

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The Republic of Korea stipulates that local emergency medical centers are designated and deployed nationwide to provide emergency medical services to the community and that patients who cannot be managed by local emergency medical centers should be treated at regional emergency medical centers [1]. The total number of emergency department (ED) visits was 10,445,829 in 2017, which is one-fifth of the total population [2]. There are various reasons to visit ED; among them, abdominal pain is the main reason, accounting for 6~23%[345]. Abdominal pain can be caused by a wide range of disorder including trauma, infectious or non-infectious diseases, vascular diseases, metabolic diseases, and lead poisoning [678]. Depending on the disease, the duration, location, intensity, and pattern of the abdominal pain are different, and various accompanying symptoms may occur [69].
Diseases that causes abdominal pain can be categorized as, excluding trauma, urgent diseases or non-urgent diseases [101112]. Urgent diseases such as gastrointestinal tract infection which was more likely to develop into a septic shock [13] and to be life-threatening [11] must be diagnosed and treated within 24 hours; on the other hand, non-urgent diseases don't require urgent treatment and tend to be self-limiting. However, the majority of patients who visit ED with abdominal pain (64~83%) were discharged from ED [36], so, there have been previous studies about clinical diagnosis that divide urgent and non- urgent diseases using medical history taking, physical examination, blood test, and simple X-ray results, additional tests should be conducted only in case of suspected urgent diseases. They claimed the clinical diagnosis with or without plain radiographs had a high sensitivity [101415].
However, in most EDs, triage nurses conduct an initial assessment and determine the order of seeing a doctor [16]. Their decisions affect doctors' judgment, so, it is necessary to identify the relating factor to urgent disease among the information collected by triage nurses. None the less, most of the previous research included related factors that are not available in the triage [10] or identified factors related to hospitalization without distinction between urgent diseases and non-urgent diseases [1718]. Thus, this study was intended to identify the relevant factors to urgent diseases among information obtained by the nurse of triage.
METHODS
1. Study Design
This study is a retrospective descriptive study to identify the relevant factors of urgent diseases to cause abdominal pain.
2. Setting and Subject
The study institution was a regional emergency medical center located in Seoul metropolitan city with an average of 70,000 ED patients per year. Subjects were all patients aged 19 and older who visited the ED with abdominal pain from September 1, 2017 to October 15, 2017. During the study period, a total of 6181 patients visited the emergency department. Patients with obvious cause such as trauma, full-term pregnancy, tube malfunction were excluded. Patients with impaired consciousness and patients who entered the resuscitation room immediately were also excluded because they could not express detailed symptoms. The 573 patients were included in the final analysis, excluding 158 patients.
3. Data Collection
Data were collected from the electronic medical records by one researcher who was not responsible for triage.
Sex, age, route of visit and mode of arrival and vital sign were collected because they reported as relating factors to hospitalization, surgery or the type of diagnosis in previous studies [3101718]. Blood pressure was classified as hypertension (systolic pressure ≥140 mmHg or diastolic pressure ≥100 mmHg) and hypotension (diastolic pressure ≤90 mmHg). The pulse was classified as tachycardia more than 100 times per minute and bradycardia less than 60 times per minute. Body temperature greater than 38℃ was classified as fever and body temperature less than 35℃ was hypothermia [1920].
Abdominal pain can be caused by a wide range of disorder and show the various accompanying symptoms [6789], we collect data about underlying disease, surgery history, and accompanying symptoms such as poor oral intake, indigestion, abdominal distension, nausea, vomiting, diarrhea, constipation. We excluded symptoms that indicated the clear pathological causes such as hemorrhage and jaundice. The pain was investigated for three attributes: duration of pain, pain intensity measured using numeric rating system, location of pain.
The final diagnosis was collected from discharge medical records. We divided final diagnoses into urgent disease and non-urgent disease. Urgent disease refers to a condition that, if delayed in diagnosis and treatment, is likely to affect survival or cause disability [11]. In previous studies, the categories of urgent disease and non-urgent disease groups were often classified by referring to mortality by cause of death, with slight differences in literature. World society of emergency surgery study group [21] classified incarcerated hernia, perforated viscus, diffuse peritonitis, abscess, appendicitis, and cholecystitis as urgent disease. Laméris et al. [10] and Stewart et al. [11] classified perforated viscus, intestinal bleeding, acute cholecystitis, complicated diverticulitis, ovarian torsion, ectopic pregnancy, acute mesenteric ischemia as urgent disease [1011]. The Ministry of Health and Welfare of Korea listed urgent disease groups by referring to the annual mortality rate for each cause of death [22]. urgent disease that can cause abdominal pain are gallbladder and bile duct disease, peritonitis, intestinal perforation, intra-peritoneal cavity abscess, gastrointestinal bleeding, poisoning, intussusception, bowel obstruction.
In this study, the urgent diseases included acute appendicitis, acute diverticulitis, bowel obstruction, acute cholecystitis, acute pancreatitis, ovarian torsion, pelvic inflammatory disease, bleeding/ruptured ovarian cyst, renal and ureteral stones with obstruction, hydronephrosis, pyelonephritis, intra-abdominal abscess, retroperitoneal abscess, hepatic abscess, tubo-ovarian abscess, perforated viscus, bowel ischemia, retroperitoneal or abdominal wall bleeding, acute peritonitis.
4. Ethical Consideration
Personal identification information and data were separated by matching the patient's registration number and name with serial number. Passwords were assigned to the computers and files where all the data was stored, making it impossible for others to access them. The study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No.: H-1710-018-890) and exempted from the consent because there was little harm to the patient by retrospective review of the data collected during the routine care process.
5. Data Analysis
The distributions of the demographics and clinical characteristics were presented using descriptive statistics. Duration of pain was excluded from analysis due to too wide variance and vague answer. A comparison of the categorical variables between the two groups was conducted using a χ2 test or Fisher's exact test; continuous variables using independent t-test or Wilcoxon rank sum test. Characteristics with a p-value < 0.2 in the univariable analysis were considered as candidate factors for the multivariable model. The backward elimination method was used for the final multivariate model, with the criteria for removing variables at each stage set to 0.05. Meanwhile, at least 10 events per variable are needed to get a valid logistic model [23]. In this study, there were 17 explanatory variables used in the analysis, so the number of patients should be around 170. Since there were 173 patients in the urgent disease group (UDG) and 400 patients in the non-urgent disease group (NUDG), the sample size of this study was reasonable to have a valid model.
RESULTS
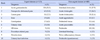
A total of 573 patients met the inclusion criteria, of which 173 patients (30.2%) had an urgent disease. In the UDG, the number of intestinal obstruction patients was the highest, followed by acute cholangitis, and acute cholecystitis. In the NUDG, acute gastroenteritis was the largest, followed by non-specialized abdominal pain and cancer pain (Table 1).
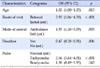
The mean age of the UDG was about 6 years higher than NUDG. In UDG, the ratio of referred patients from other clinic and ambulance utilization was significantly higher. In UDG, pain intensity was higher and the abdominal distension was more common. In NUDG, diarrhea was more common (Table 2).
In the multivariate analysis, sex, age, route of visit, mode of arrival, underlying disease, pain intensity, diarrhea, abdominal distension, pulse, blood pressure, and body temperature variables were included. Underlying disease through backward elimination was first excluded from the model, followed by sex, body temperature, and pain intensity. In the final model, age, mode of arrival, diarrhea, and tachycardia variables included (Table 3). Meanwhile, variance inflation factors among variables included in the final model were less than 1.1, which implies there's no issue with multicollinearity in our final model.
DISCUSSION
About 30.2% of patients who visited the ED with abdominal pain were classified as urgent diseases. The factors related to urgent diseases were identified as higher age, referral from other clinics, ambulance utilization, tachycardia, and no diarrhea.
To the best of the researcher's knowledge, the only study to report the rate of urgent diseases was the study of Laméris et al [10]. Other similar studies reported that the admission rate was 17~49%, but in these studies, the diagnosis for admission included non- urgent diseases such as cancer pain [3617]. Laméris et al. [10] reported that the proportion of urgent diseases was 65%, which is thought to be due to the significantly higher proportion of referral (83%) than this study (19.4%). This suggestion was consistent with the result that referral from other clinics was the relating factor to urgent diseases. Therefore, it is thought necessary to pay attention to the patients who are transferred from other clinics to a regional emergency center.
We found that the probability of an urgent disease increased by 1.03 times as the age of one year. Age was a significant predictor of the surgical diagnosis and admission [172425], higher urgency and longer length of stay in ED [26]. The clinical symptoms of elderly patients tend to be vague [17] and more complex [25]. Therefore, elderly patients with abdominal pain need to be concerned closely even if there are no other risk factors.
Even though previous studies reported that the severity of ambulance users was higher, performed more tests in the ED, and stayed longer [2627], there have been concerns in Korea that the use of ambulance may be inappropriate because paramedics cannot reject patients and ambulance is free. In this study, patients who used ambulances tend to have a higher severity. However, because patients referred from another clinic had a high incidence of urgent diseases and the high utilization of ambulance, attention should be paid to interpretation.
Among the sign and symptoms, only tachycardia and no diarrhea were related to urgent diseases. The most common finding of sepsis among patients visiting the emergency room was a tachycardia, and even if not sustained [1318]. Therefore, it is very important for nurses to accurately measure vital signs, especially pulse, and understand its meaning. Most of acute diarrhea which lasts from hours to days [28] is caused by a virus infection and is normalized by itself [2930]. The acute gastroenteritis (AGE) is the most common disease in NUDG in this study. AGE is defined as acute diarrhea with or without symptoms such as nausea, vomiting, fever, and abdominal pain [31]. So, diarrhea was identified as the relating factor to non-urgent diseases. However, diseases such as appendicitis, pneumonia, and urinary tract infections can also cause diarrhea, thus it is necessary to explain to revisit ED if diarrhea does not improve [32].
On the other hand, we found that the intensity of pain is not related to urgent diseases. The degree of pain perception, even if it is caused by the same disease, can vary due to multiple factors, including sensory, emotional, cognitive, and behavioral factors [33]. Therefore, patients with mild pain should not be treated as not severe patients, nor should the administration of pain killers to patients with severe pain be delayed for worry about missing diagnosis for urgent diseases.
This study is meaningful in that we confirmed the factors to consider in triaging as soon as the patients with acute abdominal pain visit ED. However, this study has several limitations. First, this study was conducted retrospectively in a single ED, so generalization of findings is needed to be careful. Second, the possibility that the diagnosis is changed and if the member did not revisit the study institution could not be excluded. Lastly, because surgical and medical emergency diseases are completely different in their treatment methods and outcomes when not treated, it is very important to distinguish surgical and medical emergency diseases [1121] However, because the number of surgical emergency cases is too small, we could not identify the relating factors to surgical emergency diseases separately in this study. Multi-institute research is needed to secure the number of surgical emergency patients and identify the relating factors to a surgical emergency.
CONCLUSION
The factors related to urgent diseases were identified as higher age, referral from other clinics, ambulance utilization, tachycardia, and no diarrhea. It is necessary to triage and treat the patients who are transferred from another hospital or visit by ambulance more quickly. And, it is important for triage nurses to check for tachycardia or diarrhea symptom through accurate history taking, especially when triaging an elderly patient whose symptoms may be ambiguous. Additionally, based on the findings, we suggest that researches to use a broader range of data such as NEDIS information to reaffirm the factors that can predict urgent disease. It is necessary to develop screening tools that can predict urgent diseases based on the evidence and use them as training materials for the triage nurses.

 XML Download
XML Download