

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Human cadaveric dissection has been used as the fundamental teaching tool in anatomy for centuries. Though technology has revolutionised gross anatomy teaching over the past few decades, research clearly emphasizes on the indispensability of dissection in anatomical sciences. Moreover the anatomy dissection lab in coherence with the body donation programs has the potential to cultivate humanistic values among medical students which could possibly contribute invaluably towards the making of empathetic physicians of tomorrow [1].
Appropriate preservation is critical to the effective use of cadavers in educational settings. It must ensure safety from harm, destruction or decomposition. Hence, embalming cadavers with special chemicals like formaldehyde (FA) has been employed worldwide [2].
Formalin, an aqueous solution of FA, has been used as a fixative in anatomy, pathology, and in embalming since the 20th century. Readily available and cheap, FA is an effective fixative with rapid penetration of tissues and long-term preservation properties [3]. Laboratories typically employ 10% formalin or 4% FA water solution.
Cadavers are infused with embalming fluid through femoral arteries or the internal carotid arteries. Vapours of FA emitted during dissection sessions elevate the indoor FA concentration and result in significant exposures to FA for medical students and instructors [4].
The anatomists, technicians, and students in the laboratories are continually exposed to FA during their dissection course. The level of exposure depends on the duration of time spent in the gross anatomy theatre and the working environment [5].
The Occupational Safety Health Administration (OSHA), formaldehyde standard and equivalent regulations in states protect workers exposed to FA and apply to all occupational exposures to FA. The permissible exposure limit (PEL) for FA in the workplace is 0.75 ppm of air measured as an 8-hour time-weighted average. The standard includes a second PEL in the form of a short-term exposure limit of 2 ppm which is the maximum exposure allowed during a 15-minute period [6].
FA level monitoring, cadaver positioning and ventilation strategies are not rigorously inspected by any medical regulatory bodies across the world including India. Scant evidence is available in published literature on indoor FA concentrations in Indian Medical Colleges. Reports from other countries have reported FA levels above prescribed standards that could be harmful to those exposed. Hence this study intends to estimate the concentration of FA in cadaver preservation rooms, and dissections halls, and to evaluate its effects among exposed students, teachers, and workers.
Materials and Methods
This prospective exploratory study was conducted among teaching and non-teaching dissection theatre faculties, first year medical students of a government and private medical college located at Mysuru, Karnataka. A Universal Sampling technique was applied. The faculty and students (at the end of the first professional year) exposed to formalin for at least 6 h/wk and consenting to participate were included in the study. Known cases of epilepsy, asthma, and cardiac disorders were excluded. Institutional ethical clearance and permission was received from institutional heads prior to the study.
The following three components were evaluated under this study where cadaver dissection is delivered to students for 3 h/day and 6 days a week.
Physical parameters
The physical parameters of dissection hall and cadaver storage room were measured. The dimensions of the room, number of cadavers stored, number of windows, exhaust measures, departmental and personal protective measures used were recorded. The number of cadavers available on tables and the number of students allotted per cadaver were noted.
Questionnaire evaluation
Study subjects were given a self-administered questionnaire to note the effects of FA exposure. The validity of questionnaire responses was ensured through subject experts. Lab attendants were assisted with local language translation and were filled in by the investigator.
Air sample analysis
A formaldemeter, a cost effective tool to measure the level of FA was utilized. The instructions provided by the supplier were followed. Formaldemeter directly measures airborne concentrations of FA. It utilizes a diffusion type air sampling method with one second frequency. Response time is less than 60 seconds. The FA sensing range is 0–5 ppm with 0.001 ppm resolution and 10% accuracy at 2 ppm.
Air sampling locations
Indoor FA was monitored in (1) cadaver storage room: The workers access this room during handling of specimens and cadavers. The commercial formalin containers (37% FA) utilized for embalming are stored here (2) dissection theatre: where cadavers are handled during dissection classes for various courses (for 3 hours a day and 6 days in a week). Cadavers are infused with embalming fluid with 4% FA concentration.
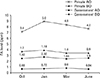
The FA sampling instruments were placed approximately 3 feet (breathing zone) above floor—at the same height at which cadavers are placed on dissection tables. FA levels were measured at each table and at four corners of the hall. The level of FA was digitally recorded by the instrument. The baseline FA level detection was done in the morning immediately after opening the lab. Each Monday, cadavers which have been stored in tanks to maintain hydration are placed back on dissection tables for demonstration. Formalin vapour levels sensed immediately after placement of cadavers was high due to quantity of FA in storage tanks. Hence second documentation was recorded after placing the cadavers on the dissection table. This was repeated 4 times corresponding to upper limb, lower limb, abdomen, and head and neck dissection schedule.
The same three parameters were measured in another medical college. The findings were documented, and analyzed by suitable statistical tools.
Results
Physical parameters of Anatomy department
The Government Medical College had a spacious dissection hall, with better ventilation in terms of windows, doors, and fans. The Private Medical College had less space per cadaver and per student, and poorer ventilation for the hall space, but better exhaust from powered fans. The cadaver storage room of the private medical college contained more tanks and cadavers for the space but had good ventilation in terms of windows and exhausts.
Neither the Government nor the Private Medical College had any protective measures against fire risk management, nor any facility for monitoring formalin gas levels individually or at the dissection hall.
Effects of FA on exposed students, teachers and workers
Personal protective measures
Sixty-nine point one percent of the students used gloves regularly, 79.8% never wore masks, and 75.8% wore shoes. Forty-four point four percent of the workers wore gloves regularly, 66.7% never wore masks or shoes. Ninety-two point nine percent of faculty wore gloves, 71.4% wore shoes regularly, and 85.7% never wore masks.
Discussion
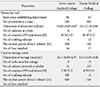
The minimum prescribed standards for dissection hall dimensions at medical colleges is as per regulations of Medical Council of India. These standards do not address occupational hazard issues like ventilation or exhaust strategies, and exposure monitoring. The ventilation system in India is solely dependent on airflow through windows and doors. Where exhaust fans are provided, the capacity of such fans for ventilation and ventilation rate are typically not considered (Table 1). This has great disparity with conditions in Iran where the physical dimension of dissection lab (4.2 m×6.10 m×3.13 m having 9 cadavers) but where the hall is provided with six ceiling diffusers arranged in two rows attached to the central air conditioning system and four exhausts provide general ventilation for the laboratory [7].
A school in Japan with the physical dimension of dissection lab 19.4 m×25 m×3 m had 25 cadavers at a time. It initially provided general exhaust ventilation with three outlets providing ventilation rate of 247 m3/min which later was increased to 280 m3/min by providing local ventilation system to each table. This dramatically reduced the faculty and student exposure to chemical [8].
In a medical school in Thailand, the gross anatomy dissection room was of 20 m×6 m×3.5 m (420 m3) with two doors and four windows for 18 cadavers. But had an efficient ventilation system with 10 air conditioners, 3 exhausts and 8 air cleaners which provided room deodorization as well as odour controllers. They were switched on for at least 30 minutes before class and were switched off 30 minutes after class [9].
In Poland, a study measured FA concentrations in the gross anatomy laboratory were relatively low (0.47–0.57 mg/m3), but medical students experienced various reactions (lacrimation in 85.9%, red eyes, dry and itchy eyes, runny nose, sneezing, and headache in >50% of students, cough in 44%, and dry throat or throat irritation in 42% of students) [10]. Wineski and English [11] measured mean exposures of less than 1 ppm and a peak of 5 ppm FA in an anatomy laboratory and reported a range of 0.07 to 2.95 ppm.
There is lack of regulations either from Medical Council of India or Occupational Safety and Health allotted to Ministry of Labour and Employment under the Government of India. Hence occupational hazard due to FA is not given utmost consideration despite of necessity.
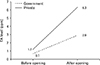
The difference in FA concentration documented in the cadaver storage room before opening the tanks among two institutes was marginal but after opening was significant (Figs 1, 2). The difference is explained by vast difference in the number of cadavers stored per unit floor area.
A study in an Indian Medical College monitored indoor air at the breathing zone and observed FA levels (0.11 to 1.07 mg/m3 in the cadaver storage room and 0.06–1.12 mg/m3 in the gross anatomy laboratory) that were beyond the prescribed guideline values laid down by regulatory bodies. This was considered to be harmful for students' and teachers' health [12].
A study in Japan noted that FA evaporating from cadavers tended to be associated with higher levels in the dissection room. It was elevated at the start, and decreased with the progression of cadaver dissection; however, it exceeded the Health, Labour and Welfare Ministry's guidelines for indoor chemical concentrations in specified workplaces by 0.25 ppm on all days of measurement except the last day of dissection. The FA levels could not be reduced to below the guideline presumably because of evaporation from cadavers, suggesting the need for further measures [13].
The levels measured before placing cadavers in both study institutions were above acceptable standards prescribed by American Conference of Government Industrial Hygienists (0.3 ppm) and Japan Society for Occupational Health (0.5 ppm) for exposure to FA in the work environment [13]. The levels after opening especially in the private college were alarmingly high, raising a serious health concern.
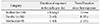
The present study documented symptoms like burning and irritation of eyes, and running nose prominently among students (Table 2). Additionally, workers and faculty with prolonged exposures experienced symptoms like redness of eyes, migraine, nasal congestion, breathlessness, recurrent sinusitis, sore throat and chest congestion. Skin, gastrointestinal and respiratory symptoms and fatigue were observed, but less frequently. Renal and neurological symptoms were insignificant. One of the lab workers was treated for skin discoloration due to prolonged formalin contact. The study showed symptoms experienced by workers are more severe than for faculty, which in turn is more severe than for students. Severity of symptoms correlates with the duration and years of formalin exposure for faculty, workers, and students (Table 3).
A study on medical and dental students at a school in Nepal had eye symptoms of irritation and itching (77.5%) as the most common manifestation followed by tearing and reddening. Among the nasal symptoms, nasal blockage and loss of smell (84% and 69%, respectively) was common followed by discharge and sneezing. For the throat, the most common manifestation was sore throat, irritation 84.5% with manifestation of suffocation (59.7%). Skin rashes were seen among 93% and 82% had itching sensation [14].
Tehran medical school documented that the most commonly reported complaints were unpleasant odour (68%), cough (64%), sore throat and runny nose (56%), nasal irritation and itching (52%), and eye irritation (48%) [7].
Similar work at Alexandria but on medical students, staff members, and workers found that 68.8% had skin burning, 68.8% had eczema, 87.5% allergic contact dermatitis, and 68.8% with ocular discomfort and irritation. One hundred percent of them had upper and lower respiratory tract irritation and 54% had work related asthma. They highlighted the severity of toxic, carcinogenic effects, and other consequences of FA [15].
A review of 27 studies on formalin exposure across the world from 2000 to 2013, classified the clinical symptoms, environmental monitoring and preventive measures. Acute exposures are associated with irritation of nose, throat and respiratory tract and long term exposures with neurological symptoms like headache, dizziness. Medical students and workers in the anatomy laboratory must take concrete measures to reduce exposure to FA [16].
Current study comprised a lab worker with 25 years' exposure to FA being diagnosed with nasopharyngeal carcinoma. But its causation by formalin could not be determined.
The study on pragmatic approaches to formalin safety in anatomical pathology highlighted the carcinogenic effects of the formalin and its importance in our daily activities. They recommended formalin spillage management at work places by various techniques like individual actions, engineering measures, and personal protective measures [17].
The NIOSH-2541 method was used by the U.S. OSHA to get FA exposure assessment and they compared its values with normal short term exposure limits. A self-reported symptom questionnaire administered to anatomy laboratory workers and medical students revealed their experience of eye and nose irritations during and off working hours [18].
The suitability of FA as a chemical for embalmment of cadaver for dissection was questioned as it causes numerous health challenges on students. The lack of awareness by laboratory attendants and students on carcinogenic nature of FA was emphasised. They emphasized the utility of protective equipment such as laboratory coats, gloves and suggested introduction of goggles, masks, and ventilators when working in gross anatomy laboratories, and suggested less toxic chemicals for embalming [19].
Increasing awareness of potential health hazards of FA exposure, mandatory use of protective garments and equipment (a laboratory coat, protective goggles, and gloves), and prevention of direct skin contact with FA and adequate ventilation in the Gross Anatomy Laboratory is recommended for students and instructors [4].
This study provides evidence of undue and hazardous workplace exposure to FA. Extension of FA level monitoring to other medical colleges to document excess exposure could validate the results.
Harmful exposure to FA gas can be diminished or prevented by measures like: (1) Taking out the cadavers from tanks well before (at least 30 minutes) starting dissection to avoid exposure to peak levels. (2) Maximizing use of possible room ventilation with windows and doors. (3) Installation of active ventilation at dissection halls and storage rooms. (4) Use of masks containing activated carbons, especially by workers having prolonged FA exposure. (5) Incorporation of routine FA level monitoring facilities and regulation of exposure levels at workplace.
The guidelines with respect to the number of doors, windows, and the exhaust system and ventilation rates must be included by the Medical Council of India. If such a mandate is made, compliance with it would effectively diminish exposure to FA and diminish adverse health effects experienced by those who work with FA.

 XML Download
XML Download