

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pediatric obesity has increased in prevalence in the last 2 decades worldwide: specifically, in the United States, 8.4% for preschool children (2–5 years), 17.7% for school aged children (6–11 years), and adolescents (12–19 years) [1].
Prevalence is also increasing in Asian countries due to westernized high calorie diet, sedentary lifestyle, and decreased physical activity. In China, obesity among children aged 2–18 was 18.7% [2]. Meanwhile, in Korea, among children aged 7–18, the obesity rate was 8.4% in 2008 and 14.3% in 2016 [3].
Childhood obesity causes physical complications that impact the endocrine, digestive, respiratory, cardiovascular, and musculoskeletal systems. In a recent meta-analysis, the prevalence ratio for pediatric obesity to healthy weight groups for prediabetes was 1.4, high blood pressure >90 percentile at 4.4, and nonalcoholic fatty liver disease at 26.1 [4].
In addition to physical complications, pediatric obesity also affects self-esteem, body image, and social relations, which can be a risk factor for psychiatric disorders, psychopathology and psychosocial complications [567]. A recently published guideline strongly recommends that obese children be monitored for mental health problems and screened for psychiatric treatment [8].
Treatment of pediatric obesity requires multidisciplinary interventions including medical and lifestyle interventions, psychosocial support, and pharmacological strategies, as well as bariatric medical procedures in extreme cases. Eating behaviors and weight problems are often related with abnormal behavioral patterns due to distorted cognition and negative emotions. Therefore, one of the most up-to-date approaches to managing pediatric obesity is cognitive behavioral therapy (CBT).
Therefore, this review focuses on recent research on mental health issues, psychosocial problems, and CBT in pediatric obesity.
DEPRESSION AND ANXIETY
Previous studies on adults with obesity have reported associations between obesity and depressive disorders, and suggest a reciprocal link between depression and obesity [910]. This reciprocal link can lead to depressive symptoms, as a result of the stigmatization of obesity, or depression can lead to obesity in vulnerable populations.
There is some variation in the symptoms associated with obesity and depression/anxiety in the pediatric obesity study compared to the adult study. A cohort study of 3,134 people aged 11–17 years reported that there was no evidence of reciprocal effects between weight and depression, and the participants' weight did not predict depression [11]. In a meta-analysis published in 2015, the relationship between weight and anxiety was reported as weak [12]. Some studies have reported no significant differences in depression between adolescents and obese adolescents [13]; also, depressive symptoms of obese adolescents were not related to the degree of obesity [14]. Additionally, obesity was not significantly related to marked psychopathology in a study of 3,021 adolescents and young adults in Germany [15].
However, some studies have reported an association between pediatric obesity and depression/anxiety symptoms. Mannan et al. [16] reported obese adolescents had a 40% increased risk of being depressed and reported a bi-directional association of depression and obesity. A meta-analysis of 51,272 children and adolescents published in 2017 reported a positive association between childhood and adolescent obesity and depression [17]. In the case-control study, obese children showed significantly higher levels of depressive symptoms and increased anxiety score [18]. In a recent study published in 2019, 39.8% of treatment-seeking children with overweight/obesity suffered from depression and/or anxiety symptoms [19]. In a meta-analysis, 21.7% of overweight/obese children were diagnosed with depression and 39.8% with anxiety, while 18.0% of non-overweight/non-obese children had depression and 14.0% had anxiety [20].
Although the mechanisms for the association between obesity and depression are still unclear, high depression and anxiety in obese children may share neurobiological mechanisms, such as imbalance in the Hypothalamic-Pituitary-Adrenal axis and altered cortisol levels; also, low self-esteem and negative self-image, as well as lower life satisfaction due to obesity, can lead to anxiety and depression [21]. Indeed, the relationship between depression/anxiety and obesity involves a complex interplay of biological, psychological, and social factors.
These inconsistent results may vary depending on the population, for example, a large community-based sample or a clinical sample being treated in the hospital due to obesity, as well as variation due to the measurement tool, age, and gender of subjects. For example, studies of child and adolescents in a large community have a relatively limited number of obese children, among which significant depression and anxiety symptoms may be masked. Also, in community study, the risk of major depressive disorders and anxiety disorders was higher in female adolescents than in males [22]. This study suggests the possibility of behavioral phenotypes that present aberrant eating, depression, and obesity according to gender.
However, it is important to note that among obese children and adolescents that require clinical treatment, adolescents with developing body images, namely female adolescents, may experience significant depression and anxiety. Depression/anxiety not only decreases treatment compliance, but also negatively impacts growth and development. Additionally, a 20-year cohort study also reported that childhood overweight and obesity may increase the risk for mood disorder in adulthood [23]. Early identification and active intervention in depression and anxiety are required in vulnerable obese children and adolescents.
EATING DISORDERS
Obese adolescents may experience body image dissatisfaction as they begin to undergo physical and cognitive changes during the transition from childhood to adulthood, and are at risk of eating disorders such as anorexia, bulimia, and binge eating disorder (BED) [2425]. Overweight adolescents have 4.91 times higher risk of eating disorders than non-overweight adolescents [26].
BED is associated with a large amount of binge eating, accompanied by a sense of loss of control and is the most common eating disorder among obese patients. Uncontrolled eating increases the chance of excess energy intake over time and is a predisposing factor for weight gain and obesity. Attempts to limit calorie intake in obese children may also affect the onset and maintenance of binge eating. Thirty-three percent of moderate to severe BEDs were reported in a study of adolescents between the ages of years in the United States [27]. Moreover, a recent study reported that the prevalence of moderate or severe BED in French overweight and obese adolescents was 41.7%, in which 25.0% of anxiety and 36.5% of depression [28].
Decaluwé et al. [29] reported that 36.5% of obese children aged 10–16 years experienced binge eating episodes, and that ‘loss of control eating (LOC eating)’ would be a therapeutic target to improve the outcome of obesity treatment. Studies on the relationship between binge eating, emotions, and temperamental traits in obese children suggest that body dissatisfaction in obese adolescents can lead to eating disorders through low self-esteem and depression [30]. Children and adolescents with LOC eating experience more anxiety, depression, and body dissatisfaction than children who do not have LOC eating. A review published in 2019 reports that LOC eating is not only a risk factor for obesity but is also associated with anxiety, depression, and more severe eating disorders in adulthood. In addition, in the obese child with LOC eating, the impulsivity trait influences dysregulated eating behavior [31].
Indeed, some obese children have LOC eating, which leads to eating disorders. The symptoms of eating disorders are influenced by body dissatisfaction, emotional eating due to negative emotions, and temperament characteristics, such as impulsivity, which may lead to low treatment response. Therefore, the Expert Committee recommends that binge eating, or purging behavior, should be evaluated in obese youths [32], and eating disorder symptoms, like LOC eating, requires therapeutic intervention in pediatric obesity treatment.
ATTENTION DEFICIT HYPERACTIVITY DISORDER
Some studies have shown a high probability of attention deficit hyperactivity disorder (ADHD) in obese children and adolescents [3334]. Overweight or obese children are twice as likely to be diagnosed with ADHD [35], while this diagnosed was made in 28.6% of adolescents with severe obesity [36].
Recent genome-wide association studies have reported that higher body mass index (BMI) increases the risk of developing ADHD [37]. In the mechanism of the association between ADHD and obesity, impulsivity and inattention, which are core symptoms of ADHD, are thought to increase the risk of obesity. Children diagnosed with ADHD has difficulty maintaining their attention on tasks and there is a high probability that they have difficulty controlling tendency to overeat. Impulsivity in children with ADHD may be associated with disinhibited eating behavior patterns, and dysregulation of the dopaminergic reward system in ADHD may lead to unhealthy food intake, since children with ADHD are susceptible to behaviors that provide immediate reward or instant gratification. In addition, lack of executive function leads to difficulties in controlling eating behavior due to difficulties in planning and organization, and inattention may affect lack of awareness of hunger and satiety [33].
The traits of impulsivity and inattention associated with ADHD can lead to decreased motivation and treatment compliance, which can be a risk factor for obesity treatment failure, so clinical attention to ADHD symptoms may be required in pediatric obesity. A previous study suggests that it is necessary to screen for ADHD symptoms and impulsive eating among obese children, and to consider behavioral interventions and pharmacological therapy as needed [38].
PSYCHOSOCIAL PROBLEM
Childhood obesity is a risk factor for psychosocial problems, including bullying, social stigmatization, and peer rejection. In a study of 43,297 children between the ages of 10–17 years reported that obese children had high activity restriction, academic difficulties and missed school days [39].
In a study published in 2019, adolescents with overweight and obesity were more likely to be the target of bullying behaviors than healthy weight peers. Also, those adolescents with overweight and obesity had higher behavioral conduct problems and difficulty making friends [40]. Meta-analysis published in 2019, which analyzes research published in 41 low- and middle-income countries, reported that overweight and obesity were both associated with significantly increased odds or bullying by being made fun of because of physical appearance among both sexes-obese adolescents compared to adolescents with normal weight [41].
Weight stigma poses various psychological and physical health problems for children and adolescents, including binge eating, social isolation, avoidance of health care services, decreased physical activity, and increased weight gain [42].
Body image is defined as an individual's personal judgment of his or her own physical appearance. Obese children and adolescents may feel dissatisfied with their weight and body shape. Furthermore, there was a higher probability for individuals in this population to report being teased about their body shape or weight [43]. Also, obese youth, regardless of gender, reported poorer quality of life and higher rates of body image dissatisfaction compared with their normal-weight counterparts [44]. Also, obese youth are more likely to report difficulties with sleep and degree of obesity was predictive of increased sleep difficulties and decreased quality of life score [14]. According to a recent study on impact of psychosocial risk on obesity treatment outcomes, children with moderate or high psychosocial risk were 3.1 times more likely to be lost to treatment follow-up and have poorer weight outcomes [45]. Pediatric obesity is associated with poor psychosocial outcomes, and since psychosocial problems have a negatively impact on the course and prognosis of pediatric obesity, so, active intervention is required.
COGNITIVE BEHAVIORAL THERAPY FOR PEDIATRIC OBESITY
The 2016 World Health Organization Commission on Ending Childhood Obesity report, recommended “family-based, multicomponent, lifestyle weight management services for children and young people who are obese” [46]. Also, behavioral interventions, including controlling caloric intake, decreasing sedentary time, and increasing physical activity are important in pediatric obesity treatment.
However, behavioral therapy shows short-term effects of lifestyle changes and weight loss, but lacks evidence for long-term effectiveness, and in fact, some studies show behavioral interventions for treating overweight and obesity in children and youth are associated with a low to moderate treatment effect [4748].
Psychological factors, such as distorted body image, negative emotions, and failure to stimulus control impact eating behavior and weight problem in pediatric obesity. Recently, CBT has become an important area of pediatric obesity treatment. CBT is a theoretically based treatment approach that highlights the relationship between cognitions, feelings, and behaviors, and utilizes techniques involving motivational enhancement, goal-setting, problem-solving, and knowledge/skill acquisition that can facilitate sustainable behavior changes.
CBT, when used in combination with dietary or exercise interventions, led to more weight loss than when only using dietary or exercise interventions [49]. Furthermore, CBT can help maintain weight loss more efficiently than behavioral therapy [50]. Recently, the Committee on Pediatric Obesity of the Korean Society of Pediatric Gastroenterology Hepatology and Nutrition recommended CBT, which may be beneficial for treating childhood obesity [8].
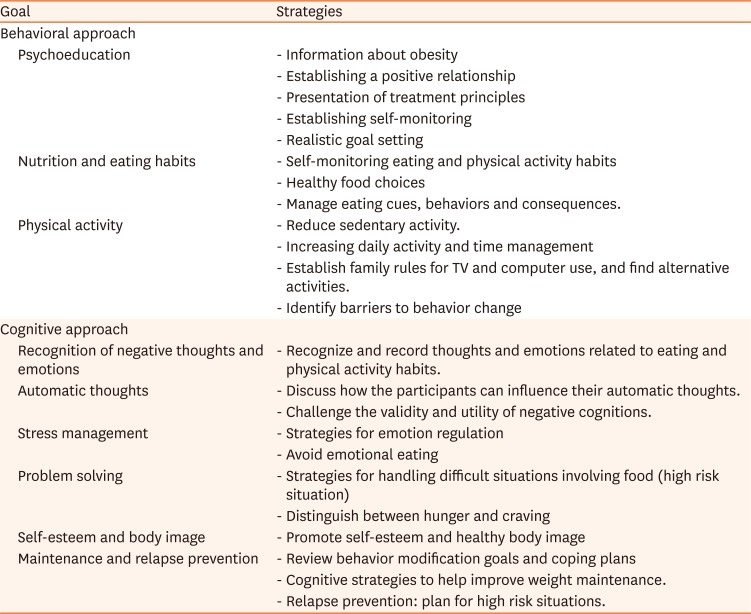
The common components of pediatric obesity CBT proposed in the previous studies were a behavioral approach aiming to change eating habits and physical activity through self-monitoring, and cognitive approach to change distorted body image and help emotion regulation (Table 1) [5152]. In particular, the cognitive approach includes thinking about emotions and negative automatic thoughts related to eating habits, helping to regulate emotions, promoting problem solving to cope with high-risk situations where food control is difficult, changing self-esteem and body image, and cognitive strategies to prevent relapse. Some studies aimed at improving parenting strategies, as well as parent-child interactions, by adding parent education sessions, considering that the subjects were children and adolescents.
Table 1
Common components of CBT for obese children and adolescents
Among recent studies related to the effects of CBT on pediatric obesity (Table 2) [53545556], most CBT interventions include 6 to 10 sessions (90 minute/session) in face to face format. In the CBT group, healthier food habits were adopted compared to the control group, and psychosocial health, health-related quality of life, and self-esteem improved, as well as improvement of anthropometrical variables, such as BMI and waist circumference.
Table 2
Recent update of CBT trials for obese children and adolescents (published in 2018-2019)
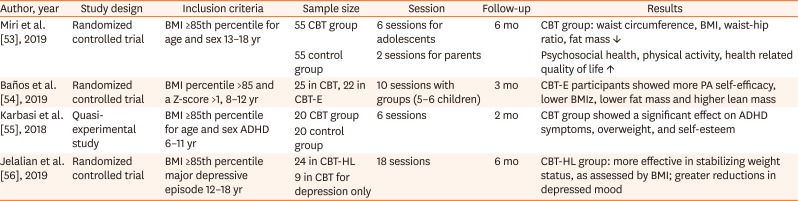
| Author, year | Study design | Inclusion criteria | Sample size | Session | Follow-up | Results |
|---|---|---|---|---|---|---|
| Miri et al. [53], 2019 | Randomized controlled trial | BMI ≥85th percentile for age and sex 13–18 yr | 55 CBT group | 6 sessions for adolescents | 6 mo | CBT group: waist circumference, BMI, waist-hip ratio, fat mass ↓ |
| 55 control group | 2 sessions for parents. | Psychosocial health, physical activity, health related quality of life ↑ | ||||
| Baños et al. [54], 2019 | Randomized controlled trial | BMI percentile >85 and a Z-score >1, 8–12 yr | 25 in CBT, 22 in CBT-E | 10 sessions with groups (5–6 children) | 3 mo | CBT-E participants showed more PA self-efficacy, lower BMIz, lower fat mass and higher lean mass |
| Karbasi et al. [55], 2018 | Quasi-experimental study | BMI ≥85th percentile for age and sex ADHD 6–11 yr | 20 CBT group | 6 sessions | 2 mo | CBT group showed a significant effect on ADHD symptoms, overweight, and self-esteem |
| 20 control group | ||||||
| Jelalian et al. [56], 2019 | Randomized controlled trial | BMI ≥85th percentile major depressive episode 12–18 yr | 24 in CBT-HL | 18 sessions | 6 mo | CBT-HL group: more effective in stabilizing weight status, as assessed by BMI; greater reductions in depressed mood |
| 9 in CBT for depression only |
In an attempt to maintain achievement, a recent noteworthy study prevent relapses by helping subjects to foster a healthier lifestyle by combining web platforms to increase treatment adherence [54]. This study used a variety of multimedia elements in contrast to traditional CBT, provided a clinician support system (evaluation, and intervention, and progress of the children established by the clinician), home support system (children contact clinicians and access tasks), mobile support system (children register amount of food intake, physical activities performed in real time) through web platforms. This approach improved anthropometrical variables by enhancing self-efficacy, compared to traditional CBT, in face to face format.
Also, a recent study highlighted the need to note the effects of CBT treatment on obese children and adolescents with psychiatric disorders. The CBT group can positively affect BMI and ADHD symptoms compared to the control group when parent focused CBT is administered to pediatric obese children with a mean age of 8.4 years [55]. This result suggests that when ADHD is comorbid with obesity in children who may have difficult with comprehension in individual CBT sessions due to cognitive function, parent-centered obesity CBT can be effective in involving parents in the treatment of obesity, and has the effect of developing healthy habits and helping with the parenting role. In a study of obese adolescents with major depressive disorder, CBT for depression modified to address aspects of healthy living and nutrition (CBT plus healthy lifestyle, CBT-HL), including content on body image and coping with food cravings, and attention to the relationship between depressed mood and weight. CBT-HL group showed greater improvement of depressive symptoms and stabilization of weight status than CBT for depression only [56]. These findings suggest that CBT, including areas of recognition of negative emotions and negative self-image and problem solving, may be more effective than behavioral therapy, especially in obese children and adolescents with psychiatric symptoms, such as impulsivity or depression.
Multidisciplinary treatment for children/adolescents with obesity should focus on psychological consequences, like body image dissatisfaction, LOC, obesity stigma, and low self-esteem. Especially in the treatment of pediatric obesity with mental health problems or psychosocial problems, CBT may be an important treatment approach in terms of multidisciplinary treatment. In the future, multisite research on various CBT approaches, such as using multimedia and applications or parental involvement in treatment are needed for pediatric obesity treatment.
CONCLUSION
Recent studies suggest that evidence for association between pediatric obesity and psychiatric disorder, such as depression, eating disorders, ADHD is increasing. Also, pediatric obesity experiences psychosocial problems, such as bullying, sleep problems, quality of life, and school adjustment problems. Mental health problems and psychosocial problems need clinical attention because these problems negatively affect the progress and prognosis of obesity treatment, as well as psychosocial development during critical period. CBT is more helpful in cases of mental health problems and psychosocial problems, Research is needed on various approaches and techniques of CBT in pediatric obesity treatment.
 XML Download
XML Download