

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
One of the most common procedures used by medical staff is setting up venous access. It is considered a major component of care for both inpatients and outpatients. It seems viewed as a simple technique, but it requires good anatomical knowledge about the targeted veins.
Veins are classified according to their location to the deep fascia into superficial and deep veins; they communicate by perforating veins. The location of the superficial veins within the superficial fascia provides an easy access for cannulation and blood drawing for clinical tests. In addition to venous access, the superficial veins are clinically used for right cardiac catheterization [1].
The superficial veins of the upper extremities are more desirable than the superficial veins of the lower extremities. The venous access of the lower extremities is less durable and accompanied with more complications like venous thromboembolism [23]. Moreover, venous access in the lower extremities limits patients mobility [4].
The superficial veins of the forearm, the hand and less often the foot have been commonly used for venous access [5]. Among the superficial veins; dorsal metacarpal veins (dorsal MCVs), cephalic vein (CV), and basilic vein (BV) are the most common sites for venous access [3]. The superficial veins of the hands are the digital, metacarpal and the begening of the BV on the ulnar side and the CV on the radial side on dorsum of the hand. The veins on the dorsum of the hand are easily palpated, readily visible and supported by metacarpal bones. The dorsal MCVs are the first choice for venous cannulation essentially in pediatric patients [6], while the distal part of the CV has been suggested for vein puncture [7]. It has been indicated that catheterization of the veins in the dorsum of the hand in obstetric patients is more successful than the veins in the lower forearm [8]. However, in urgent situations, the median cubital vein of the forearm is the first choice for cannulation [3].
The advantages to use dorsal MCVs are easeness of accessibility and distal location of the veins, which allow utilization of more proximal veins in the same upper limb when needed [8]. On the other hand, the disadvantages to use these veins are the small size of the veins and the tendency to be mobile [9].
In the elderly however, the veins in the dorsum of the hand are not the preferable site for venous access because the veins are more mobile and fragile and the needle may cause bruising and bleeding under the skin, furthermore, they are tortuous and could be thrombosed [2].
Vein viewer can be applied for many purposes as in plastic surgery procedure; microsurgical anastomoses and most commonly in phlebotomy and intravenous access [10]. Many studies were performed to determine the efficiency of the vein viewer in difficult vein access or vein find specifically in pediatric patients with excellent results, having successful venous access from the first attempt, as well in locating the vein [1112].
Thus, it seems that the superficial veins on the dorsum of the hand are of a major clinical value. Numerous papers and books have provided detailed information about the normal anatomical variations of the antecubital veins [1314]. While the superficial veins of the hand are variant and complicated, despite their clinical value, there is scarce information about their normal anatomical variations. Thus the goals of the present study were to identify the dorsal MCVs and to determine the most prominent dorsal MCV.
Materials and Methods
Subjects
Four hundred and two subjects were enrolled in the study; 217 males and 185 females. Subjects ranged from 18 to 35 years old; they were students and staff of the medical college. A total number of 804 hands were examined. Subjects who had hand injuries, scars, burns were excluded. Subjects were informed in details about the procedure and a written consent was signed. The study was approved by the Institution Review Board of the university (IRB No. P.0/222/1704841).
Instruments
The infrared (IR) vein illumination system (Sure vein ZD-JM-260-01) has been used to identify the dorsal MCVS. It utilizes 750–980 nm wavelength of infrared light, with effective distance of projection of 29–31 cm.
Study design
The procedure was conducted in a dark room with a temperature between 24℃ and 26℃. On the day of the experiment, subjects were instructed to sit and to grip the transmitter device while the forearm was in pronated position (Fig. 1). Before exposing the hand to the IR beam, the targeted area was carefully identified. The targeted area was bounded distally by the flexed second, third, fourth, and fifth metacarpophalangeal joints (MPJs) and proximally by the wrist joint. On the sides of the dorsum of the hand, an imaginary line from the medial side of the fifth MPJ considered the medial boundary of the target area, while an imaginary line from the lateral side of second MPJ considered the lateral boundary.
The most prominent dorsal MCV was identified as straighter, more vertical and with less communicating veins. The subject's hand was then exposed to the IR beam; the dorsal MCVs were photographed by a mobile phone camera. Images were carefully analyzed and grouped according to the course of the metacarpal veins.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics version 22 software (IBM Corp., Armonk, NY, USA). A chi-square test was used to test the association between gender, sidedness and handedness, and common site of the most prominent dorsal MCV. Statistical comparisons were made by Student's unpaired t test. The association was considered statistically significant if P<0.05.
Results
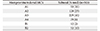
The initial population of this study consisted of 402 subjects; 217 males and 185 females (Table 1). The total number of hands was 804 hands. The number of hands included in this study was 435 in males and 369 in females (Table 1). The number of right hands included in the study 401 was nearly equal to left hands 403 (Table 1). One hundred and eighteen hands were excluded (exclusion rate 15%) and 187 hands (23%) were with complex pattern of veins. The final number of hands included in the study was 503 hands.
It was found during the examination of the dorsum of the hand, that the dorsal MCVs had different courses and communications. Some dorsal MCVs ran between the knuckles of the hand as long dorsal MCVs on the dorsum of the hand (Figs. 1A, 2A), while other dorsal MCVs bifurcated into two veins, where they united with the adjacent bifurcated vein to form short metacarpal veins (Figs. 1B, 2B). It has been also identified that some dorsal MCVs united with an adjacent vein near their origin and formed long metacarpal veins (Figs. 1C, 2C), or away from their origin and formed short metacarpal veins (Figs. 1D, 2D). In addition, some of the dorsal MCVs united with an adjacent vein near their origin and passed parallel to the corresponding extensor tendon (Figs. 1E, 2E). Finally, some of the examined dorsal MCVs were running in different directions and were forming a network of veins on the dorsum of the hand (Figs. 1F, 2F).
The most prominent metacarpal vein was identified according to its origin relative to the MPJs (knuckles) of the hand which courses in intermetacarpal spaces. Veins were classified according to their origin as follows.
Type A1 was present in 53 (11%) of the examined hands, being one prominent vein in the second intermetacarpal space originated between second and third MPJs (Figs. 3, 4). Type A2 occurred in 128 (25%) of the examined hands, where there was one prominent vein in third intermetacarpal space originated between third and fourth MPJs (Figs. 3, 4). Type A3 was the most common being in 229 (46%) of the examined hands (one prominent vein in fourth intermetacarpal space originated between fourth and the fifth MPJs (Figs. 3, 4). Lastly in the A subtypes, A4, accounted for 6% (n=29) of the examined hands having one prominent vein parallel to extensor digitorum tendon of the fourth digit (ring finger) (Figs. 3, 4). There were two type Bs: type B1 (n=12, 2%) of the examined hands, where two prominent veins were found in second and third intermetacarpal spaces, they originated between second and third MPJs and between third and fourth MPJs, respectively (Figs. 3, 4), and type B2 (n=52, 10%) where two prominent veins were found in third and fourth intermetacarpal spaces, they originated between third and fourth MPJs and between fourth and fifth MPJs, respectively (Figs. 3, 4).
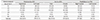
The most common location of the most prominent dorsal MCV was in fourth intermetacarpal space (A3) at 46% (Table 2) and was the most common in both males 118 (45%) and females 101 (44%) (Table 3). In addition, it was equally distributed in both the right (n=112, 46%) and left hands (n=117, 45%) (Table 3) as well as both right handed 99 (42%) and left handed 12 (31%) participants (Table 3). Moreover, it was noted that the symmetry of location of the most prominent dorsal MCV between both hands in the same subject was 29% (n=117) (Table 4).
Statistical analysis using chi-square test, there was not a significant relation between both right and left hands, and site of the most prominent dorsal MCV (P=0.769). There was a significant relation between both females and males, and the site of the most prominent dorsal MCV (P=0.013). There was not a significant relation between right handed and left handed subjects, and the site of the most prominent dorsal MCV (P=0.376).
Discussion
The aim of the present study was to identify the most prominent vein on the dorsum of the hand. A recent study that examined the dorsal MCVs and for the first time they were recognized and classified into different anatomical patterns rather than considering them as a network of veins [15]. However, employing earlier mentioned patterns would not help in recognition of a prominent vein. Patterns were based on the shape of connections between different veins, while identifying a prominent vein should have focused on the individual course of the vein. Thus, the course of the individual dorsal metacarpal veins that were investigated in the present study found that veins on the dorsum of the hand have different courses and communications.
Findings in the present study clearly showed that whatever the course of dorsal MCVs, there were predominantly one or two veins that would run in a straight, vertical course and have less communicating veins connected to them. The only exception was, perhaps, when the dorsal metacarpal veins were forming a network of veins on the dorsum of the hand. Therefore, to identify the most prominent vein on the dorsum of the hand three major criteria were proposed based on the common criteria generally used in choosing an ideal vein for venous access. The criteria of an ideal vein were reported as straight, vertical and has less branches or anastomosis veins [16]. The present study adopted almost the same criteria and took the MPJs and intermetacarpal spaces as reference points to make the recognition of the veins easier.
Applying the above mentioned criteria, it was found that the most prominent vein was located in the fourth intermetacarpal space in 46% of the examined hands. Moreover, the prominent vein which often was located in the fourth intermetacarpal space in both hands as well as in both genders. To a lesser extent there was one prominent vein in the third intermetacarpal space between third and fourth MPJs in 25% and there was one prominent vein in the second intermetacarpal space between second and third MPJs. In addition, there was one prominent vein parallel to extensor digitorum tendon of the fourth digit.
The present study did not investigate why it was possible to have a prominent vein but it has been noted that the location of the prominent vein was more frequent on the medial side of the hand, with the veins of the dorsum of the hand ultimately grouped into radial veins on the lateral side of the dorsum of the hand to form the CV and ulnar group of veins on the medial side to form the BV [17]. Therefore, veins coming from the third intermetacarpal space may need to cross the dorsum of the hand in an oblique course or be connected to adjacent vein to reach the medial side of the hand to participate in the formation of the BV. However, the dorsal MCV in the fourth metacarpal space between the fourth and fifth MPJs is more medial and in line with the BV without any need to be connected to other veins. This may explain the fact that most prominent veins were found on the medial rather than on the lateral side. Moreover, when two prominent veins were identified they were also located in the third and fourth intermetacarpal spaces between third and fourth MPJs and fourth and fifth MPJs.
It is important to mention that the dorsal MCVs on the lateral side of the dorsum of the hand coming from the first and second metacarpal spaces were usually involved in the formation of the radial group of veins that form the CV. In addition, the dorsal MCV that usually runs in the first metacarpal space was not examined in the present study as it was outside of the designed experimental procedure. However, veins in this space are usually oblique and close to radial artery located in this area and to the superficial branch of the radial nerve, therefore, veins in this area are not preferable for venous access [1819].






 XML Download
XML Download