

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hip fractures in the elderly are associated with high mortality and morbidity and are expected to increase in the future. These fractures are a socioeconomic burden to both individuals and the community.1234
Postoperative pneumonia has been known as a common complication in elderly hip fracture patients.56 The incidence of postoperative pneumonia ranged from 5% to 10%.789 Men gender, prolonged operation, multi-organ failure, malnutrition, mechanical ventilation, old age, pre-existing pulmonary disease, low body mass index have been reported as risk factors for postoperative pneumonia.10 The postoperative pneumonia is a major cause of early mortality in these patients. Previous studies reported the short-term mortality of 14%–27.1%.511 However, there is a lack of studies on mid- to long-term effects of pneumonia on death of hip fracture patients. In addition, the differences in the effect of pneumonia according to the age and gender of patients on mortality are not known.
Therefore, we aimed 1) to investigate the incidence of pneumonia during hospitalization period in elderly hip fracture patients and 2) to evaluate the effect of pneumonia on mortality from 30 days to 1 year after the surgery and 3) to analyze the difference of mortality rate according to patient's age and gender using a nationwide cohort of Korea.
METHODS
Database
This retrospective review used data from the Health Insurance Service-Senior cohort (NHIS-Senior) of Korea. This database was constructed to represent the elderly living in Korea and included approximately 5.5 million enrollees, who were older than 60 years of age. From the NHIS-Senior database, a total of 588,147 participants were randomly selected using 10% simple random sampling. All individuals included in the NHIS-Senior were followed until December 31, 2015 unless death or disqualification for National Health Insurance such as emigration occurred. The NHIS is the only payer under the single-insurer system of nationwide health coverage in Korea. Virtually all Korean citizens are enrolled in NHIS, and they are categorized into insured employees, insured self-employed individuals, or medical aid beneficiaries.1213 Data set included all inpatient and outpatient medical claims including codes of diagnoses and treatment procedure codes.
Identification of elderly hip fracture
The eligibility criteria for elderly hip fracture patients were: 1) first-time admission to an acute care hospital (index admission) with diagnostic codes of femoral neck fractures (International Classification of Diseases, 10th Revision [ICD-10] S720) or intertrochanteric fractures (ICD-10 S721)1415; 2) at least a three year hip fracture-free period prior to the index hip surgery; 3) recipients of hip fracture surgeries including internal fixation (open reduction [femur], closed pinning [femur]), hemiarthroplasty (hip), and total arthroplasty (hip); and 4) age of 65 to 99 years at the time of a hip fracture surgery.15 To ensure a minimal 1-year follow-up period, patients with a hip fracture, which occurred within less than 1-year before the end of the observation period (December 31, 2015) were excluded. Patients who had a hip fracture prior to December 31, 2004, were also excluded to make sure of hip fracture-free period longer than 3-year. The incidence date (index date) of hip fracture was defined as the date of admission to the acute care hospital that fulfilled the eligibility criteria. The last date of follow-up was defined as the date of death or December 31, 2015, whichever came first.
Identification of pneumonia patients
The diagnostic codes used to identify pneumonia patients were J10-J18 based on validation study of ICD-10.16 Pneumonia during the hospitalization was identified from the diagnostic code of pneumonia claimed during the first time admission period to an acute care hospital due to hip fracture and there is no diagnostic code within 30 days prior to index date.
All-cause mortality
In the NHIS-Senior, each subject's unique de-identified number was linked to mortality information from the Korean National Statistical Office.15 Thus, all deaths of subjects were identified and the time lapse from index date to date of death was used to define survival time.
Statistical analysis
Baseline characteristics were identified at the time of hip fracture (time zero). Survival time used in survival analyses was defined as the days from the index date to the date of death or December 31, 2015, whichever occurred first. If the hip fracture surgery was done and pneumonia occurred during the same admission episode, the date of pneumonia was set to the same date (time zero) as that of the hip fracture. The cumulative survival probabilities and survival curves were estimated and graphed by a Kaplan-Meier method using the product-limit formula. Comparison of survival was performed by using the log-rank test on the null hypothesis of a common survival curve. A multivariable-adjusted Cox proportional hazard model was used to investigate the effects of pneumonia on all-cause mortality. A generalized estimating equation model with a Poisson distribution and logarithmic link function was performed to estimate adjusted risk ratios (aRRs) and 95% confidence intervals (CIs) to assess the association between pneumonia and the cumulative mortality at different time frames (postoperative 30-, 90-, 180-day, and 1-year).
Included covariates were age group, gender, household income level, residential area, Charlson Comorbidity Score (CCS), fracture type, surgery type, anesthesia type, hospital stay, and year of the hip fracture occurrence. Number of comorbidities at each subject was assessed by diagnostic codes during the 3 years before the index date using the Quan ICD-10 coding algorithm of the CCS.17
The statistical analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute, Cary, NC, USA). P values < 0.05 were considered statistically significant.
RESULTS
From January 2002 to December 2015, 19,915 patients underwent surgeries for hip fracture. Among them, 14,736 patients, who were older than 65 years at the time of surgery, were subjects of this study (Fig. 1). Postoperative pneumonia developed in 1,629 patients (11.05%) during the hospitalization (pneumonia group) while it did not develop in the remaining 13,107 patients (88.95%) (non-pneumonia group) (Table 1). The pneumonia incidence was 16.39% (601/3,666 patients) in men patients and 9.29% (1,028/10,042 patients) in women patients. The 30-, 90-, 180-day, and 1-year cumulative mortalities were 3.25%, 11.17%, 14.61% and 18.11% in men pneumonia patients, and 3.56%, 12.22%, 17.37% and 21.98% in women pneumonia patients.

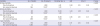
Table 1
Baseline characteristics of study participants

![]()
Compared to non-pneumonia patients, aRR of death in pneumonia patients was 2.69 (95% CI, 2.14–3.38; P < 0.001) within postoperative 30-day. The aRR of pneumonia patients was 3.40 (95% CI, 3.01–3.83; P < 0.001) within postoperative 90-day, 2.86 (95% CI, 2.61–3.15; P < 0.001) within postoperative 180-day and 2.31 (95% CI, 2.14–2.50; P < 0.001) within postoperative 1-year. The effect of pneumonia on all-cause mortality was highest within postoperative 90-day (Table 2 and Fig. 2).
Table 2
Effect of pneumonia on all-cause mortality of different time frame
![]()
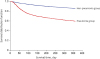 | Fig. 2Kaplan-Meier curve of elderly hip fracture patients according to the pneumonia. P value of log-rank test was < 0.001.
|
The aRR of death in the pneumonia group was 5.75 (95% CI, 2.89–11.43) in patients aged < 70 years, 5.14 (95% CI, 4.08–6.46) in those aged 70–79 years, 3.29 (95% CI, 2.81–3.86) in those aged 80–89 years and 2.02 (95% CI, 1.52–2.69) in those aged ≥ 90 years (Table 3).
Table 3
Effect of pneumonia on all-cause 90-day mortality according to the age group in elderly hip fracture patients

![]()
The aRR of death was 3.63 (95% CI, 3.01–4.38) in men pneumonia patients, and 3.27 (95% CI, 2.80–3.83) in women pneumonia patients (Table 4).

DISCUSSION
The principle findings of this study are that the prevalence of pneumonia in elderly patients with hip fracture was 11.05% and the aRR of postoperative pneumonia on all-cause mortality was 2.31 to 3.40 according to different time frames from postoperative 30 days to 1 year.
Lv et al.5 reviewed 1,429 Chinese patients who underwent hip fracture surgery and reported 4.9% incidence of postoperative pneumonia. Skull et al.18 also reported a 4.9% pneumonia incidence in a study of 153,613 Canadian patients with hip fracture complications. Recently, Roche et al.10 retrospectively reviewed 519 Korean hip fracture patients aged ≥ 60 years, and reported that postoperative pneumonia developed in 8.8%. In their study, old age, low body mass index, malnutrition, longer duration of surgery and delayed surgery were identified as risk factors of aspiration pneumonia.10 Quan et al.19 reported a comparative study of inpatient pulmonary rehabilitation program in 240 Chinese hip fracture patients. The intervention group had a lower incidence of pneumonia (6 patients, 5.9%) compared to the control group (19 patients, 13.9%). The incidence of pneumonia in our patients was comparable with those of previous studies.
Sheehan et al.20 reported that men patients had higher incidence of postoperative pneumonia by 2.1 times than women patients after surgery for geriatric hip fracture. Smoking history and combined chronic obstructive pulmonary disease might explain the high risk of postoperative pneumonia in men patients.21 In our study, the incidence of pneumonia was higher in men patients than in women patients (16.39% vs. 9.29%).
Lawrence et al.22 and Smetana23 reported that men patients with postoperative pneumonia after hip fracture surgery had higher mortalities than women patients. Bohl et al.24 reported that the 30-day mortality rate in men patients after hip fracture surgery was 1.74 times higher than that of women. However, in our study, the risk of death by pneumonia was not different between the 2 genders (P for interaction > 0.05) after adjusting underlying comorbidities. Although men patients seemingly have higher risk of developing pneumonia and higher mortality rate than women patients in previous studies, the higher risk in men patients was not due to gender difference but due to underlying comorbidities of men patients.
There are limitations in our study. First, our study was based on the national claim data. Thus, we could not evaluate the effect of bone mineral density, body mass index, smoking history, alcohol abuse, the levels of vitamin D and calcium on the pneumonia development and mortality. Nevertheless, we attempted to overcome this limitation by adjusting CCS, socio-economic factors and residential area. Second, the national claim data did not include information about preoperative medical optimizations or postoperative care programs, which might have affected the rates of postoperative pneumonia and mortality.
In conclusion, the prevalence of postoperative pneumonia in elderly hip fracture patients was 11.05% and the pneumonia patients had higher 30-day to 1-year mortalities with aRR of 2.31 to 3.40 compared to non-pneumonia patients. They had increased mortality in all age group older than 65 years with aRR of 1.52 to 4.08. Both genders of pneumonia patients had higher risk of mortality (aRR, 3.63 in men and 3.27 in women) compared to non-pneumonia patients.
 XML Download
XML Download