

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Intraoral haemorrhage as a result of a dental procedure or trauma may cause life-threatening complications, such as airway obstruction or hypovolemic shock123. Therefore, rapid haemostasis may be needed. The most common haemostasis method used for intraoral bleeding is local compression. If this method fails, additional local haemostatic measures, such as suturing, can be applied. Aggressive systemic intervention, i.e., transfusion of blood products, ligation of the causative vessel(s), or embolisation, may also be necessary45.
Systemic factors that can increase the risk of intraoral haemorrhage include antithrombotic agents, hepatic cirrhosis, leukaemia, and inherited bleeding disorders. Local risk factors include highly invasive surgery, extensive soft tissue trauma during surgery, and inflammation at the surgical site. The methods used to prevent postoperative haemorrhage are well known6789. However, most studies have focused on preoperative adjustment of doses of antithrombotic agents. Although there have been some systematic reviews of haemostasis in patients with clinically significant bleeding10, such as delayed or secondary haemorrhage, these reviews only mentioned that minor bleeding events were well controlled by local haemostatic measures, regardless of preoperative adjustment of oral anticoagulant therapy1112. There has been no research on factors associated with an increased need to use more than local compression to achieve haemostasis1314.
The aims of this study were to determine the effectiveness of local compression in patients visiting the emergency room with intraoral haemorrhage and to identify patients in whom a haemostatic method other than local compression may be required.
II. Materials and Methods
The medical records of all patients who visited our institution with intraoral haemorrhage were retrospectively reviewed during the period from January to June 2019. The inclusion criterion was admission to the Emergency Department either with gingival haemorrhage (K0688) or oral haemorrhage (K137) according to the International Statistical Classification of Diseases and Related Health Problems 10th revision (ICD-10) between 2010 and 2018. The exclusion criteria were intraoral haemorrhage originating from a site other than the oral cavity proper and uncertainty regarding antithrombotic treatment. Two oral and maxillofacial surgeons (J.B.S. and Y.S.H.), each with at least 3 years of experience, evaluated the clinical parameters; if necessary, consensus was reached by discussion. All data collected were checked for missing values and outliers.
The study protocol was approved by the Institutional Review Board of Seoul Metropolitan Government-Seoul National University Boramae Medical Center (approval No. 10-2019-23) and conducted according to the tenets of the 1964 Declaration of Helsinki and its later amendments. The need for informed consent was waived in view of the retrospective nature of the study and the anonymity of the data.
1. Haemostasis protocol and clinical setting
The need for haemostasis in a patient who arrives with intraoral haemorrhage in our Emergency Department is determined by an emergency physician with more than 2 years of experience. If haemostasis is deemed unnecessary, medical support is provided and the patient is discharged after an hour of observation. If haemostasis is necessary, local compression using a small amount of sterile gauze is applied to the site of the haemorrhage for an hour. Blood tests are only performed when deemed necessary by the emergency physician. An oral and maxillofacial surgeon with at least 2 years of clinical experience is called to perform haemostasis if local compression fails. Depending on the cause and location of the haemorrhage, control measures may include application of a local haemostatic agent, sutures, and bipolar or monopolar electrocautery. If the haemorrhage is associated with a mobilised tooth affected by chronic periodontitis, the causative tooth is extracted and a local haemostatic measure is applied. Local haemostatic agents used during the study period included a gelatine sponge (Cutanplast Dental; Curesys, Seoul, Korea), an absorbent collagen dressing (Ateloplug; TRM Korea, Seoul, Korea), and oxidised regenerated cellulose (Surgicel Original; Ethicon, Somerville, NJ, USA). Suturing was performed using non-absorbable uncoated polyamide (Dafilon 4/0; B Braun Surgical SA, Barcelona, Spain). If necessary, these local methods were supplemented by a 500-mg intravenous injection of tranexamic acid (Shinpoong Pharmaceutical, Seoul, Korea) or transfusion of fresh frozen plasma or packed red blood cells. After confirmation of haemostasis, the patient was discharged after an hour of close observation.
2. Study variables
The study outcome was whether or not a simple or complex haemostatic method was needed to achieve haemostasis. The haemostasis method was defined as simple if no treatment or only local compression was required or complex if application of a local haemostatic agent, sutures, electrocautery, extraction of a causative tooth, or intravenous administration of tranexamic acid or blood products was needed. Local compression was defined as simple direct local compression only with a small piece of sterile gauze applied to the site of haemorrhage. When more than one method was used for local haemostasis, the final method used was recorded. The intervention was recorded as systemic if intravenous blood products were administered regardless of whether or not a local haemostasis method was used. Potential predictive variables included sex, age, American Society of Anesthesiologists (ASA) class, hepatic cirrhosis, bleeding disorder, history of antithrombotic treatment, and site and cause of haemorrhage.
3. Statistical analysis
Continuous variables were analysed using the Student's t-test or Mann-Whitney U test according to the Kolmogorov-Smirnov test for normality assumption, and categorical variables were analysed using the Pearson's chi-square test or Fisher's exact test. Multivariable logistic regression with backward elimination was performed for variables that were found to be statistically significant in univariable logistic regression analyses. The final model was selected based on the Akaike information criterion. The Hosmer-Lemeshow test was performed to assess goodness-of-fit for the final fitted model. All statistical analyses were performed using IBM SPSS Statistics for Windows (ver. 20.0; IBM, Armonk, NY, USA). A P-value <0.05 was considered statistically significant.
III. Results
1. Patient characteristics in the simple and complex haemostasis groups
Six hundred eight patients who met the inclusion criteria were screened against the exclusion criteria, after which 540 were eligible for inclusion in the study. Eighty-four patients required a complex haemostasis method. The most common method used was local compression (68.1%), followed by local haemostatic agents, sutures, systemic blood products, bipolar or monopolar electrocautery, and extraction of a causative tooth. Eighty-eight patients did not require treatment for haemostasis.(Fig. 1) Excluding patients in whom no treatment was administered, local compression alone was adequate for haemostasis in 81.4% of cases. Intravenous tranexamic acid was administered in five cases and packed red blood cells or fresh frozen plasma in four. Two of these four patients were receiving warfarin, one at a dose of 6.5 mg once daily and the other at a dose of 4.0 mg once daily. The platelet counts in these patients were 221,000 and 157,000/µL, respectively, with respective prothrombin time-international normalised ratio (PT-INR) values of 4.38 and 6.60. The remaining two patients were not taking antithrombotic agents; one had idiopathic thrombocytopenic purpura (platelet count, 50,000; PT-INR, 1.01) and the other had alcoholic liver cirrhosis (platelet count, 77,000; PT-INR, 1.27). No invasive procedures, such as embolisation of the affected blood vessels, were required in the emergency room.
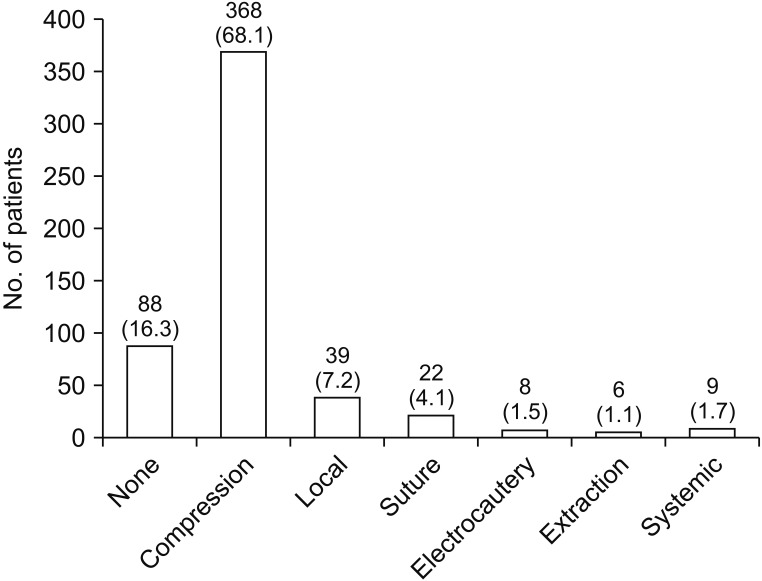
Fig. 1
Method of haemostasis used for intraoral haemorrhage. The values are presented as the number (%). (None: no treatment, Compression: simple direct local compression only with a small piece of sterile gauze applied to the site of haemorrhage, Local: local haemostatic agent, Electrocautery: bipolar or monopolar electrocautery, Extraction: extraction of causative tooth, Systemic: systemic administration of tranexamic acid or blood products)
![]()
The general characteristics of the simple and complex haemostasis groups are summarised in Table 1. The mean age was 48.9 years (range, 1-93 years), and 53.5% were male. ASA class II or higher systemic disease was present in 231 cases, hepatic cirrhosis in 17 cases, and a bleeding disorder (thrombocytopenic purpura) in 2 cases. One hundred and twenty-eight patients were receiving antithrombotic agents. The antiplatelet agents used were aspirin, clopidogrel bisulphate, cilostazol, and triflusal; and the anticoagulants used were warfarin, apixaban, and dabigatran.(Supplementary Table S1) Whether or not the antithrombotic agents were discontinued before the dental procedures were performed is unclear; however, all patients on antithrombotic agents were taking these medications at the time of their emergency room visit.

Table 1
Description of risk factors according to whether a simple or complex method of haemostasis was used for intraoral haemorrhage
![]()
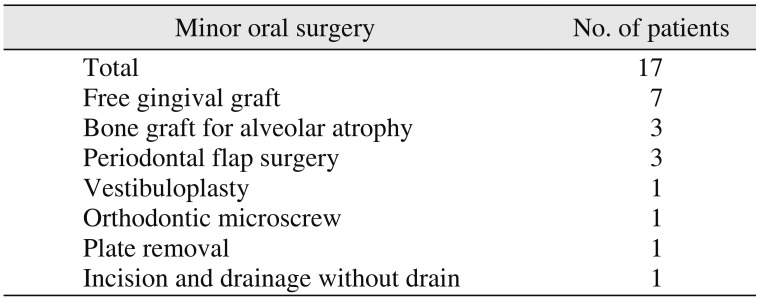
The most common site of haemorrhage was the gingiva (91.7%), followed by the buccal mucosa, tongue, palatal mucosa, and lip.(Fig. 2) The simple and complex haemostasis groups are compared according to the cause of haemorrhage in Fig. 3. The most common cause of haemorrhage was tooth extraction (45.7%), followed by installation of a dental implant fixture, trauma, local inflammation caused by periodontitis, basic periodontal treatment, minor oral surgery (excluding tooth extraction and installation of a dental implant), intraoral insertion of a Penrose drain, and cancer. The specific types of minor oral surgery performed are described in Table 2. In a further 3 cases, spontaneous bleeding was caused by idiopathic thrombocytopenic purpura, mucosal abrasion by severe xerostomia, and eruption of a permanent tooth, respectively.
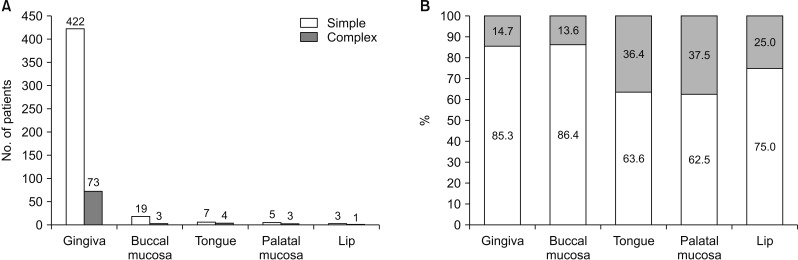
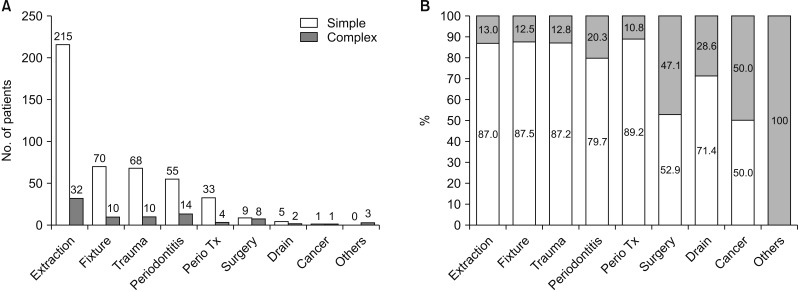
Fig. 2
A. Number of patients. B. Percentile of patients. Comparison of cases stratified by whether or not a simple or complex method of haemostasis was performed according to the site of haemorrhage. P=0.169, univariable logistic regression test. The values are presented as the number or percentile. (Simple: simple method of haemostasis, Complex: complex method of haemostasis)
![]()
Fig. 3
A. Number of patients. B. Percentile of patients. Comparison of cases stratified by whether or not a simple or complex method of haemostasis was performed according to the cause of haemorrhage. P=0.019, univariable logistic regression test. Values are presented as the number or percentile. (Simple: simple method of haemostasis, Complex: complex method of haemostasis, Extraction: tooth extraction, Fixture: installation of a dental implant fixture, Trauma: physical trauma to tooth or gingiva, Periodontitis: local inflammation caused by periodontitis, Perio Tx: basic periodontal treatment including scaling or subgingival curettage, Surgery: minor oral surgery excluding tooth extraction and dental implant surgery, Drain: intraoral Penrose drain insertion, Cancer: oral cancer)
![]()
2. Factors affecting the haemostasis method used
Univariable logistic regression analysis revealed significant associations of use of a complex haemostasis method with older age, ASA class II or higher systemic disease, and use of an antithrombotic agent. A complex haemostasis method was used more often after minor oral surgery than after tooth extraction.(Table 3) Multivariable logistic regression analysis revealed significant associations between the need for a complex haemostasis method and use of an antithrombotic agent and minor oral surgery.(Table 4)
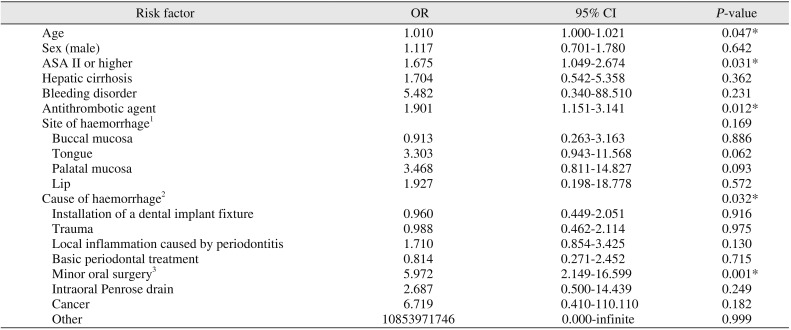
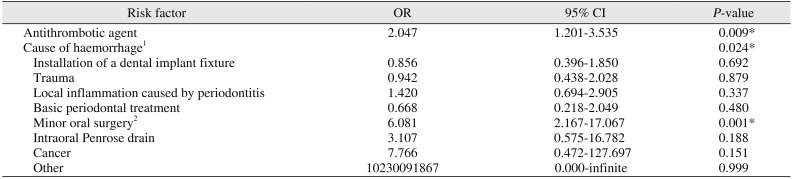
Table 3
Results of univariable logistic regression analysis of factors associated with the need for a complex method of haemostasis for intraoral haemorrhage
![]()
Table 4
Results of multivariable logistic regression analysis of factors related with the complex method of haemostasis for intraoral haemorrhage
![]()
IV. Discussion
The most straightforward haemostatic method used for intraoral bleeding is local compression. However, a more complex method is needed if this is ineffective, which entails additional cost and time consumption. Complex methods include local haemostatic agents, suturing, electrocautery, extraction of the causative tooth, and systemic administration of tranexamic acid or blood products. Local haemostatic methods include application of a gelatine sponge, absorbent collagen dressing, or oxidised regenerated cellulose. This study aimed to determine the effectiveness of local compression in patients presenting to the emergency room with intraoral bleeding and to assess the risk factors prompting a more complex approach. Local compression was usually sufficient for haemostasis. Use of a complex haemostatic approach was associated with use of an antithrombotic agent and minor oral surgery, such as a free gingival graft, alveolar bone graft, or periodontal flap surgery.
Various local haemostatic methods have been used in dentistry. Most cases of intraoral haemorrhage can be controlled successfully by local haemostatic methods with or without suturing41516. In the present study, 39 of 84 patients requiring a complex haemostasis method were successfully treated with local haemostatic agents. Other cases were controlled with alternative local measures, including sutures, electrocautery, and extraction of the causative teeth. However, in 9 of the 540 cases in this study, local haemostasis methods failed and intravenous administration of tranexamic acid or blood products was required. Four patients who required transfusion had a PT-INR ≥4 at the time of bleeding or had severe systemic disease. In all 9 cases, use of a systemic haemostasis method was successful and without complications.
In previous studies, use of a local haemostatic agent, such as oxidised regenerated cellulose, was more effective than local pressure alone for controlling bleeding after surgery in the palatal region, such as a free gingiva graft1718. In our study, a complex haemostasis method was more likely if the haemorrhage involved the tongue, palate, or lips than the gingival and buccal mucosa. This finding might reflect local anatomical characteristics, i.e., local compression involving the tongue, palate, and lips is more difficult than that involving the gingiva and buccal mucosa. However, we found no statistically significant difference in choice of haemostatic method according to site of haemorrhage.
Antithrombotic agents have been widely used to prevent and treat cardiovascular disease and stroke1920. Therefore, many studies of the complications associated with postoperative bleeding have been performed in patients taking antithrombotic agents. Use of acetylsalicylic acid alone does not significantly increase the risk of bleeding after oral surgery10,21. However, patients receiving dual antiplatelet therapy or anticoagulants, such as warfarin and direct oral anticoagulants, are at greater risk of bleeding after minor oral surgery; however, a local haemostasis method at the time of the procedure is usually enough to avoid excessive bleeding1113222324. Previous studies have focused mainly on whether or not antithrombotic therapy should be stopped before invasive dental treatment, and an antithrombotic agent's effects on the haemostasis method used in cases of secondary haemorrhage are unclear. In the present study, the haemostasis method used was likely to be more complicated in patients with secondary or delayed haemorrhage using antithrombotic agents.
We found that minor oral surgical procedures, including free gingival grafts, bone grafts for alveolar atrophy, and periodontal flap surgery, but not tooth extraction or installation of a dental implant fixture, increased the likelihood of needing complex haemostasis. Postoperative local compression easily controlled bleeding in an extraction socket. An implant fixture itself functioned as a pressure dressing; and primary closure was possible in implant surgery, which is more favourable for haemostasis25. Most of the previous studies on procedure-related bleeding and the haemostasis method applied have focused on the antithrombotic agent used. Scully et al. reported that, with the exception of harvesting of an autogenous bone graft, extensive flap, or osteotomy, use of a local haemostatic agent only reduced bleeding without discontinuation of oral anticoagulant therapy after simple extraction or implant placement1426. Febbo et al.27 reported that the number of postoperative bleeding complications increased as the number of teeth extracted increased. In contrast, Gualandro et al.28 recommended continuation of antiplatelet therapy in patients undergoing multiple tooth extractions, biopsy, flap surgery, gingivectomy, or alveoloplasty. These researchers suggested that the usual dose of warfarin could be continued in patients undergoing extraction of up to 5 teeth or installation of up to 6 implants. Another study found no correlation between the risk of postoperative bleeding and type of dental surgery23.
Most studies of oral bleeding have focused on risk factors that affect bleeding after dental procedures in patients taking medications that affect the mechanism of haemostasis1529. However, no previous study has evaluated the factors determining the method required for effective haemostasis in patients with intraoral haemorrhage, regardless of antithrombotic therapy or the dental procedure performed. Moreover, complex haemostasis measures are relatively more costly and time-consuming to perform than local compression. Nevertheless, most of the published studies did not separate simple and complex haemostasis methods. The novelty of our study is that we separated these two methods.
This study has several limitations. First, the study had a retrospective design and was based on review of medical records without direct patient observation. Second, we only focused on the causative dental procedure; we did not consider the details of each procedure, extent of damage caused by surgery, the state of inflammation at the surgical site, and time elapsed since the procedure. Third, we considered only the presence or absence of systemic disease without detailed disease classification. Fourth, we did not consider the platelet count or PT-INR at the time of haemorrhage because such tests were only performed in patients with severe bleeding. Therefore, a larger prospective study that considers these factors is needed.
V. Conclusion
Conventional local compression is easily performed and useful when a patient visits the emergency room with intraoral bleeding. However, primary use of another method, such as a haemostatic agent, suturing, electrocautery, or removal of the cause of inflammation, might be preferable for rapid haemostasis in patients who have undergone minor oral surgery, such as a free gingival graft, bone graft for alveolar atrophy, or periodontal flap surgery, while taking antithrombotic agents.
 XML Download
XML Download