

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pyogenic liver abscess caused by Klebsiella pneumoniae has emerged in East Asia including Taiwan, China, and the Republic of Korea (ROK).123 This condition is frequently complicated by an extrahepatic metastatic infection such as septic endophthalmitis and is primarily caused by strains of hypervirulent K. pneumoniae (hvKP).4 For hvKP liver abscess, K. pneumoniae serotype K1 is the most prevalent serotype and sequence type (ST) 23 is the predominant type identified from multilocus sequence typing (MLST).4 In addition, hvKP is known to have virulence genes related to the expression of the hypermucoviscous phenotype manifested as a positive string test, which would facilitate further invasion by enhancing resistance to phagocytosis.5 Also, virulence genes related to iron uptake for promoting bacterial replication and survival are well characterized in hvKP.6 These virulence factors are thought to contribute to the pathogenesis of hvKP liver abscess, even in healthy individuals. Previous epidemiological studies suggested that higher rate of K. pneumoniae including hvKP intestinal colonization seen in individuals in Asian countries such as Taiwan and ROK789 may have resulted in transient bacteremia followed by dissemination and invasion of the liver. This possible association was further supported by a study from Taiwan,10 which showed that liver aspirate K. pneumoniae isolates had a pulsed-field gel electrophoresis profile identical or closely related to those of fecal or saliva samples from the same patient with hvKP liver abscess. However, the intestinal colonization rate of K. pneumoniae including hvKP was found to be different in ROK when compared to that of Taiwan,78 which might have an impact on the characteristics of K. pneumoniae of the hvKP liver abscess patients in the ROK. Furthermore, little is known about the characteristics of K. pneumoniae colonizing the intestinal tract of the hvKP liver abscess patients in the ROK.
Therefore, this study aimed to investigate the distribution and characteristics of K. pneumoniae colonizing intestinal tract of the hvKP liver abscess patients in the ROK. Also, we compared the intestinal colonization isolates of K. pneumoniae with the liver abscess strains of hvKP to evaluate the roles of the intestinal colonization of K. pneumoniae in the development of hvKP liver abscess.
METHODS
Study population and bacterial strains
K. pneumoniae isolates from liver aspirate samples and stool samples from hospitalized adult patients diagnosed with hvKP liver abscess at the Korea University Anam Hospital, Seoul, ROK were prospectively collected from 2017 to 2018. Patients were required to meet the inclusion criteria: 1) age ≥ 19 years, 2) confirmation of the primary hvKP liver abscess diagnosis defined with the combination of hvKP isolation from the liver aspirate sample culture and the presence of typical clinical manifestations including fever, right upper abdominal pain, and imaging evidence of liver abscess seen from the computed tomography scan, 3) positive isolation of K. pneumoniae from the stool sample culture. Patients with the following criteria were excluded from this study: 1) possible evidence of a secondary liver abscess such as polymicrobial bacteremia or presence of other intra-abdominal sources of infection (e.g., appendicitis), 2) isolation of bacteria other than K. pneumoniae from the stool sample culture.
The liver aspirate sample from liver abscess was inoculated into one aerobic and one anaerobic blood culture bottle and was placed into a BacT/ALERT® 3D Microbial Detection System (bioMerieux, Inc., Durham, NC, USA). Identification of K. pneumoniae was carried out using matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS; Bruker Daltonics, Bremen, Germany). Antibiotic susceptibility testing was performed using an automated antimicrobial susceptibility testing system (Vitek® 2; bioMérieux Vitek, Hazelwood, MO, USA). Results of antibiotic susceptibility were interpreted according to the standards of the Clinical and Laboratory Standards Institute.11 The string test was performed on identified K. pneumoniae isolates from the liver abscess aspirate sample. HvKP was confirmed if there was a positive string test defined as the formation of viscous string > 5 mm in length.12 The stool sample from the hvKP liver abscess patient was inoculated into the MacConkey media. Identification and antibiotic susceptibility testing of K. pneumoniae from the stool sample were carried out using MALDI-TOF MS and Vitek® 2, respectively. The string test was also performed on the identified K. pneumoniae isolate from the stool sample.
Clinical variables including hvKP liver abscess patients' demographics, comorbid chronic illnesses, clinical manifestations, outcomes, and microbiological data were collected.
Microbiological characterization
The serotype of K. pneumoniae isolates was determined by polymerase chain reaction (PCR) using primers specific for wzy and wzx alleles for detection of serotype K1, K2, K5, K20, K54, and K57 as described previously.13 For detection of other serotypes, sequencing polymorphisms of the wzi gene by PCR was performed as wzi sequencing can offer a reliable determination of the K serotypes of both hvKP and classical K. pneumoniae strains.14 MLST was performed on K. pneumoniae isolates by PCR using known sequence primers for seven housekeeping genes (rpoB, gapA, mdh, pgi, phoE, infB, tonB).15 ST was determined by application of the sequenced data of seven housekeeping genes into the K. pneumoniae MLST database (http://www.pasteur.fr/mlst/). The phylogeny scheme was generated by assembly and editing of nucleotide sequences obtained from the MLST by the software ClustalX2 v2.1 (http://www.clustal.org/clustal) and BioEdit v7.0.5 (http://www.mbio.ncsu.edu/bioedit/bioedit.html). The phylogenetic tree was displayed with iTOL (http://itol.embl.ed).16 Genes encoding major virulence factors (rmpA, magA, iutA) were determined by PCR using known primers as described previously.1718
Statistical analysis
Descriptive statistics were used to analyze the data. The Fisher's exact test was used for dichotomous variables and the Mann-Whitney U test was used for continuous variables where applicable. SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
RESULTS
Clinical characteristics
There was a total of 37 patients diagnosed with the primary hvKP liver abscess during the study period. These primary hvKP liver abscesses were caused by the extended-spectrum beta-lactamase (ESBL) negative and ciprofloxacin-susceptible hvKP isolates except for one patient whose liver abscess was caused by the both ESBL-negative and ciprofloxacin-susceptible hvKP isolate and K. pneumoniae isolate with positive ESBL and sensitivity to ciprofloxacin. Out of 37 patients with the primary hvKP liver abscess, 11 patients were noted to have K. pneumoniae isolated from the stool samples and were enrolled for analyses. There were 8 men (72.7%) and 3 women (27.3%). The median age was 71 years (interquartile range [IQR], 50–75 years). The majority of the patients (72.7%) were without significant underlying comorbidities. Diabetes mellitus (DM) was noted in 1 patient (9.1%). The median Pitt bacteremia score at the hospital admission was 0 (IQR, 0–1). Presence of metastatic infection was noted in 2 patients (18.2%; one patient with endophthalmitis and another patient with endophthalmitis and abscess in the prostate and bilateral psoas muscle) who did not have underlying comorbidities. Third generation cephalosporin (ceftriaxone or cefotaxime) was the most commonly used in-hospital antibiotic treatment (9/11; 81.8%). There was no 30-day mortality among these patients (Table 1).
Table 1
Clinical characteristics of patients with liver abscess caused by hypervirulent Klebsiella pneumoniae
Microbiological characterization
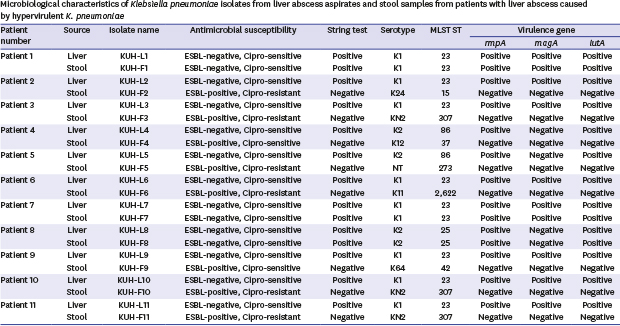
For hvKP isolates from the liver aspirate samples of 11 patients, the most common serotype was K1 (8/11; 72.7%) followed by K2 (3/11; 27.3%). The string test was positive in all hvKP isolates. All K1 serotype isolates were ST23 (8/11; 72.7%). There were ST25 (1/11; 9.1%) and ST86 (2/11; 18.2%) for K2 serotypes. Presence of the major virulence factors (rmpA, magA, and iutA) were noted in all K1/ST23 isolates. However, the absence of magA was seen in all K2 serotype isolates (two ST86 isolates and one ST25 isolate). All hvKP isolates were susceptible to ciprofloxacin without the presence of ESBL. For K. pneumoniae isolates from the stool samples of 11 patients, the majority was non-K1/K2 serotype (8/11; 72.7%). There were two K1/ST23 (18.2%) and one K2/ST25 (9.1%) isolates. The median time between the initiation of antibiotic therapy for hvKP liver abscess and collection of stool K. pneumoniae isolates was 14 days. The string test was positive only in K1/K2 serotype isolates. Among non-K1/K2 serotype isolates, high variability of ST was noted; ST15, ST307, ST37, ST273, ST2622, and ST42 were observed. With regard to antibiotic susceptibility, K1/K2 serotype isolates were susceptible to ciprofloxacin without ESBL. However, a high rate of ciprofloxacin resistance (6/8; 75.0%) and presence of ESBL (8/8; 100.0%) were noted among non-K1/K2 serotype isolates. The major virulence factors (rmpA, magA, and iutA) were absent in all non-K1/K2 serotype isolates. For K1/K2 serotype isolates, these virulence factors were present except for magA, which was absent in the K2 serotype isolate (Table 2). The phylogenetic tree analysis of K. pneumoniae isolates from the liver aspirate sample, and the stool sample by MLST showed a considerable heterogeneity of K. pneumoniae isolates from the stool sample (Fig. 1).
Table 2
Microbiological characteristics of Klebsiella pneumoniae isolates from liver abscess aspirates and stool samples from patients with liver abscess caused by hypervirulent K. pneumoniae

Comparison of characteristics between the concordant and discordant group
The concordance rate of the K. pneumoniae isolates between the liver aspirate sample and the stool sample from the primary hvKP liver abscess was low (27.3%). Between the concordant and discordant group of K. pneumoniae strains, there was no significant clinical difference in terms of age distribution, gender, and presence of co-morbidities and metastatic infection. However, higher Pitt bacteremia score was noted in the concordant group than in the discordant group (mean, 2.7 vs. 0.1; P = 0.006). Although there was no difference of microbiological characteristics regarding K. pneumoniae isolates from the liver aspirate sample, the difference in the distribution of serotypes, the presence of virulence factors, and presence of ESBL was noted in the K. pneumoniae isolates from the stool sample. This difference was mainly due to a higher prevalence of non-K1/K2 serotype K. pneumoniae isolates in the discordant group than in the concordant group (100.0% vs. 0.0%; P = 0.006), which showed characteristics of the high rate of ESBL positivity without specific features of hvKP (Table 3).
Table 3
Comparison of characteristics between the concordant and discordant group of Klebsiella pneumoniae strains

DISCUSSION
Despite the limitations due to a small number of hvKP liver abscess patients, our results clearly showed that K1 and ST23 were the most common serotype and ST type from the liver aspirate sample of the hvKP liver abscess patients. These are consistent with a previous study conducted in the ROK,3 which showed the predominance of K1/ST23 in the K. pneumoniae liver abscess. Also, in accordance with an earlier study19 which showed more diversity of ST types in K2 serotype compared with K1 serotype, our K2 isolates had 2 ST types while all K1 isolates had 1 ST type (ST23). Additionally, distribution of the major virulence factors (rmpA, magA, and iutA) in the K. pneumoniae isolates from the liver aspirate sample in the present study were consistent with the previous studies.123 However, unlike the previous study3 which reported the mean age of 60 years and the substantial prevalence rate of DM (39.9%) for patients with K. pneumoniae liver abscess, our hvKP liver abscess patients were older (median, 71 years) with lower prevalence rate of comorbidities including DM (9.1%). Although our analysis was limited by the small numbers of patients, our results suggest that hvKP liver abscess can occur in healthy older individuals. Furthermore, the elderly are known to be more susceptible to K. pneumoniae infection due to aging-related changes in immune responses,20 and a recent increase of the detection of hvKP among K. pneumoniae isolates in the elderly has been reported in China recently.21 Given the similar epidemiologic features of hvKP liver abscess between ROK and China,123 continued epidemiologic surveillance of hvKP liver abscess in the elderly may need to be considered to define the possibly changing epidemiology of hvKP liver abscess in the ROK.
The majority of stool K. pneumoniae isolates from hvKP liver abscess patients in our study were non-K1/K2 serotypes. Moreover, we observed that the concordance rate between the liver aspirate K. pneumoniae isolates and stool K. pneumoniae isolates was low (27.3%). Additionally, discordant stool K. pneumoniae isolates did have significant heterogeneity in terms of ST types with ESBL and antibiotic resistance. These are in contrast to a previous study conducted in Taiwan10 which reported a high degree of identicalness between liver aspirate K. pneumoniae isolates and stool K. pneumoniae isolates from K. pneumoniae liver abscess patients. There are several explanations. As shown in the previous study,10 gastrointestinal colonization of hvKP is one of the predisposing factors for hvKP liver abscess. However, different rates of stool colonization of K. pneumoniae including hvKP strains among individuals were noted in the previous studies conducted in Taiwan, ROK, and China.8922 Moreover, an increasing trend of fecal carriage of ESBL-positive Enterobacteriaceae including K. pneumoniae on the global level has been reported recently.23 Extrapolating from these, it can be inferred that there might be greater heterogeneity of intestinal colonization of K. pneumoniae including hvKP strains and other K. pneumoniae strains with ESBL in the hvKP liver abscess patients. The low concordance rate between the liver aspirate K. pneumoniae isolates and stool K. pneumoniae isolates in our study supports this inference. Also, our result of the low growth rate of K. pneumoniae from the stool sample (11/37; 29.7%) of overall hvKP liver abscess patients along with the low concordance rate suggest that intestinally colonized hvKP may be able to outcompete other intestinally colonized K. pneumoniae strains with ESBL or other Enterobacteriaceae such as Escherichia coli for crossing the intestinal barrier to invade the liver. Furthermore, there was one patient whose liver aspirate culture revealed positive growth of the both ESBL-negative and ciprofloxacin-susceptible hvKP isolate and K. pneumoniae isolate with positive ESBL and sensitivity to ciprofloxacin. Although this patient was not included in the main analysis due to lack of isolation of K. pneumoniae from the stool sample, this case illustrates possible basis for the emergence of ESBL-positive hvKP liver abscess infection following co-colonization of hvKP and ESBL positive K. pneumoniae. Recent reports of increasing trends in the prevalence rates of ESBL-positive hvKP isolates in China2124 along with our case suggest possible dissemination of the ESBL plasmid into hvKP isolates, which should be monitored closely. Of note, there was a higher Pitt bacteremia score in the concordant group in our study. Whether this was representing an increased disease severity due to enhanced translocation of hvKP from a higher burden of intestinally colonized hvKP or an incidental observation is difficult to conclude but this warrants further investigation.
This study has limitations. First, this was a single-center, observational study with a small number of hvKP liver abscess patients. Thus, sampling bias from a small number of patients and K. pneumoniae isolates might have existed to affect the analysis. Second, selection bias regarding the stool K. pneumoniae isolates might have led to an underestimation of the concordance rate as the stool samples were collected after hvKP liver abscess patients had already been treated with antibiotic therapy, which might have affected the yield of the stool culture.
In conclusion, despite the aforementioned limitations, the current study suggests the significant heterogeneity of K. pneumoniae colonizing the intestinal tract of the hvKP liver abscess patients in the ROK. In the era of increasing elderly population and intestinal colonization with ESBL-positive Enterobacteriacea including K. pneumoniae, further studies involving a larger number of hvKP liver abscess patients with continuing surveillance are needed to define the changing epidemiology and the role of gastrointestinal K. pneumoniae in the hvKP liver abscess patients in the ROK.
 XML Download
XML Download