

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Description of the condition
Menopause is an important period in the life of women; one reason being the numerous problems it may cause, affecting the quality of life of women [12]. One common problem is vaginal discomfort [3], and it is estimated that up to 40% of post-menopausal women experience this problem [4], leading to loss of collagen, elastin, and smooth muscles in the vagina [5]. Low estradiol levels, which menopausal women commonly experience, can cause a deficient maturation of vaginal mucosa [6]. This condition is clinically presented by dryness, irritation, itch, and dyspareunia [7] and it could affect daily activities, sexuality, relationships, and quality of life [8]. To evaluate vaginal health, it is necessary to assess vaginal epithelial cell measurement, vaginal dryness, and vaginal acidity (pH).
Description of the intervention
Treatment approaches that are used for vaginal health improvement in menopausal women are hormonal therapy and complementary therapy [69].
Such treatments are commonly based on local hormonal therapy, in the form of vaginal creams, tablets, or suppositories [1011], although other routes of hormone administration have also proven to be successful. Despite the fact that the benefits of estrogen replacement in preventing vaginal complications and reducing the incidence of related symptoms are well established [12], hormonal therapy has various limitations and contraindications [13].
Vitamins D and E have been used for the treatment of menopausal disorders and vaginal discomfort [1415]. Vitamin D is involved in the regulation of growth and differentiation of many cells, especially tissues lining the stratified squamous epithelium [16], which are present in the vagina and are regulated by Vitamin D [17]. Vitamin D3 binds to an intracellular receptor that is a member of the steroid-thyroid hormone receptor family. Vitamin D3 and its receptors form a complex that binds to the Vitamin D3 response element of genes and either positively or negatively affects the transcription of that gene [1819].
The importance of this review: Being free of sexual problems can improve the confidence and mental state of women [20]; therefore, it is important to resolve sexual problems associated with menopause. Accordingly, vitamin D may be useful in vaginal discomfort in menopause women [7212223]; however, some experimental results are controversy [2425].
Objective
Review of the literature showed that there was no study that summarized the effects of vitamin D on vaginal health in menopausal women; therefore, the aim of this systematic review study was to evaluate and summarize the effects of vitamin D on vaginal health in menopausal women.
Go to : 
MATERIALS AND METHODS
In this narrative systematic review the following criteria were used to determine their eligibility into our study.
Inclusion criteria: we performed a screening of titles or abstracts followed by a full-text review. Studies were considered eligible if they met the following criteria: they were clinical randomized, placebo-controlled, double-blind, single-blind, non-blinded trials, or cohort trials published in the English language biomedical journals until 2019; they were quasi-randomized trials, the study populations were menopausal women; vitamin D supplementation alone or plus calcium was studied; the study was published in English language journals without reference to a scientific quality index; and all clinically-used dosages and durations of vitamin D administration in menopausal women were considered.
Exclusion criteria: vitamin D was used in combination with other drugs except calcium, data was insufficient, studies were conducted on animals or in in vitro models, and the diagnostic criteria were not applied to the study subjects. Case reports and articles on non-vaginal health were excluded.
Participants are menopausal women. Types of intervention are use of vitamin D supplementation alone or plus calcium. Exposure is vaginal health such as vaginal epithelial cells, vaginal dryness and vaginal pH in menopausal women. Types of outcome measures are performance-based; outcome measure was the Vaginal Maturation Index and vaginal pH and vaginal dryness. Primary outcomes are change in vaginal epithelial cells in menopausal women. Secondary outcomes are change in vaginal pH and vaginal dryness.
Search methods for identification of studies
The electronic search engines included PubMed, Web of Science, Scopus, Google scholar, and Embase using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.
Search strategy: the search strategy included a combination of key words, and medical subject headings: vitamin D, vaginal, and menopause. We checked all titles and abstracts. Full text copies were obtained when the studies were considered possibly relevant. Searching other resources: gray literature and the reference list of articles.
Data collection and analysis
Selection of studies
Two review authors independently screened titles and abstracts for inclusion of all potential studies, and after they were identified they were then coded as ‘retrieve’ (eligible or potentially eligible/unclear) or ‘do not retrieve’. Next, the full-text studies coded as ‘retrieve’ were obtained and the two review authors independently screened the full-texts and identified studies for inclusion, and identified and recorded reasons for exclusion of the ineligible studies.
Data extraction and management
The following data were extracted (if available): author, publication year, and methodology (including criteria for menopause diagnosis, sample size, study design, dosage of intervention, duration of intervention, and main outcomes). We resolved any disagreement through discussion or, if required, we consulted a third person and used the consensus strategy. We identified and excluded duplicates and collated multiple reports of the same study. We recorded the selection process in sufficient detail to complete a PRISMA flow diagram.
Assessment of risk of bias in included studies
One reviewer assessed the quality of the included studies according to criteria for selection, methods of outcome assessment, and data analysis, using the Cochrane scale. If there were disagreements between the two reviewers during the process of study selection, the issues were resolved through discussion among multiple investigators.
Measures of treatment effect
For vaginal health outcomes we used the epithelial cells score (%) or number of participants with vaginal health improvement after intervention or after comparison with the control group.
Dealing with missing data
To complete the information that was unavailable from the published reports, we contacted the researchers of the relevant studies and they provided the missing information.
Assessment of heterogeneity
Methodological diversity such as variability in the study design and risk of bias were observed during this review. Some variations in the materials and methods such as varied drug forms of vitamin D, different inclusion criteria, or measurement scale in some studies led to no meta-analysis of the review.
Go to :
RESULTS
A total of 351 studies seemed to be potentially relevant in the first search. However, 340 studies were excluded (irrelevant subjects) after screening the titles and/or abstracts. Finally, full texts of the remaining 11 studies were evaluated in depth, 6 trials with a total of 391 participants met the inclusion criteria. Table 1 shows the diagram of the retrieved articles included in the systematic review.
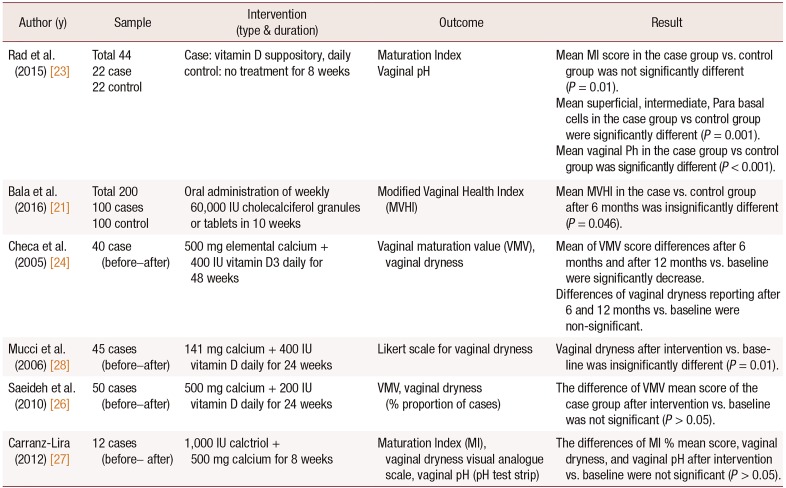
Table 1
The characteristics of articles included in the systematic review
| Author (y) | Sample | Intervention (type & duration) | Outcome | Result |
|---|---|---|---|---|
| Rad et al. (2015) [23] |
Total 44 22 case 22 control |
Case: vitamin D suppository, daily control: no treatment for 8 weeks |
Maturation Index Vaginal pH |
Mean MI score in the case group vs. control group was not significantly different (P = 0.01). |
| Mean superficial, intermediate, Para basal cells in the case group vs control group were significantly different (P = 0.001). | ||||
| Mean vaginal Ph in the case group vs control group was significantly different (P < 0.001). | ||||
| Bala et al. (2016) [21] |
Total 200 100 cases 100 control |
Oral administration of weekly 60,000 IU cholecalciferol granules or tablets in 10 weeks | Modified Vaginal Health Index (MVHI) | Mean MVHI in the case vs. control group after 6 months was insignificantly different (P = 0.046). |
| Checa et al. (2005) [24] | 40 case (before–after) | 500 mg elemental calcium + 400 IU vitamin D3 daily for 48 weeks | Vaginal maturation value (VMV), vaginal dryness | Mean of VMV score differences after 6 months and after 12 months vs. baseline were significantly decrease. |
| Differences of vaginal dryness reporting after 6 and 12 months vs. baseline were non-significant. | ||||
| Mucci et al. (2006) [28] | 45 cases (before–after) | 141 mg calcium + 400 IU vitamin D daily for 24 weeks | Likert scale for vaginal dryness | Vaginal dryness after intervention vs. baseline was insignificantly different (P = 0.01). |
| Saeideh et al. (2010) [26] | 50 cases (before–after) | 500 mg calcium + 200 IU vitamin D daily for 24 weeks | VMV, vaginal dryness (% proportion of cases) | The difference of VMV mean score of the case group after intervention vs. baseline was not significant (P > 0.05). |
| Carranz-Lira (2012) [27] | 12 cases (before–after) | 1,000 IU calctriol + 500 mg calcium for 8 weeks | Maturation Index (MI), vaginal dryness visual analogue scale, vaginal pH (pH test strip) | The differences of MI % mean score, vaginal dryness, and vaginal pH after intervention vs. baseline were not significant (P > 0.05). |
![]()
Description of studies
Results of the search
The search was updated from February 2000 to November 2018. We screened a total of 351 records from the following databases: Web of Science (7), PubMed (17), EMBASE (7), Google Scholar (31), Scopus (289). Overall, this review has a total of six trials, 23 duplicated, 5 animal studies, 50 breast cancer studies that were excluded, 11 studies selected for full text assessment in which 6 studies were excluded. See Figure. 1 for the study flow diagram. Six trials were included in this review: 2 studies were individually randomized controlled trials (RCTs) [2123] and 4 were quasirandomized [24262728]. A total of 391 participants were part of the 6 trials. Overall, the included trials fall into two main groups: vitamin D alone and vitamin D plus calcium. See Table 2 for excluded studies [715222930] and their reason.
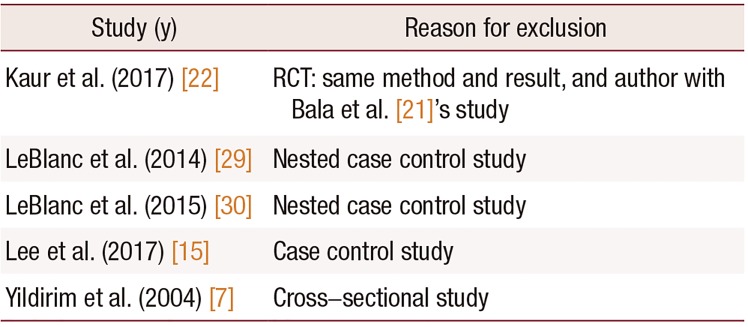
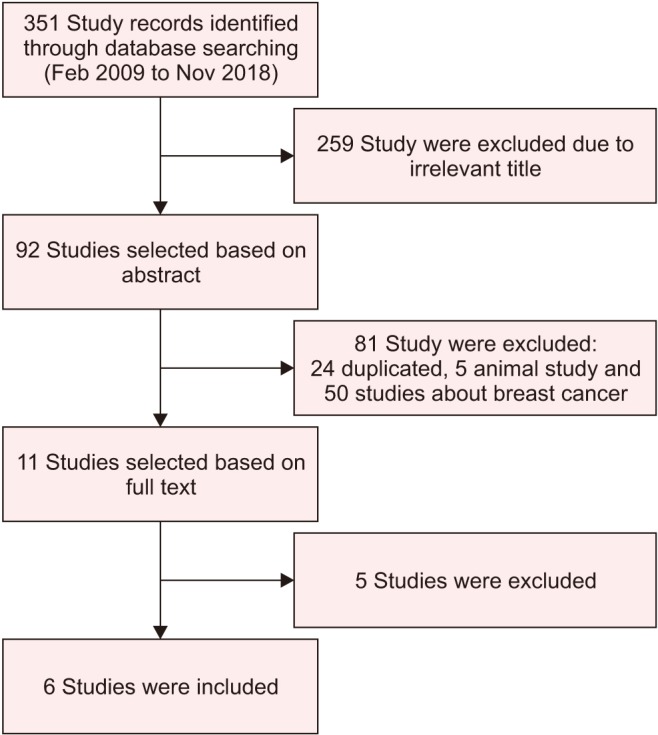
Table 2
Characteristics of excluded studies
| Study (y) | Reason for exclusion |
|---|---|
| Kaur et al. (2017) [22] | RCT: same method and result, and author with Bala et al. [21]'s study |
| LeBlanc et al. (2014) [29] | Nested case control study |
| LeBlanc et al. (2015) [30] | Nested case control study |
| Lee et al. (2017) [15] | Case control study |
| Yildirim et al. (2004) [7] | Cross–sectional study |
![]()
Risk of bias in included studies
Allocation (selection bias)
Table 3 shows the results for the random sequence generation and allocation concealment for the Cochrane Risk of Bias tool. For random sequence generation, 6 trials were deemed to be at low risk and for allocation concealment and 6 trials were at unclear risk.
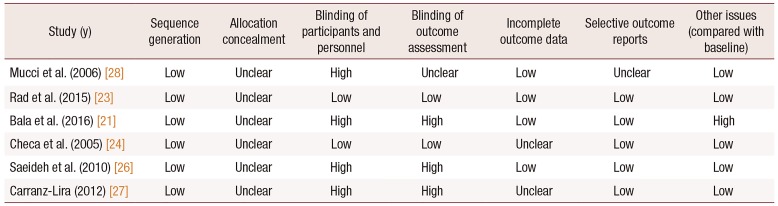
Table 3
Risk of Bias score in included studies
| Study (y) | Sequence generation | Allocation concealment | Blinding of participants and personnel | Blinding of outcome assessment | Incomplete outcome data | Selective outcome reports | Other issues (compared with baseline) |
|---|---|---|---|---|---|---|---|
| Mucci et al. (2006) [28] | Low | Unclear | High | Unclear | Low | Unclear | Low |
| Rad et al. (2015) [23] | Low | Unclear | Low | Low | Low | Low | Low |
| Bala et al. (2016) [21] | Low | Unclear | High | High | Low | Low | High |
| Checa et al. (2005) [24] | Low | Unclear | Low | Low | Unclear | Low | Low |
| Saeideh et al. (2010) [26] | Low | Unclear | High | High | Low | Low | Low |
| Carranz-Lira (2012) [27] | Low | Unclear | High | High | Unclear | Low | Low |
![]()
Effects of interventions
Vitamin D alone versus placebo or no treatment
Two studies used vitamin D alone vs. a placebo or no treatment. In the study of Rad et al. [23], 1,000 IU doses of vitamin D vaginal suppository were used with for eight weeks, but in Bala et al. [21]'s study 60,000 IU doses of vitamin D were administered orally and weekly. In two studies that included 244 menopausal women, both studies showed vitamin D was effective in the vaginal health of these women.
Vitamin D plus calcium versus baselin
Four studies used vitamin D plus calcium and compared the results versus baseline [24262728]. In the study of Checa et al. [24], 40 menopausal women used 500 mg of elemental calcium plus 400 IU vitamin D3 for 24 weeks. In Mucci et al. [28]'s method, 141 mg calcium plus 400 IU of vitamin D were used daily, for 24 weeks in 45 women. In Carranza-Lira et al. [27]'s study, 12 women used 1000 IU of calcitriol plus 500 mg of calcium daily for eight weeks, and in the study of Saeideh et al. [26], 50 cases used 500 mg of calcium plus 200 IU of vitamin D daily, for 24 weeks. The 4 studies included 147 women. One study showed vitamin D plus calcium effectiveness in vaginal health [28] and 3 showed no positive result regarding vaginal health [242627].
Epithelial cell
Rad et al. [23] showed that use of vitamin D can improve the superficial, intermediate, parabasal of vaginal cells. Also, the mean vaginal maturation score between the case and control group was significantly increased. Bala et al. [21] reported that use of vitamin D significantly affected the vaginal health index such as vaginal epithelial integrity. Checa et al. [24] reported vaginal maturation mean score after 24 weeks (−38.7%; after 12 months, −51.8% significantly decreased). Saeideh et al. [26] showed vaginal maturation mean score was not significant between the before intervention (27.51 ± 18.98) vs. after intervention (29.41 ± 18.75). In Carranza-Lira et al. [27]'s study, the mean % score change maturation index and parabasal and intermediate cells were not significant but the mean % score in superficial cells before intervention 2.5 ± 4.5% vs. after intervention 10.0 ± 8.5% was significantly changed. Three studies reported vitamin D can positively affect vaginal epithelial especially in superficial cells [212327], although two other studies were inconsistent regarding this result [2426].
Vaginal pH
Vaginal acidity (pH) was affected in two studies and pH mean score was significantly decreased in the vitamin D group. In the study of Carranza-Lira et al. [27], the mean score of the pH strip test (1.5 ± 1.2 vs. 1.7 ± 1.0) did not significantly change before and after the intervention. Two studies reported significant change in vaginal pH [2123] and one study result was negative [27].
Vaginal dryness
Bala et al. [21] found that use of vitamin D orally significantly affected vaginal moisture and consistency. Checa et al. [24] showed that after 24 weeks, 21.4% of cases and after 12 months, 15.8% of cases suffered from vaginal dryness, but this change was not significant (P= 0.5). In Mucci et al. [28]'s study, 13.3% of cases reported improvement after intervention vs. baseline and 39% of the vaginal dryness mean score decreased and this change was significant (P= 0.01). Saeideh et al. [26] reported the number of vaginal dryness before intervention was 36 cases and after intervention was 37 cases, and Carranza-Lira et al. [27] reported severity mean score using the visual analogue scale before intervention (58.5 ± 24.0) vs. after intervention (64.4 ± 27.2) was not significant. Two studies showed vitamin D can improve vaginal dryness [2128] and three studies were inconsistent [242627].
Go to :
DISCUSSION
Summary of main results
Vitamin D alone versus placebo or no treatment
Vitamin D alone, in the high doses tested or vaginaluse format, appears to be have an effect on vaginal epithelial cells especially superficial cells and vaginal pH decrease (two trials, 244 participants) [2123]. Use of vitamin D alone in the vaginal formats and 1,000 IU doses tested daily appears not to be able to reduce vaginal dryness (one study, 44 participants). Duration time of use of vitamin D was 8–10 weeks, which seems sufficient time for vaginal health improvement except for vaginal dryness.
Vitamin D plus calcium versus baseline
Although there was no firm evidence that vitamin D (including 25-hydroxy vitamin D) with calcium was more effective than vitamin D alone for vaginal health in menopausal women, only one study (calcium plus vitamin D) reported positive vaginal health results [28] while three studies did not report any positive results [242627]. The calcium dose in all of the studies was 500 mg daily except for one study [28] that used a low dose (141 mg daily). The dose of vitamin D in two studies [2428] was the same (400 IU), but their results were different. The study with low dose calcium and 400 IU vitamin D was effective in reducing vaginal dryness [28]. Intervention durations were different, such as 8 weeks [27], 24 weeks [2628] and the longest being 48 weeks [24]. Only 24 weeks duration of vitamin D plus calcium had positive results in vaginal dryness [28].
Adverse effects
Three trials reported adverse effects [242628], which was mostly gastric discomfort. Overall, none of the trials reported the effect of vitamin D on mortality; however, use of calcium and vitamin D for a long time is dangerous and is not recommended for menopausal women, but in another study [31], which was not included in our study, the use of vitamin D and calcium was associated with a reduction in mortality (risk ratios 0.94, 95% CI 0.89 to 0.99). It is highly recommended to measure the level of vitamin D before high doses are administered and it is better to prescribe the supplement based on blood vitamin D levels [32]. Calcium supplements could increase the risk of myocardial infarction [33], particularly in people with a higher dietary calcium intake. Supplements of calcium and vitamin D could also increase the risk of myocardial infarction and stroke [34] but might also decrease the risk of breast cancer [35].
Overall completeness and applicability of evidence
This review included an evidence base from six trials that examined vitamin D (including 25-hydroxy vitamin D) with or without calcium in the improvement of vaginal health in menopausal women with a mean age of 50 years or over. Vitamin D was administered in a variety of formats and doses (oral daily, oral weekly, and vaginal suppository). However, three of the trials in this review tested daily vitamin D3 in doses greater than 800 IU [212327] and one of these trials recruit participants with very low (mean < 12 ng/mL) baseline 25-hydroxy vitamin D blood levels [21]. American Geriatric Society suggests that a minimum blood vitamin D level of 30 ng/mL (75 nmol/L) is necessary in older adults to minimize the risk of menopause complications. It has been suggested that higher doses of vitamin D are required in women with vitamin D insufficiently [36], and vitamin D level testing before intervention is necessary for future studies in vaginal health in menopausal women.
Quality of the evidence
This review included a small body of evidence from six trials with 391 participants. Our assessments of risk of bias and quality assessment are presented in Table 3.
Potential biases in the review process
We believe that selection bias is very low in this review. We have searched a wide range of databases for relevant journals. One report of studies that was published at a different time but using the same method and result was excluded [22]. We only included RCTs and the other low quality evidences such as observational or case-control were excluded.
Agreements and disagreements with other studies or reviews
Although the results of two included studies [2327] and two excluded studies [1537] showed improved superficial vaginal cells by using vitamin D, another study reported that vitamin D was not associated with menopausal related symptoms in menopausal women [29].
The Cochrane review reported that supplements of vitamin D and calcium may prevent hip or other types of fracture [38] and another study suggested that high intakes of dietary vitamin D and calcium may be modestly associated with a lower risk of early menopause [39].
However, the use of complementary therapy such herbal medicine and supplements is beneficial for menopause symptoms such as hot flashes [40], but the results of a meta-analysis study conducted in 2017 showed that oral phytoestrogen cannot be effective in severe vaginal atrophy [41]. Other treatments for vaginal atrophy in postmenopausal women may be the use of laser therapy, in which a study published in 2017, found the effectiveness of this method in improving vaginal health in postmenopausal women and improving their sexual quality, but the use of this method is not recommended due to need of advanced equipment that comes with a high cost [42].
Limitations
One of the limitations of this systematic review was using varied drug forms of vitamin D in the evaluated studies. Other limitations were the different ages of the menopausal women and different inclusion criteria in the studies. The weak methodology of some studies used in our systematic review is also a limitation of this study. Small sample sizes, inadequate treatment allocation, unclear blinding method, and unmentioned randomization technique can degrade the validity of the results. Since there was large variation on the methodology of examined studies, it was impossible to do a meta-analysis.
Implications for practice
Vitamin D alone in the high doses and combined formulations that have been used in some studies appears to be effective in vaginal health in menopausal women.
Implications for research
There is a need to confirm vitamin D treatment effects on vaginal health using longitudinal studies.
Result of this study show that the superficial epithelial cell can be improved with vitamin D. It has been suggested that the topical use of vitamin D in future studies be also compared with vaginal estrogen and vitamin D suppository.
Go to :
 XML Download
XML Download