

 Citation
Citation Print
Print



INTRODUCTION
Exacerbations of chronic obstructive pulmonary disease (COPD) contribute to an increased number of COPD-related hospitalizations, increased morbidity, and mortality. Acute exacerbations account for the bulk of the financial burden related to COPD management in the long-term.1234 Hence, optimal management of exacerbations is important in reducing the COPD-related treatment burden.
Although a large number of patients are hospitalized with COPD exacerbations every year, several patients with mild to moderate exacerbation are treated on an outpatient basis. Recent studies have revealed that > 40% of patients with acute exacerbation are managed in outpatient clinics.56
Objective indicators of disease, including detailed vital signs, and laboratory and radiological data, are often difficult to evaluate in outpatient clinics due to time constraints. Furthermore, detailed assessment of patient symptoms and functional status on a daily basis is difficult in this setting. Hence, a simple tool for the objective evaluation of patients with exacerbations may be helpful for making important decisions regarding the optimization of drug therapy, hospital admission, and additional treatment.
The COPD assessment test (CAT) is a validated, eight-item questionnaire used to assess the various manifestations of COPD and quantify health status.7 It is simple and easy to complete, involves no complex calculation, and the results are immediately available.
The CAT questionnaire has been used to assess the response to pulmonary rehabilitation programs and reflects the severity of the disease.8910 In recent years, CAT score monitoring has been reported to be useful in assessing the health status and severity of COPD exacerbation.101112 A significant correlation between treatment response and changes in the CAT score was seen in a study of hospitalized patients with COPD exacerbation.13 In the most recent study, Choi et al.14 reported that the Exacerbations of COPD Tool-Patient-Reported Outcomes instrument reflects treatment efficacy during the management of an acute exacerbation; however, it has not been widely used so far.
We evaluated the association between treatment response and changes in the CAT score during COPD exacerbation in an outpatient setting. We hypothesized that changes in the CAT score during treatment of an acute exacerbation would reflect response to treatment.
METHODS
Study setting and patients
We had previously published a prospective, multicenter, double-blind, double-dummy, randomized, controlled, phase 3, non-inferiority clinical trial comparing the effectiveness of oral zabofloxacin with moxifloxacin for the treatment of outpatients with COPD exacerbations.15 The study was registered with ClinicalTrials.gov (No. NCT01658020) and the Clinical Research Information Service registry (No. KCT0000532).
In the present study, we retrospectively assessed the usefulness of CAT by dividing the patients in the original study into groups according to their therapeutic response, regardless of the type of antibiotic used. We compared the CAT scores between groups.
Patients between 40–80 years old with a physician-confirmed diagnosis of COPD exacerbation were recruited from the pulmonary outpatient clinics of 31 university hospitals between September 2012 and February 2014. The diagnosis of COPD was based on spirometry results in a stable state, in accordance with the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, which defines COPD as a post-bronchodilator forced expiratory volume in one second to forced vital capacity ratio of < 0.7.16 According to the symptom-based definition by Anthonisen et al.17 and the GOLD guidelines,16 COPD exacerbation was defined as an acute worsening of two or more major respiratory symptoms (dyspnea, sputum volume, or sputum purulence) for 2 consecutive days that warranted a change in the patient's daily medication. Patients with asthma, those with any other active respiratory disease requiring treatment, and those with any other severe, uncontrolled comorbidities were excluded.
Patient self-reported symptoms and demographic and clinical data were documented at the beginning of the study. Sputum samples were also obtained before the initiation of treatment for the exacerbation. We noted respiratory symptoms, including dyspnea and volume/purulence of respiratory secretions. The degree of purulence was categorized as follows: 0, similar to a stable state; 1, mucoid (clear mucoid, like egg white); 2, mucopurulent (mucoid with a thick and purulent consistency [≤ 50% pus]); and 3, purulent (mostly purulent, with yellow or green, thick pus [≥ 50% pus]). To facilitate understanding, patients were provided with a sputum color chart and were asked to make the appropriate selection. The detailed scoring of respiratory symptoms is described as supplementary data (Supplementary Table 1).
Exacerbation assessment
Patients were examined by a board-certified specialist in respiratory medicine who made the diagnosis of a COPD exacerbation. Treatment was administered according to the GOLD guidelines, based on physician judgment. Treatment could include an increased dose of inhaled therapy or an oral steroid, or a combination of both. Patients received either zabofloxacin (367 mg once daily for 5 days) or moxifloxacin (400 mg once daily for 7 days) based on the original study protocol that aimed to confirm the efficacy and safety of zabofloxacin, a new fluoroquinolone antibiotic.
Patients were followed up at the hospital at 5 (visit 2), 10 (visit 3), and 36 (visit 4) days after the day of enrollment (visit 1). During each visit, changes in respiratory symptoms, primarily the degree of dyspnea, sputum volume/purulence, were evaluated by clinicians.
Clinical assessment
In accordance with the symptom-based definition of COPD exacerbation mentioned above, the therapeutic response was noted at visit 3 (day 10). On the basis of changes in respiratory symptoms, patients were classified as responders or non-responders. A responder was defined as a patient who showed an improvement by more than one grade both in dyspnea and sputum volume/purulence relative to the findings at the time of enrollment. If any of the symptoms remained unchanged or had aggravated, the patient was defined as a non-responder. Non-responders were treated with additional antibiotics until symptomatic improvement was observed.
CAT questionnaire
The CAT questionnaire was completed by patients daily at home from the initial visit until visit 2 on day 5. Subsequently, the questionnaire was completed in the presence of a physician on days 10 (visit 3) and 36 (visit 4). The questionnaire comprises eight items reflecting respiratory symptoms, wellness, and activities of daily living.18 Each item is scored from 0 to 5 (overall score range, 0–40), with higher scores indicating worse health status.
Statistical analysis
Comparisons between groups were assessed using the Student's t-test or the Mann–Whitney test for continuous variables and the χ2 test or the Fisher's exact test for categorical variables. Repeated measures analysis of variance with the Tukey's B post hoc test was applied to evaluate changes in the CAT score according to the duration of treatment. Multivariate logistic regression analysis was performed to evaluate the relationship between changes in clinical parameters during the management of an exacerbation and the therapeutic response. The results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). Data are expressed as means ± standard deviations for continuous variables and frequencies for categorical variables. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 18 for Windows (SPSS Inc., Chicago, IL, USA). A P value of < 0.05 was considered statistically significant.
Ethics statement
The study protocol was approved by the Institutional and Review Board (IRB) at each center before the commencement of the study and Konkuk University Hospital (IRB No. KUH1010970). All participants were fully informed about the study and provided written informed consent before data collection.
RESULTS
We enrolled 345 patients with COPD exacerbation; 48 were excluded because they did not meet the inclusion criteria, provided insufficient information for analysis, or withdrew consent. The remaining 297 patients were included in the study. On the basis of the therapeutic response on day 10, 258 patients were classified as responders and 39 as non-responders (Fig. 1).

The study subjects were predominantly men, and approximately 80% experienced moderate to severe COPD. There was no significant difference in baseline characteristics between responders and non-responders (Table 1). At the time of enrollment, > 60% of all patients experienced moderate dyspnea, while 15%–20% experienced severe dyspnea. The sputum was mucopurulent in 46% and purulent in 33%–34% of patients (Table 1).
Table 1
Demographics and clinical characteristics of patients

Data are presented as mean ± standard deviation or number (%).
BMI = body mass index, GOLD = Global Initiative for Chronic Obstructive Lung Disease, FEV1 = forced expiratory volume in 1 second, FVC = forced volume capacity, SABA = short-acting beta agonist, LABA = long-acting beta agonist, LAMA = long-acting muscarinic antagonist, ICS = inhaled corticosteroid, PDE4 = phosphodiesterase 4.
aResponders were defined as patients demonstrating an improvement in dyspnea and sputum purulence and volume on day 10; bHypertension, coronary artery disease, diabetes mellitus, cerebral infarction; cOn the first day of exacerbation.
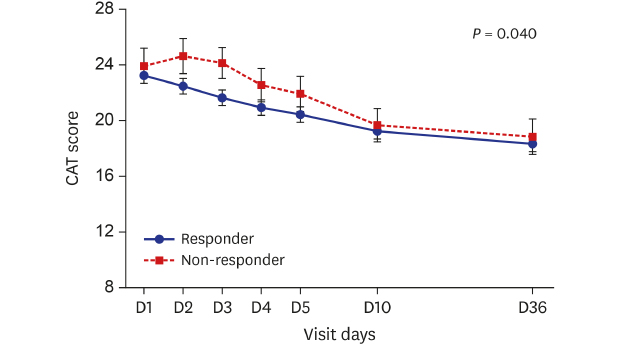
Fig. 2 illustrates changes in the CAT score according to the treatment in the two groups. The mean CAT score of all patients was 23.4 ± 7.4 on the first day, 20.72 ± 7.8 on day 5, and 18.34 ± 7.9 on day 36. During the first 5 days after treatment, the CAT score decreased more rapidly in the responder group compared to the non-responder group. In the responder group, the CAT score decreased by more than 2 points, which is considered a minimum clinically important difference (MCID), on day 4 (23.3–20.5 vs. 23.5–22.0; P = 0.04).19 An increase in the CAT score was observed during the first 3 days after treatment in the non-responder group. The detailed scores are presented in Supplementary Table 2.
Fig. 2
Time course of CAT scores in both groups.
CAT = chronic obstructive pulmonary disease assessment test.
In addition, we compared clinical characteristics to patients who improved by more than 2 points (CAT-Improved) and those who did not (CAT-Unimproved) following the CAT score change on day 4 (Supplementary Table 3). Unlike the treatment response classification, patients with improved CAT scores of 2 or more on day 4 had significantly lower disease severity at the time of registration (severe + very severe group; 51.6% vs. 68.6%; P = 0.04), lung function also showed no statistical significance, but showed a better tendency. Interestingly, patients in the CAT-Improved group tended to have more severe respiratory symptoms (dyspnea, respiratory secretions) at time of enrollment than patients in the CAT-Unimproved group, but they were nearly similar or better when compared to day 5 of treatment (visit 2).
Multivariate logistic regression analysis revealed that the improvement in the CAT score during the first 3 days after treatment was associated with the therapeutic response (adjusted OR, 1.35; 95% CI, 1.01–1.391; P = 0.043) (Table 2). The initial CAT score after enrollment and the changes during 5 days of treatment revealed a weaker, statistically non-significant correlation. There was a significant association between the alleviation of respiratory symptoms and the therapeutic response (dyspnea: adjusted OR, 5.509; 95% CI, 2.326–15.242; P < 0.001; sputum: adjusted OR, 3.561; 95% CI, 1.62–8.907; P = 0.003).
Table 2
Correlation between CAT scores, dyspnea, respiratory secretions, and treatment response

CAT = chronic obstructive pulmonary disease assessment test, OR = odds ratio, CI = confidence interval, Δ = delta change, FEV1 = forced expiratory volume in 1 second.
aCorrected for age, sex, smoking status, exacerbations in the previous year, type of antibiotics, and post-FEV1% predicted; bOn the first day of exacerbation.
The mean overall CAT score was lower and revealed a more rapid recovery pattern in the responder group compared to the non-responder group. In particular, scores in the cough, sputum, and breathlessness domains revealed rapid recovery. The responders showed a significant decrease in scores in the domains of sputum, chest tightness, and activities of daily living. Non-responders demonstrated an increase or a minimal decrease in scores in the confidence, sleep, and energy domains (Fig. 3).
Fig. 3
Change of CAT scores during follow-up.
CAT = chronic obstructive pulmonary disease assessment test.

The overall change in the CAT score according to the severity of COPD is presented in Fig. 4, and details are provided in Supplementary Table 4. The mean CAT score was higher in patients with more severe disease throughout the study. In the responder group, the CAT score for all patients revealed a significant decrease over time (P < 0.01). Patients with very severe COPD demonstrated significantly higher mean CAT scores than those with lower degrees of severity on day 1 (mild, 19.8 ± 6.2; moderate, 21.4 ± 7.8; severe, 23.8 ± 6.5; very severe, 28.6 ± 7.2). This difference was observed throughout the treatment period. The CAT scores recovered gradually in patients with more severe disease (Fig. 4A). In the non-responder group, the overall CAT scores for patients with moderate and severe COPD decreased during the treatment period (P = 0.8). In non-responders with very severe COPD, the CAT scores increased over time (Fig. 4B).
Fig. 4
Change in the mean CAT score based on the severity of disease. (A) Change in the mean CAT scores among responders. (B) Change in the mean CAT scores among non-responders. Severity of disease was classified according to the GOLD criteria.
CAT = chronic obstructive pulmonary disease assessment test, GOLD = Global Initiative for Chronic Obstructive Lung Disease.

DISCUSSION
In the present study, we found that CAT scores decreased more rapidly in patients with a good therapeutic response. A decrease in CAT scores during the first 3 days of treatment was associated with a favorable outcome.
Treatment of exacerbations is a vital component of COPD management. Early treatment improves the recovery rate, lowers the risk of hospitalization, and reduces the cost of care.20 Monitoring of the therapeutic response can be helpful with the establishment and re-evaluation of the treatment plan.
CAT is a well-established test that correlates with disease-related health status.18212223 Several recent studies have suggested that the change of CAT score may reflect treatment efficacy during COPD exacerbation.131424
In the present study, we observed a weak correlation between treatment response and change in CAT scores during the early stage of treatment. A stronger association was observed between respiratory symptoms (dyspnea, respiratory secretions) and treatment response; however, this association resulted from the definition of treatment response, which included dyspnea, sputum volume, and purulence. Besides being an indicator of respiratory symptoms, the CAT scores may also reflect exercise capacity, quality of life, and psychological state.7252627 Hence, CAT scores may be more useful in determining the overall condition of the patient in a clinical setting.
The prognosis of COPD exacerbation depends on various factors, including age, disease severity, comorbidities, and sociomedical support. These factors could account for the weak relationship we observed in the present study.28 However, considering the lack of a standard tool for predicting and monitoring treatment response in these patients, the CAT score deserves full consideration. Future studies with a larger sample size may be helpful for assessing the usefulness of CAT in the evaluation of treatment response.
We also demonstrated that the 4-day decline in the CAT score was more than 2 points, which is considered the MCID919 and patients who improved more than 2 points on day 4 were found to have recovered rapidly although the respiratory symptoms were not good at the time of enrollment.
Among responders, the decrease was more than 2 points in 47.2% of patients on day 3 and 53.5% of patients on day 4. In the non-responder group, a 2-point decrease was observed in 27.2% of patients on day 3 and 33.4% of patients on day 4. The MCID in the CAT score has not been well established so far, and it remains unclear whether there is a significant decline in cases of COPD exacerbation. In a European CAT validation study, the difference in the score between exacerbation and stable disease was 4.1 points, and Mackay et al.10 reported an overall change in score of 4.7 points.23 In contrast, a study by Jone et al.8 showed that a decrease of 2.6 points over a period of 14 days in patients who responded to treatment could be considered MCID during exacerbation management. Similarly, a recent report proposed a decrease in score of 2 units or more.24 The results of our study support the hypothesis that a relatively small change in the CAT score may be clinically significant in patients with exacerbation.
Our results, consistent with those from previous studies,1224 indicate that disease severity was strongly correlated with a change in the CAT score, with greater disease severity resulting in higher initial CAT scores and worsening the recovery rate. Although the disease severity did not adequately reflect the health status, airway limitation affected the health status of patients and worsened the long-term prognosis by adversely affecting recovery from exacerbations. Interestingly, patients with very severe disease in the non-responder group had lower CAT scores than those with moderate or severe disease on day 1. However, the scores increased over time. A possible explanation for this finding is that patients with very severe disease are relatively insensitive to adverse changes in baseline symptomatology during the stable phase. However, due to slow recovery, treatment satisfaction decreases with an increase in CAT scores over time. Hence, the CAT score may be less useful in some patient subgroups, including those with very severe COPD, and clinicians should exercise caution while interpreting the results.
As expected, we confirmed that the scores in the cough, sputum, and breathlessness domains reflect the therapeutic response in patients with exacerbation. In the non-responder group, chest tightness and breathlessness showed a slow recovery pattern, whereas parameters pertaining to emotional aspects, including confidence, sleep, and energy, worsened relative to their status at baseline. Our results concur with a previous report29 and suggest that symptom-related domains reflect the treatment outcome in the acute phase, while emotional factors affect the long-term outcome of treatment of COPD exacerbations. When considering the clinical aspects of care in patients with COPD exacerbations, the emotional aspect tends to be neglected. Our results suggest that emotional factors are important during the management of an exacerbation.
Our study has several limitations. First, we did not document respiratory symptoms and baseline CAT scores when patients were stable. Hence, we could not determine whether the acute symptomatic worsening and CAT scores returned to baseline levels during the study period. However, CAT scores in previous studies2429 generally recovered over a 1-month period; hence, we believe that our results are valid. Second, our study was retrospective and post-hoc by design; we could not include objective parameters including changes in lung function, cost of care, and the duration of treatment to assess the correlation with CAT. Future studies including these parameters are required. Finally, our sample size was small, particularly among non-responders. Therefore, our results could have been influenced by limitations in data collection and interpretation.
In conclusion, the findings of the present post-hoc study suggest that there is a correlation between changes in CAT scores and treatment response in patients with COPD exacerbation. In particular, changes during the first 3 days of treatment determine whether outcomes are favorable. Our findings suggest that the routine application of CAT in the management COPD exacerbation can help improve treatment outcomes.
 XML Download
XML Download