

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
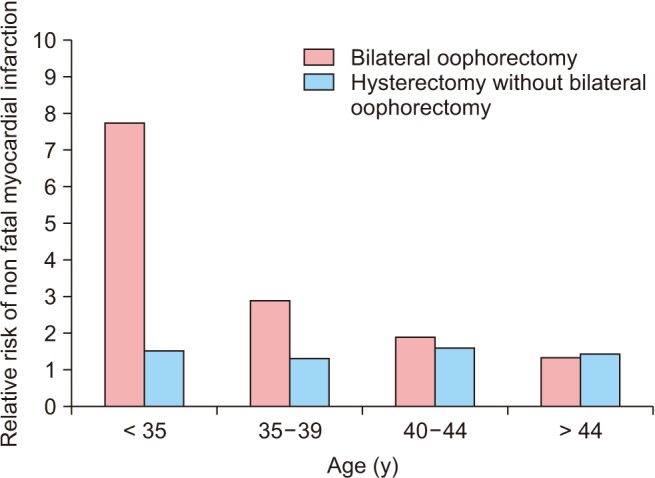
Menopause is an important phenomenon in every woman's life and can be initiated in a primary (i.e., natural) or a secondary form (i.e., via surgery, chemotherapy, radiotherapy, etc.). Surgical menopause refers to the removal of both ovaries with or without the removal of the uterus [1]. Depending on its timing, surgical menopause can be categorized as pre-mature for patients who are under 40 or early menopause for patients who are under 45 years old. In surgical menopause the body automatically enters the menopausal phase without any preparation. This can cause a crisis in women's lives [23]. Annually, in the United States, 36,000 women under the age of 45 undergo either a hysterectomy with bilateral oophorectomy or surgical menopause. The most common ages for undergoing surgical menopause in decreasing order of occurrence are under 35, 35–39, 40–44, and above 44 [4] (Fig. 1). In the UK, 1 in every 5 women who has had hysterectomy has also undergone oophorectomy. According to the World Health Organization's health report in 2002, 146,422 women have undergone hysterectomy in Iran, a figure that has been rising in recent years [5].
Sudden menopausal crisis, caused by the immediate drop in sex hormone levels, causes an exacerbation in the distressing symptoms of menopause [4]. This crisis compromises the vasomotor, psychosocial, physical, and sexual wellbeing of a woman [6]. Marra et al. [4] reported that 100% of women with surgical menopause experience a wide range of vasomotor symptoms. In 90% of cases, they experience more severe hot flashes compared to those who go through natural menopause. This process continues for an average of 8.5 years after the surgery. Additionally, undergoing oophorectomy prior to the age of 45 results in a 5-time increase in the morbidity rate resulting from neurologic and mental disorders [4]. It also increases the risk of developing various cardiovascular diseases [7], reduced bone density [8], neurological diseases, and cardio-metabolic and urogenital disorders. Surgical menopause also has a negative effect on a woman's sexual well-being and satisfaction [89]. Overall, these issues significantly influence women's quality of life and satisfaction [10]. These problems not only influence the quality of life in surgically menopausal women, but also cause distress, disability, as well as enormous financial burden on health systems [11]. The quality of life in surgically menopausal women is lower in all domains, especially in psychosocial domain compared to the natural menopausal women [12]. The majority of the surgically menopausal women who experience moderate to severe symptoms need preventive care for at least up to 10 years after undergoing risk-reducing salpingooophorectomy, in order to improve their quality of life [13]. The use of hormonal therapy is considered to be the last option, due to its side effects such as causing breast and uterine cancer [10]. Therefore, alternative methods such as education or counseling are often suggested [5]. It is thought that increasing women's awareness through applying proper educational methods, which are in accordance with social norms, results in improving the quality of their lives in various aspects [14]. Group counseling along with interpersonal communication further increases the effectiveness of the education provided. In these sessions, participants are able to share similar experiences with their peers, ultimately contributing in making better decisions by group members for resolving their own issues [15]. Therefore, the purpose of this study was to investigate the effectiveness of a multi-dimensional group counseling program, based on the great clients, ask clients, tell clients, help clients, explain how to use, return for follow up (GATHER) approach, on the quality of life of the surgically postmenopausal women.
Go to : 
MATERIALS AND METHODS
This randomized clinical trial, consisting of a control and an intervention group, was conducted from December 2017 to September 2018. Data sampling was done in two stages: initially, 4 healthcare centers from the northwest region that are affiliated with Shahid Beheshti University of Medical Sciences were randomly selected. Subjects were then assigned to two groups of intervention and control by applying simple random sampling as follows; first, a registration list was created using the participants' information. Next, the participants were invited to report to a designated location on a particular day in order to receive information on the purpose of the study. Then, a written consent was obtained from the eligible individuals who were willing to participate in the study. Each person was then given ID code. Next, random numbers were generated in order to read the numbers from top to bottom. After registering the random numbers, the odd numbers were designated to the control group and the even numbers to the intervention group. This process was continued until the sample size was exhausted. Sample size was calculated using the G-Power software (USA) with a 95% confidence interval (α = 5%, β = 20%, and power = 80%), in accordance with the guidelines specified [16], with an estimated 20% lost to follow-up rate 78 persons.
The data was collected at 4-time points: 1) before the intervention/baseline, 2) after the intervention, 3) 1 month after the intervention, and 4) 3 months after the intervention. The inclusion criteria were: 1) bilateral salpingo oophorectomy (BSO) with or without hysterectomy, 2) married women, 3) 35–55 years old, and 4) within 6 months of BSO.
Exclusion criteria included: 1) surgically menopausal women who had received additional treatments in form of chemo or radiation therapy or BSO due to cancer, 2) using hormone replacement therapy (HRT) within 6 months and till the end of the study period, 3) using drinking or smoking, and 4) women who had chronic diseases such as diabetes, hypertension, seizures, or mental disorders.
The study was designed as follows: the intervention group was organized into 4 subgroups (3 groups, 10th and 1 group, 9th). Four subgroups received 6 continuous, weekly sessions of group counseling for an average of 90 minutes per session addressing 4 symptoms of vasomotor, psychosocial, physical, and sexual domains. The sessions were conducted in a bright and quiet environment away from any noise pollution with the participants gathering in a circle for better face-to-face interaction. These group counseling sessions were done in 3 phases while adhering to the GATHER approach: 1) orientation and proceeding phase in first session, 2) proceeding phase in second to fifth session, and 3) conclusion phase in sixth session.
It should be noted that the participants were also consulted in devising the discussion guidelines and topics. The content of the meetings is listed in Table 1. There were no interventions in the control group.
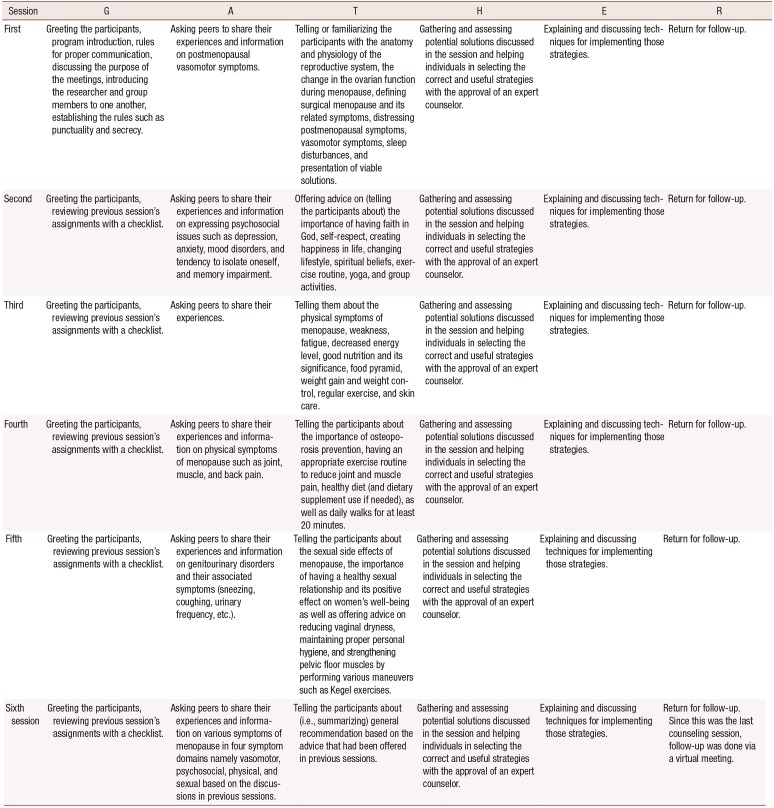
Table 1
Group counseling session agenda including the introduction, intervention, and termination of the program based on the GATHER approach for counseling
![]()
In order to consider the ethical issues and due to the observed low quality of life in the control group, upon completion of the study, the control group participants were offered notebooks containing detailed contents of the group counseling sessions.
A demographic questionnaire was used to investigate factors related to the characteristics of a particular population. The Menopause-specific Quality of Life (MENQOL) questionnaire was also used to assess the quality of life in various symptom domains namely vasomotor, psychosocial, physical, and sexual. The MENQOL questionnaire is a widely-recognized, standardized tool that was developed and used by Hilditch et al. [17] in 2008. Content validity within the Iranian society was done by Yasdkhasti et al. [18] in 2011. The reliability of this questionnaire was done by test-retest analysis in the overall quality of life (r = 0.84), vasomotor (r = 0.80), psychosocial (r = 0.79), physical (r = 0.82), and sexual (r = 0.83) domains [2]. According to scoring and points and number of questions (29 questions), minimum and maximum scores for vasomotor, psychosocial, physical and sexual dimensions were, respectively, 3 to 24, 7 to 56, 16 to 128, and 3 to 24; the overall quality of life was 29 to 232. According to the MENQOL questionnaire, a higher score indicates lower quality of life whereas a lower score indicates a better one in surgically menopausal women.
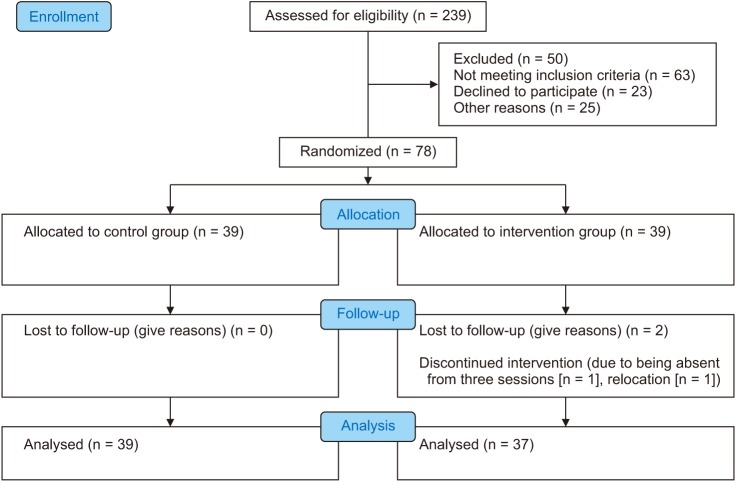
Two of the participants were lost to follow up in the intervention group, one due to being absent from three sessions because of the time conflict with work hours and the other due to relocation. (Fig. 2).
Statistical analysis was conducted using IBM SPSS Statistics 19.0 software (IBM Co., Armonk, NY, USA). Chi-square and Fisher's exact test were used for qualitative variables. Statistical results from the quantitative data were presented with mean ± standard deviation. Data normality was reviewed using the Kolmogorov-Smirnov test. The score for the sexual domain did not follow a normal distribution in either of the intervention or control groups. For that reason, non-parametric tests such as Wilcoxon, Mann-Whitney and Friedman tests were used to assess those scores. Scores in other domains followed a normal distribution. Therefore, parametric tests such as t test and two-way analysis (time × group) of variance (ANOVA) with repeated measures of “time” were used to analyze the multidimensional counseling program on each of the dependent variables. Also, the Greenhouse-Geisser correction was used in the case that the sphericity assumption was not established. The a priori level of significance was set at 0.05.
Go to :
RESULTS
In this study, the characteristics of demographic data on 78 participants (n = 39 per group) were analyzed. There were no significant statistical differences between the control and intervention groups in terms of the age, menopausal age, body mass index, number of children (live or dead), number of abortions, socioeconomic status, life satisfaction, or level of education. These variables were homogenous before the intervention/baseline (Table 2).
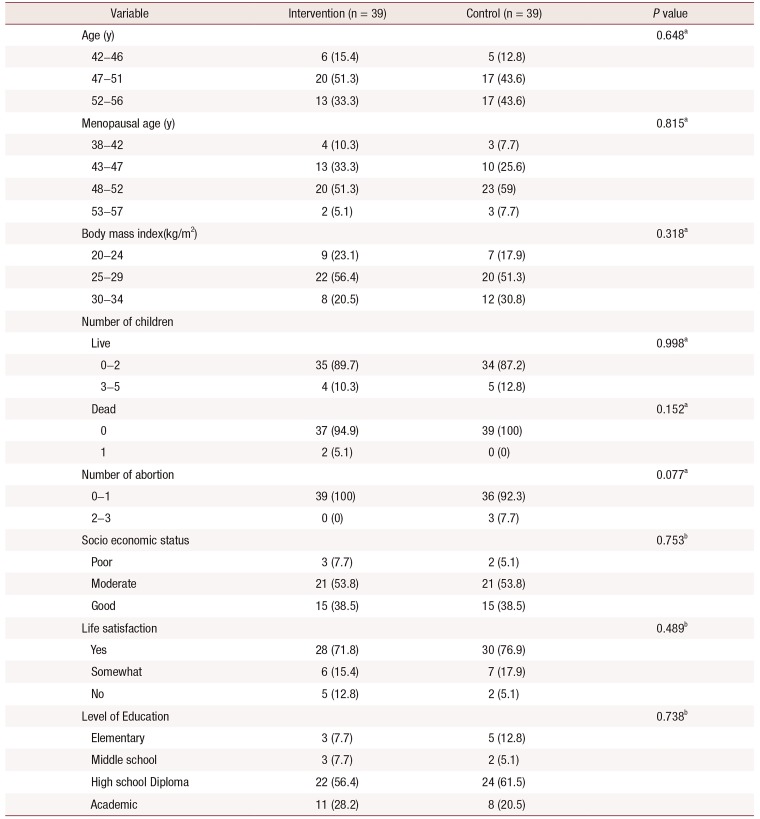
Table 2
Comparison of baseline demographics characteristics between intervention and control groups
![]()
At baseline, mean scores in domains of vasomotor, psychosocial, physical, and overall quality of life were compared using the independent t test and results showed no significant difference between the control and intervention groups. Additionally, at baseline, the mean scores for the sexual domain were analyzed by the Mann-Whitney test for control and intervention groups. The results showed no significant difference (Table 3).
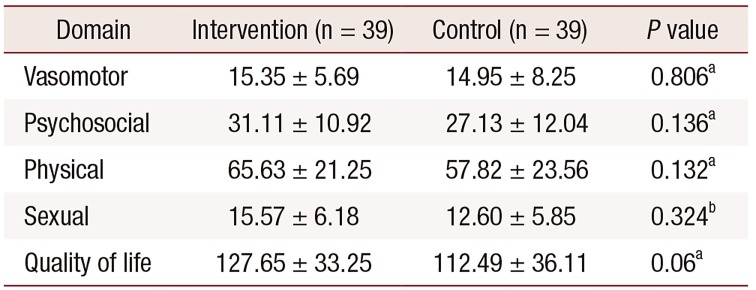
Table 3
Baseline comparison of the mean of overall quality of life score and its domains in two groups
![]()
Paired t test results in the intervention group showed that the mean score of overall quality of life, vasomotor, psychosocial, and physical domains 3 months after the intervention was significantly different compared to those baseline. The Wilcoxon test results in the intervention group showed that the mean score for the sexual domain 3 months after the intervention was significantly different compared to those of baseline. Paired t test results in the control group showed no statistically significant differences (Table 4).
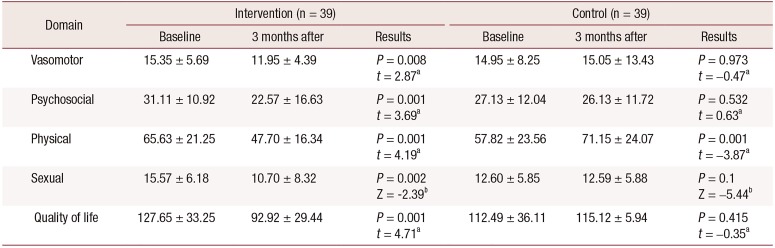
Table 4
Comparison of the overall quality of life score and its domains before and 3 months after the intervention in each of the control and intervention groups
![]()
The ANOVA test results with repeated measures in control and intervention groups showed that the temporal trends of the mean scores in the vasomotor, psychosocial, and physical domains during at 4 time-points (i.e., baseline, after the intervention, 1 month after the intervention, and 3 months after the intervention) were statistically significant between the two groups. The results of the Mauchly's test for the vasomotor and sexual domains revealed that the sphericity assumption was not established (P = 0.001). Therefore, Greenhouse-Geisser assumption was used to correct the degrees of freedom of the repeated measures test. The Friedman test showed a statistically significant difference between the control and intervention groups, in the mean score trend in the sexual and overall quality of life domains during at 4 time-points (Table 5).
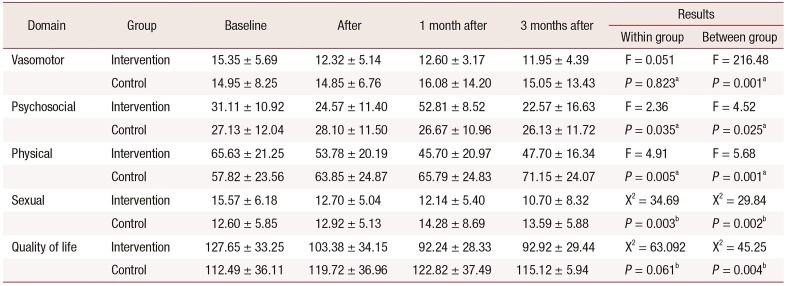
Table 5
The repeated measures and Friedman tests of quality of life and its domains at 4 time-points in intervention and control groups
![]()
Go to :
DISCUSSION
In our study, comparison of mean scores of vasomotor, psychosocial, physical, and sexual domains, as well as the overall quality of life at baseline in the intervention and control groups showed no statistically significant difference. The mean score of overall quality of life and their domains after the intervention was significantly different compared to that baseline in the intervention group. There were no statistically significant differences in control group. Also, the trend of changes at 4 time-points based on the results of the repeated measures test showed statistically significant difference in overall quality of life and their domains between the two groups. Surgical menopause can result in a crisis in women's life and have a negative effect on the quality of their life [9], as it causes sudden changes in various aspects of their lives, which are distressing and bothersome [17]. In a descriptive study conducted on 700 postmenopausal women, 4 symptom domains related to the quality of life namely vasomotor, psychosocial, physical, and sexual, as well as overall quality of life were analyzed using MENQOL questionnaire. The main distressing issues based on a decreasing order of severity were related to vasomotor and physical domains, respectively. Therefore, proper interventions were designed to mainly focus on improving the quality of life in those particular domains [19]. In the present study, the effectiveness of implementing group counseling sessions was assessed in improving the quality of life of surgical postmenopausal women and decreasing the associated distressing symptoms in 4 domains of vasomotor, psychosocial, physical, and sexual, as well as the overall quality of life. The results of the study showed that, implementation of a 6-week, consecutive, and multi-dimensional group counseling program had a positive effect in the intervention group compared to the control regarding decreasing the distressing postmenopausal symptoms. As such, statistically significant differences were observed in the average scores for overall quality of life and its 4 domains at 4 time-points between the intervention and control groups in the average scores for overall quality of life and its 4 domains (i.e., vasomotor, psychosocial, physical, and sexual) at 4 time-points.
The rate of hot flash in surgically postmenopausal was reported 90% to 100% vs. 80% in naturally menopausal women [20]. Several studies have also evaluated the effectiveness of group counseling in reducing the vasomotor symptoms using the group support method [1617192021] as well as group discussion methods described by Forouhari et al. [22] and Rostami et al. [23]. In the study by Rostami et al. [23], vasomotor scores in the intervention and control groups were compared 3 months after the group counseling, which showed a statistically significant reduction in hot flash, daytime sweating, and night sweats and improvements in other distressing symptoms [22]. In this study, the effectiveness of the group counseling program on the vasomotor domain was evaluated over time, and a significant decrease was found in the score for this domain.
Surgical menopause is also associated with psychological effects in addition to physical ones [24]. Experiencing the abrupt onset of menopause along with its associated symptoms and having to deal with the new state can place women in a vulnerable state of mental health and cause psychosocial crisis [2125]. Many women experience severe menopausal symptoms interfering with their daily life routine, and negatively influencing their overall quality of life [26]. Eighty percent of women in various parts of the Middle East experience distressing symptoms such as headaches, sexual issues (such as vaginal dryness and decreased libido), palpitations, hot flashes, sweating, insomnia, and irritability, all of which can reduce their quality of life [16]. A clinical trial study on 89 patients with breast cancer based on a group psychosocial intervention reported that women in the intervention group had less depression, less overall mood disturbance, better overall quality of life, and fewer psychiatric symptoms than those in the control group, beginning immediately post-intervention and remaining so at 2 years post-intervention [10]. In a study of 350 Iranian post-menopausal women, a series of premature menopausal complications including forgetfulness and lack of concentration (56%), psychological and mood issues (52.6%), insomnia (50.6%), and hot flashes and fatigue (48.9%) have been reported [27]. The results of a study showed that surgically menopausal women experience a higher level of stress, anxiety, and depression, as well as a lower overall quality of life compared to the women with natural menopause. Therefore, in the present study, it is suggested to design a multi-dimensional counseling program for postmenopausal women aimed at improving the quality of their life [28]. Psychological changes caused by menopause can influence various elements of empowerment such as self-efficacy and self-esteem; they can diminish one's sense of self-worth and create a negative self-concept in postmenopausal women. They can also cause a sense of inadequacy and lack of control over the distressing symptoms of menopause [29]. On the other hand, knowledge enrichment through participation in group counseling sessions plays a crucial role in enabling postmenopausal women to deal with their psychosocial issues. In a study, an educational intervention was implemented based on an empowering model developed to enable health promoting behaviors, and a positive correlation was observed between the elements of the empowering model and the health promoting behaviors [30]. In another study by Faraji et al. [16], the effectiveness of group counseling on psychosocial symptoms, with a focus on self-care, was investigated. In their study, a positive impact was observed after conducting five weekly, consecutive group counseling sessions with an average of 60 minutes per session. In our study, group counseling also showed a positive impact in the psychosocial domain in the intervention group.
Surgical menopause leads to serious health consequences such as osteoporosis, memory loss, genitourinary and sleep disorders, weight gain, muscle pain, fatigue, and lack of energy [4]. Several studies have suggested providing education and counseling to postmenopausal women to improve their physical wellbeing [14203132]. In another study, the effectiveness of the “green practice” was investigated on improving the sleep quality in elderly women who had no routine physical activity. The study was conducted for 10 weeks with 3 sessions per week, each lasting 60 minutes. Sleep quality was assessed using the Pittsburgh Sleep Quality Index, in which a statistically significant increase was observed in the average score for sleep quality before and after the intervention in the intervention group [30]. The results of a study also showed the positive effect of group counseling on diabetic postmenopausal women who were recommended to have an exercise routine and a proper diet, taking dietary supplements as needed. The study showed that, after 3 months, with respect to the physical well-being, the quality of life improved in the intervention group [33]. Exercise, proper diet, and daily walks for at least 20 minutes were also included in the present study. There was a statistically significant difference in the average score of physical fitness between the control and intervention groups, indicating the effectiveness of these strategies in reducing distressing physical symptoms.
Hypoestrogenism can also cause distressing symptoms in postmenopausal women such as vaginal dryness, decreased libido, and sexual contact avoidance due to the dyspareunia [34]. In one study, a 70% reduction in sexual performance and an 80% reduction in sex drive were reported [35]. Changes in libido, avoiding sexual contact, and reduction in quality of life with respect to sex have all been reported to be more significant in surgically postmenopausal women compared to the ones who go through natural menopause [336]. It is reported that surgically postmenopausal women are at a 17% increased risk for developing disorders of sexual dysfunction compared to naturally postmenopausal women [34]. After conducting a large trial with an emphasis on biomedicine, Newton et al. [37] concluded that not all the symptoms of menopause can be attributed to the decrease in sex hormones; they emphasized that in order to alleviate menopausal symptoms. One needs to consider the psychosocial and cultural issues of postmenopausal women and design multi-dimensional programs addressing such issues. The effect of counseling in improving the quality of life of the menopausal women was evaluated in a semi-experimental study, consisting of control and intervention groups and using a counseling method that is based on the GATHER approach. This study was conducted in form of 4 continuous, weekly counseling sessions with each session lasting for 45 to 60 minutes in the intervention group. The control group received routine counseling. The results of the study based on the MENQOL questionnaire showed that there was only a statistically significant difference in the quality of life score as it was related to sexual well-being and that the difference in the scores for vasomotor, psychosocial, and physical domains did not show any significant difference [38]. Another study showed that a group counseling program consisting of 4 sessions, 120 minutes each, that focused on improving sexual function in menopausal women led to statistically significant improvements after 2 months compared to its status prior to the intervention, while the difference was not significant in the control group [39]. In another study conducted on women with an average age of 39 ± 5 years old, it was found that group counseling, involving 8 sessions 60-minute sessions, improved the intimacy and marriage satisfaction in the intervention group after the last counseling session [40]. Similarly, our study with 6 weekly group counseling sessions resulted in significant improvements in the quality of life in regards to sexual well-being baseline as well as one and three months later in the intervention group. Yazdkhasti et al. [25] also examined the effects of implementing an educational support group program in improving the quality of life and reducing the distressing menopausal symptoms in 4 domains namely vasomotor, psychosocial, physical, and sexual. The program consisted of 10 weekly sessions each lasting 120 minutes. No interventions were done in the control group. The results, according to the MENQOL questionnaire, showed a statistically significant difference between the symptom scores related to vasomotor, psychosocial, physical, and sexual domains in the intervention group 3 months after the intervention compared to baseline. This different was not statistically significant in the control group. Regarding the effectiveness of the proposed program in the present study, it appears that group counseling offers promising solutions in resolving the distressing symptoms of menopause, and also postmenopausal women who participate in such programs are better prepared to discuss their issues regarding sexual well-being and other domains with their peers and are able to benefit from the experiences of others as well.
A particular limitation of this study was the probability of content leakage from the intervention to the control group. This limitation was minimized to our best efforts by having the participants from the control and intervention groups attend the counseling sessions at the healthcare center on different dates. Additionally, occasionally the length of the counseling sessions caused mild fatigue in some participants. This was addressed by holding brief receptions. Factors such as accounting for different participant lifestyles, providing routine care in healthcare centers, and public education through mass media or social networks were beyond the scope of this study and the authors' control.
In the present study, the implementation of multi-dimensional group counseling sessions addressing the vasomotor, psychosocial, physical, and sexual domains in surgically postmenopausal women led to the significant improvements in reported symptoms in these domains as well as the overall quality of life for these individuals. It was also found that knowledge enhancement through sharing similar experiences among peers by those who have experienced the distressing symptoms of menopause firsthand, in a reliable and trustworthy setting with the presence of an expert counselor to guide the process, has helped the participants to make better and more effective decisions over the course of the study. Therefore, implementing this approach with less expenditure in health care organizations aimed at improving the quality of life in surgically postmenopausal women is highly recommended.
Go to :
 XML Download
XML Download