlet obstruction type in 9 (60.0%), and slow transit type in 2 (13.3%); in the G3-c group, normal in 9 (32.1%), outlet obstruction type in 17 (60.7%), and slow transit type in 2 (7.1%) (p=NS). The CTT test results in patients over 5 years old was 48.0 hours (IQR, 43.2) in the G3-a group, 70.8 hours (IQR, 42.0) in the G3-b group, and 52.2 hours (IQR, 39.0) in the G3-c group (p=NS). There was no statistically significant difference in CTT or type among the 3 groups (Table 3).
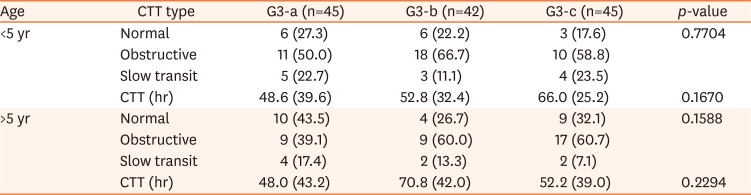
Table 3
CTT Type and CTT (hours) by group
Values are presented as number (%) or median (Interquartile range).
CTT: colon transit time, G3-a: infrequent bowel movement without fecal soiling group, G3-b: infrequent bowel movement with fecal soiling group, G3-c: fecal soiling group.
![]()
The patients were additionally classified into 2 groups according to the presence or absence of fecal soiling. In the non-fecal soiling group (G2-a, n=170), there were 82 (48.2%) male patients. In the fecal soiling group (G2-b, n=163), there were 107 (65.6%) males (p=0.0008). The median age and IQR were 33.0 (45.0) months in G2-a and 63.5 (52.5) months in G2-b (p<0.0001). The age at onset (IQR) was 7 (10) months in the G2-a group and 12 (19.5) months in the G2-b group (p=0.0062). Symptom duration (IQR) was 12 (18) months in the G2-a group and 24 (12) months in the G2-b group (p=0.0070). The number of children who used PEG 4000 was 103 (60.6%) in the G2-a group and 144 (88.3%) in the G2-b group (p<0.0001) (Table 4).

Table 4
Patients' demographic and clinical characteristics by group
Values are presented as median (Interquartile range) or number (%).
G2-a: Non-fecal soiling group, G2-b: Fecal soiling group.
![]()
The median maintenance doses of PEG 4000 were 0.67 g/kg/day (<8 years), 0.56 g/kg/day (8–12 years), and 0.41 g/kg/day (>12 years) in the G2-a group; 0.65 g/kg/day (<8 years), 0.46 g/kg/day (8–12 years), and 0.37 g/kg/day (>12 years) in the G2-b group (p=NS). The median maintenance doses of lactulose were 2.0 mL/kg/day (<8 years) and 1.1 mL/kg/day (8–12 years) in the G2-a group and 1.7 mL/kg/day (<8 years) and 1.02 mL/kg/day (8–12 years) in the G2-b group (p=NS) (Table 5).
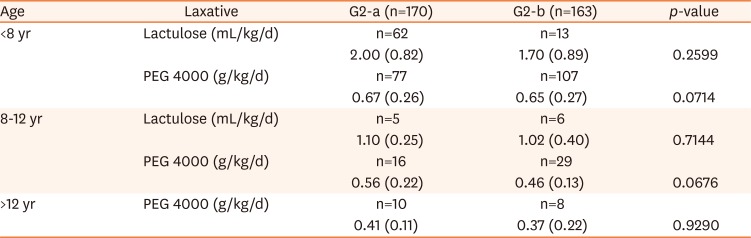
Table 5
Laxative maintenance doses by group
![]()
The CTT test results in patients under 5 years of age were: In the G2-a group, normal in 6 (27.3%), outlet obstruction type in 11 (50.0%), and slow transit type in 5 (22.7%); and in the G2-b group, normal in 9 (20.5%), outlet obstruction type in 28 (63.6%), and slow transit type in 7 (15.9%) (p=NS). The CTT in patients under 5 years old was 48.6 hours (IQR, 39.6) in the G2-a group and 63.6 hours (IQR, 30.0) in the G2-b group (p=NS). The CTT test type results in patients over 5 years of age were as follows: In the G2-a group, normal in 10 (43.5%), outlet obstruction type in 9 (39.1%), and slow transit type in 4 (17.4%); in the G2-b group, normal in 13 (30.2%), outlet obstruction type in 26 (60.5%), and slow transit type in 4 (9.3%) (p=NS). The median CTT s in patients over 5 years of age were 48.0 hours (IQR, 43.2) in the G2-a group and 58.8 hours (IQR, 42.0) in the G2-b group (p=NS) (Table 6).
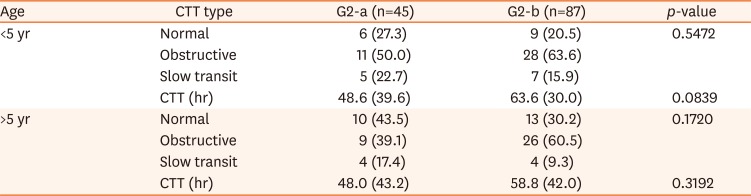
Table 6
CTT Type and CTT (hours) by group
Values are presented as number (%) or median (Interquartile range).
CTT: colon transit time, G2-a: Non-fecal soiling group, G2-b: Fecal soiling group.
![]()
Go to :
DISCUSSION
In this study, severely constipated children were classified by symptoms, bowel movement frequency, and presence of fecal soiling. The fecal soiling group included the oldest children and was male dominant. It also had the latest onset and the longest symptom duration. PEG 4000 was prescribed more frequently than lactulose in all groups and its use was prominent in the fecal soiling group. The infrequent bowel movement group included the youngest children and was female dominant. It also had the earliest onset and shortest symptom duration. However, in terms of CTT test results and medicine doses, there were no significant intergroup differences. Infrequent bowel movements and fecal soiling represent the advanced stages of functional constipation.
In pediatric functional constipation, those with severe constipation could be identified according to clinical information [9]; however, we could expand such considerations according to our clinical experiences with fecal soiling, decreased bowel movement, effective medicine type and dose, symptom duration, and CTT test result type.
Stool frequency depends on age in children. A number of studies have revealed a decline in stool frequency from >4 stools per day during the first week of life to 1 per day at 4 years of age with a corresponding increase in stool size [1011]. In severely constipated children, bowel movements are usually painful and can lead to a withholding behavior. This behavior may be one of the most important causes of infrequent bowel movements in children. However, delayed bowel movements should be considered a possible cause. Slow transit constipation (STC) is defined as decreased colonic transit time as measured by radiopaque makers. Such patients respond poorly to laxatives [12]. The slow transit may involve the entire colon or just a segment. STC can be caused by myopathic, neuropathic, and interstitial cells of Cajal (ICCs) disorders of the colon but may also be related to autonomic dysfunction. Histologic abnormalities have been reported in STC, including decreased numbers of ICCs, argyrophilic neurons, neurofilaments, and overall nerve fibers [131415]. Several studies have shown a decrease in excitatory neurotransmitters and an increase in inhibitory neurotransmitters in STC. There have been reports of decreased substance P and acetylcholine release and increased vasoactive intestinal polypeptide or nitric oxide release [1617]. Studies are conflicting on other neurotransmitters, including neuropeptide Y and serotonin [151819]. Also, STC patients have been shown to have excessive methane-producing flora [1920]. In addition, there may be coexistent disorder of the pelvic floor and anorectal function. In a previous study, about 15% of patients with puborectalis relaxation failure showed a slow transit type on CTT testing [2122].
Fecal soiling is estimated to affect 0.8–4.1% of children in Western society and 2–7.8% in Asia. Fecal soiling is defined as involuntary passage of fluid or semisolid feces around the fecal impaction as a result of fecal loading overflow [232425]. Functional fecal retention is the most common cause of chronic constipation in children. It is accompanied by soiling when the constipation is worse and often caused by fear of painful defecation in children. Children learn to control the passage of feces at an average of 28 months [26]. Voluntary contraction of the sphincter muscle in response to a perception of rectal distention is one of the most important continence mechanisms. There are several causes of fecal incontinence: gastrointestinal disorders including irritable bowel syndrome, inflammatory bowel disease, grade 3 or 4 hemorrhoids that obstruct closure of the anal sphincter, and rectal prolapse. Spinal cord injury or pudendal nerve injury increase the risk of passive fecal incontinence.
Afferent nerve injury causes the rectum to be hyposensitive to rectal filling. Conversely, when the rectum is hypersensitive to rectal distention due to increased smooth muscle tone, it increases the risk of irresistible urgent fecal incontinence. Decreased internal anal sphincter pressure from fecal impaction or sphincter injury is a risk factor for passive fecal incontinence [27]. Non-retentive fecal incontinence occurs without fecal retention or an underlying medical condition and is associated with normal defecatory function, unlike functional constipation. A psychological disorder could be present in such cases [28].
Fecal soiling in pediatric functional constipation indicates that the constipation is much worse than most cases. If the associated disease is not diagnosed and there is a relevant response to medication, the prognosis is usually good, even if takes a long time. In the present study, the patients were divided into 2 groups, conceptually: children with infrequent bowel movements and children with fecal soiling. However, some patients have both clinical symptoms, as shown in this study. If fecal withholding persists, bowel movement frequency may decrease or soiling may occur. Puborectalis relaxation failure may present as infrequent bowel movements and appear as STC on a CTT test. However, puborectalis relaxation failure may also present as fecal soiling. It is important to consider that there are a few overlapping areas between infrequent bowel movement and fecal soiling.
CTT test results are related to constipation therapy outcomes. Children with abnormal CTT test results respond more poorly to medication than those with normal CTT test results [5]. A CTT longer than 100 hours predicted a poor outcome at 1 year. The CTT was longer in children with fecal soiling than in those without fecal soiling [2930]. In this study, there was no statistically significant difference in CTT between the infrequent bowel movement group and the fecal soiling group. However, in both groups, CTT was longer than the normal CTT value of 42 hours for Korean children [31].
PEG 4000 has a better outcome than lactulose for stool frequency, stool form, and abdominal pain relief [323334]. In a previous study, 51.1% of patients were taking PEG 4000 and 48.9% were taking lactulose in the normal transit group. In the abnormal transit group, 91.8% were taking PEG 4000 and 8.2% were taking lactulose. PEG 4000 was prescribed more frequently in the fecal soiling group than in the non-fecal soiling group [7]. In this study, PEG 4000 was more frequently prescribed than lactulose in both groups. PEG 4000 was used more frequently in the fecal soiling group than in the infrequent bowel movement group. However, there were no statistically significant intergroup differences in the initial maintenance dose. The maintenance dose of PEG 4000 for children under 8 years old was higher than that of previous studies of ordinary Korean children [35].
The fecal soiling group was the oldest group, had the latest onset, had the longest symptom duration, and was male dominant. This suggests that the constipation worsened over time. The infrequent bowel movement group was the youngest group, had the earliest onset, had the shortest symptom duration, and was female dominant. This may reflect that intestinal diseases that can affect colon motility developed in early life or that the withholding behavior began at a young age because of environmental factors or fear of bowel movement pain.
A limitation of this study is that, although children with STC were selected based on the CTT test at a tertiary center, insufficient numbers of those with serious colonic diseases that can affect colonic motility, like colonic inertia, were enrolled in this study. To diagnose histologic abnormalities, a colon biopsy is mandatory; however, in most cases we performed only a CTT test, fluoroscopic defecography, and high-resolution manometry.
In the infrequent bowel movement and fecal incontinence groups, CTT was prolonged and PEG 4000 was prescribed frequently. This implies that both symptoms represent the advanced stage of chronic functional constipation.
Go to :
 XML Download
XML Download