

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Postmenopausal osteoporosis is the most common bone disease and can be managed using a variety of pharmacological agents. Menopausal hormone therapy (MHT) is effective in reducing postmenopausal bone loss and the risk of fracture and has been mainstay for the management of postmenopausal osteoporosis [12]. However, some postmenopausal women on MHT (between 5% and 15%, depending on compliance) continue to lose bone and even experience fractures [3]. Therefore, the combination of MHT with other treatments may be beneficial in postmenopausal women with insufficient response to MHT.
Bisphosphonates are stable pyrophosphate analogs that bind to hydroxyapatite in bone and inhibit bone resorption by decreasing the number and activity of osteoclasts. Etidronate was initially used, followed by alendronate and then risedronate [4]. Most of these bisphosphonates have been approved for use in treating osteoporosis in many countries and have been shown to increase bone mass and reduce fracture rates at the spine [56], hip, and other sites up to 40% in postmenopausal women [78]. Several studies from Caucasian countries have reported that the combined use of MHT with oral bisphosphonate has been reported to increase bone mineral density (BMD) better than individual drug therapy [9]. Our group, however, reported that 12 months of alendronate added to ongoing MHT did not prompt a significant BMD increase in postmenopausal Korean women [10].
Oral bisphosphonates may cause gastrointestinal (GI) disturbance in about 20% of women [11]. Moreover, for patients who have preexisting GI disease such as esophagitis and gastritis, these approaches are accompanied by poor compliance that necessitates the use of another administration route [12]. There have been no studies conducted to date that focus on the efficacy of the combination of pamidronate infusion and MHT in postmenopausal women.
Thus, the purpose of the present study was to evaluate the effects of adding intravenous pamidronate to ongoing MHT in postmenopausal Korean women with low BMD and GI disturbance.
Go to : 
MATERIALS AND METHODS
Subjects and treatments
This retrospective cohort study included 74 postmenopausal women who had received MHT for at least one year between January 2000 and December 2007 at Samsung Medical Center in Seoul, Korea. MHT was administered in an individualized manner and consisted of estrogen at a dose approximately equivalent to 0.625 mg/day of conjugated equine estrogen. Additionally, all patients with intact uteri were also prescribed progestogen in either a cyclic or continuous regimen. Women were considered postmenopausal if their amenorrhea duration was more than 12 months or if their serum follicle-stimulating hormone level was higher than 40 IU/L. Eligible patients were those who had low BMD (T-score < −2.0) in the lumbar spine, femur neck, or total hip. Patients were excluded if they had a history of certain diseases including hyperthyroidism or hyperparathyroidism or were taking medications such as glucocorticoids or anticonvulsants that could affect bone mineral metabolism. Patients were also excluded if they had received any bisphosphonate or fluoride within the last year. The study protocol was approved by the Institutional Review Board of Samsung Medical Center (no. 2019-07-106).
The study participants continued to follow their same prescribed MHT regimen. The pamidronate group who could not tolerate oral bisphosphonate due to GI disturbance (n = 30) received 15 to 30 mg of pamidronate (Hanlim Pharmaceuticals Inc., Seoul, Korea) in 250 mL normal saline intravenously infused over two hours every three months for 12 months. Nonsteroidal anti-inflammatory drugs were used as needed. The unparalleled control group (n = 44) received oral placebo for 12 months. We employed data that satisfied the inclusion criteria from another randomized placebo-controlled trial that was designed to evaluate the efficacy of oral bisphosphonate [10]. All women also received oral calcium supplementation if tolerable.
Bone mineral density
BMD was measured at the second to fourth vertebrae of the lumbar spine and at the hip by dual energy X-ray absorptiometry (DXA; Hologic, Inc., Marlborough, MA, USA) with fan-beam technology. Bone densitometry was performed at baseline and after 12 months of therapy. Percent changes from baseline BMD were calculated.
Biochemical markers of bone resorption
Urinary deoxypyridinoline was assessed in the placebo group via enzyme immunoassay by the manufacturer's manual and corrected for creatinine level. Serum N-telopeptide of type I collagen was measured in the pamidronate group via enzyme-linked immunosorbent assay using Osteomark® (Ostex International, Seattle, WA, USA). Bone markers were measured at baseline and after 6 and 12 months of therapy, respectively.
New fracture
The occurrence of new fracture was ascertained by history taking at each visit. Asymptomatic spine deformity was also checked by X-ray at baseline and the end of the study.
Statistical analysis
Baseline characteristics and BMDs are summarized in the form of mean ± standard deviation and number with percent for continuous and categorical variables, respectively. Comparisons between the placebo- and pamidronate-treated groups were conducted for continuous variables by Student's t tests or Wilcoxon rank-sum test after checking normality via Shapiro-Wilks test. Comparisons for categorical variables were performed using Chi-squared test or Fisher's exact test, as appropriate. Changes in BMD and bone resorption markers within each group and between groups were compared using paired and Student's t tests, respectively. Multivariable linear regression was further used to investigate group difference in BMD changes with adjustment of baseline characteristics that showed significant difference between the two groups. Examples include body mass index (BMI), duration of previous MHT, and baseline BMD of femur neck. A two-tailed value of P < 0.05 was considered to be statistically significant. Statistical analysis was completed using the Statistical Analysis System software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Go to :
RESULTS
Clinical characteristics of the study subjects
The baseline characteristics of each group are presented in Table 1. There were no statistically significant differences between the two groups except regarding BMI, duration of previous MHT, and BMD of the femur neck.
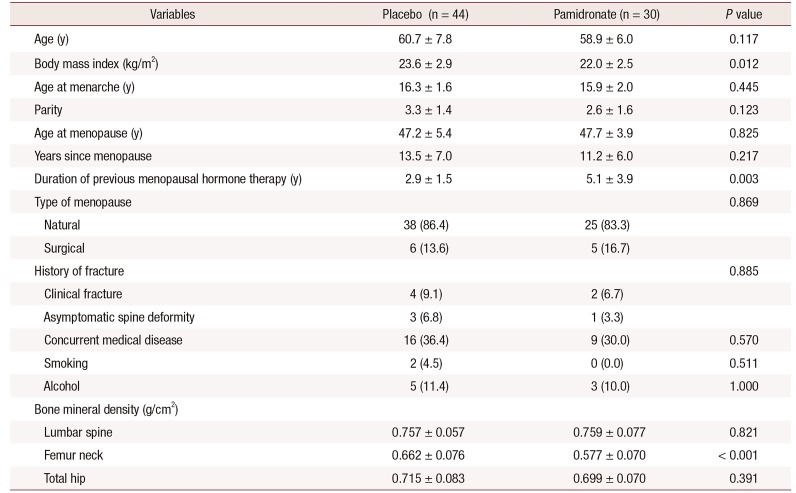
Table 1
Baseline characteristics of study patients
![]()
Bone mineral density
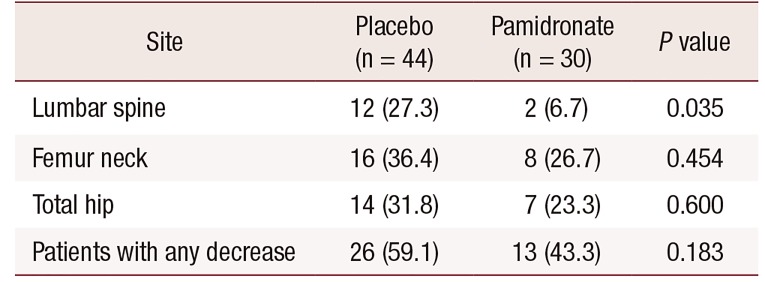
Figure 1 displays the mean percent changes in BMD after 12 months of treatment. In the placebo group, significant increase was observed in BMD values of lumbar spine (P < 0.001) and total hip (P = 0.003), but not of femur neck (P = 0.062). In the pamidronate group, BMD values of the lumbar spine, femur neck, and total hip were all increased significantly (P < 0.001 for all). BMD increase of the lumbar spine was significantly higher in the pamidronate group compared to the placebo group (mean change: 3.7% vs. 6.2%; P = 0.021). This group difference remained significant after adjusting baseline BMI and duration of previous MHT (P < 0.001). BMD increase of the total hip seems higher in the pamidronate group compared to the placebo group (mean change: 2.4% vs. 4.6%) with marginal significance before and after adjustment of baseline BMI and duration of previous MHT (P = 0.097 and P = 0.062, respectively). The increase in BMD of the femur neck showed no significant difference between two groups before and after adjustment of baseline BMI, baseline BMD of the femur neck and duration of previous MHT (P = 0.321 and P = 0.369, respectively). Conversely, the number of patients with BMD decrease after 12 months of treatment is shown in Table 2. The percentage of BMD at the lumbar spine was significantly lower in the pamidronate group than in the placebo group (27.3% vs. 6.7%; P = 0.035). The BMD percentages at the femur neck and total hip in the pamidronate group tended to be lower than the placebo group.
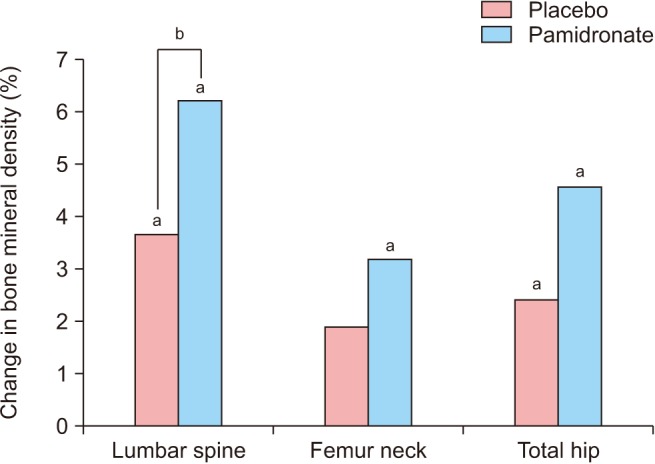 | Fig. 1Mean percent changes in bone mineral density after 12 months of therapy. aP < 0.01 vs. baseline; bP < 0.05 vs. placebo.
|
Table 2
Number of patients with decrease in bone mineral density after 12 months of treatment
![]()
Biochemical markers of bone resorption
There was no significant change in bone resorption markers during the 12 months of therapy within either group (Table 3). Percent changes in the two different markers considered were also comparable between the two groups (data not shown).

Adverse effects
There were no significant differences in the adverse effects experienced by the study patients in the two groups (Table 4). Four cases (9.1%) of joint pain occurred only in the placebo group, whereas four cases (13.3%) of flu-like symptoms were reported only in the pamidronate group. Regarding new fractures, one case (3.3%) occurred in the pamidronate group and three cases (6.8%) occurred in the placebo group.
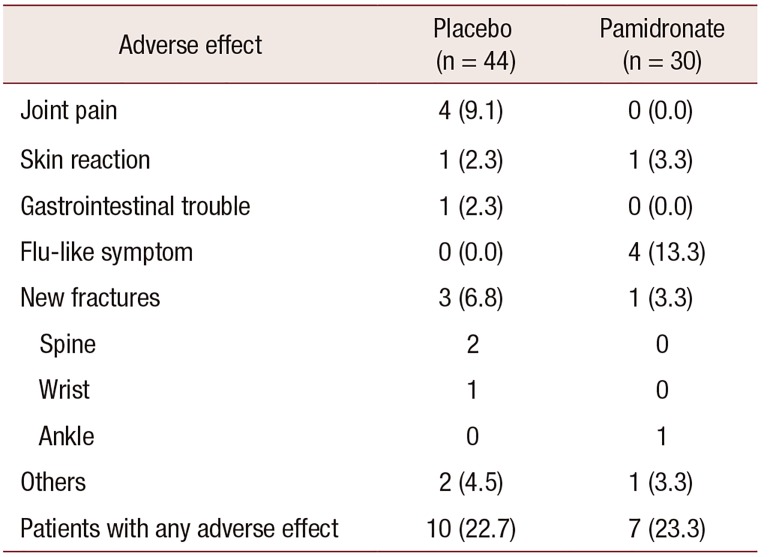
Table 4
Adverse effects experienced by study patients
![]()
Go to :
DISCUSSION
This study shows that the addition of intravenous pamidronate every three months for 12 months to ongoing MHT increased BMD of the lumbar spine in postmenopausal Korean women with low BMD and GI problems.
In the present study, BMD percentages were increased significantly in the lumbar spine and total hip in the placebo group. This BMD increase in the control group could be attributed to improved compliance with MHT.
Pamidronate is a nitrogen-containing bisphosphonate that improves BMD in both the spine and hip [13] and prevents spinal fracture [14]. Pamidronate administered intravenously is reported to have similar effects to those of alendronate on BMD of the lumbar spine and total hip in patients with osteoporosis [15]. Pamidronate injection is licensed in Korea for the treatment of osteoporosis. To our knowledge, this is the first study to report a beneficial effect of intravenous pamidronate on BMD in combination with MHT.
Importantly, oral daily alendronate added to ongoing MHT did not yield any significant BMD change in postmenopausal Korean women [10]. In this study, however, pamidronate infusion increased spine BMD compared to oral placebo. Pamidronate has a 5-to-10-times lower antiresorptive potency than alendronate [16]. The reason for the difference between the two bisphosphonates is not clear, but possible explanations are as follows: first, the GI absorption rate of oral bisphosphonate is extremely low (1%–5%) [16] and the intravenous administration of pamidronate provides high bioavailability (100%) by way of direct access to the systemic circulation. Further, higher adherence resulted in a better response to pamidronate. Oral alendronate was given daily, whereas the between-dose interval of pamidronate was three months. In addition, oral bisphosphonate requires inconvenient dosing recommendation to promote bioavailability and minimize upper GI disturbance, including long fasting, taking the medicine with a large amount of water, and maintaining an upright position for two hours after intake. Participant acceptability was likely enhanced with an intravenous route of administration. Indeed, a change from oral administration of bisphosphonate to an intravenous infusion may be considered in patients showing insufficient response [17].
Congruent with our BMD findings, the nonresponder rate for the lumbar spine was significantly lower in the pamidronate group. Hip BMD values were also increased with pamidronate for 12 months but did not reach statistical significance compared with the control group. A difference in bone composition might be attributed to the different responses to pamidronate observed by site. The lumbar spine contains a greater amount of trabecular bone, which is metabolically more active than cortical bone.
In this study, there was no change in the bone resorption marker reviewed in the placebo group. Of note, no change was also observed in the pamidronate group upon considering a different marker. Oral bisphosphonate in combination with MHT usually decreases bone resorption markers further and raises concerns about severely suppressed bone turnover [10]. If this is the case, the safety concerns regarding the use of intravenous pamidronate combined with MHT might be less than those for oral bisphosphonate. These findings require further confirmation because the biological mechanisms underlying this result are uncertain.
Patients with GI disturbance were selected for inclusion in the pamidronate group. Using intravenous preparation, no participants reported further GI trouble with pamidronate. Acute phase reaction resulting from mild transient systemic inflammatory reactions such as febrile sense, nausea, myalgia, and anorexia occurred in 10% to 30% of patients receiving their first bisphosphonate infusion [18]. In this study, flu-like symptoms were experienced in 13.3% of the pamidronate group but did not recur at subsequent infusions. Even though this study is not powered to check the difference, the number of new fractures was lower in the pamidronate group.
Our study has some limitations. This study is retrospective in design and employed an unmatched control group. In addition, the study duration was short, and the sample size was not large enough. Further randomized clinical trials are warranted using newer generations of bisphosphonate infusion with matched placebo controls to validate the clinical efficacy of combination therapy with MHT and intravenously administered bisphosphonate.
In conclusion, adding intravenous pamidronate to ongoing MHT for 12 months might increase the BMD of the lumbar spine in postmenopausal Korean women with low BMD. Pamidronate infusion is an appropriate alternative in patients with intolerance to oral bisphosphonate.
Go to :
 XML Download
XML Download