

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
In developing countries, sputum smears microscopy remains the most widely used and is the means by which universal access to diagnosis and treatment can be achieved1. Even though 2-day sputum microscopy is better in sensitivity, people make repeated visits to the health care centers for specimen delivery, results collection, and anti-tuberculosis (TB) treatment initiation. For many patients, the cost of repeated visits to health facilities (HFs) was prohibitive and patients drop-out is a significant problem23. As a result, the World Health Organization (WHO) has recommended a reduction in the number of specimens from 2-day to same-day in settings where appropriate sputum smear microscopy is strongly implemented1.
The fact that mucociliary clearance of respiratory tract is high overnight and sputum specimens obtained early in the morning is more likely productive than spot. The difference in diagnostic sensitivity of the 2 days—and same-day sputum microscopy approaches can be minimized with appropriate instruction of presumptive TB patients to spout out productive sputum specimen, proper smear preparation, staining, careful microscopic examination of stained smears and performing internal quality control for the reagents1.
Presumptive TB patients diagnosed by same-day sputum smear microscopy were more likely submit both specimens (drop-out, 2%) than those screened by 2-day approach (drop-out, 5.8%)13. In Ethiopia, diagnostic drop-out of presumptive TB patients screened for TB by same-day sputum smear microscopy was not yet studied.
On the bases diagnostic shift from 2-day to same-day sputum smear microscopy approach, morning sputum is missed and same-day sputum specimens are used to diagnose pulmonary tuberculosis (PTB). Spot specimens inevitably contain respiratory secretions from both the healthy airway tract and the diseased; the produced sputum specimens are more saliva which has an impact on smearing quality and poor quality sputum specimens might lead to miss diagnoses24. Therefore, in this context strengthening external quality assessment (EQA) is the sole parts of sputum smear microscopy.
In Addis Ababa, Ethiopia, the status EQA of same-day sputum microscopy in HFs participating in regional quality assessment scheme (REQAS) was not so far studied and documented. The present study assessed the status of EQA of same-day smear microscopy in HFs participating in REQAS, smear microscopy service quality, and diagnostic drop-out of presumptive TB patients diagnosed by same-day sputum smear microscopy approach.
Go to : 
Materials and Methods
1. Study design and setting
Cross-sectional retrospective study was conducted on HFs EQA results archived in EQA centers that performed blinded rechecking of sputum smear microscopy, from September 2016 to July 2017 to determine EQA status of same-day sputum microscopy. All newly presumptive TB patients' data registered for same-day sputum smear microscopy in 13 selected HFs for the study were reviewed to determine diagnostic drop-out rate of the same-day approach. The study was supplemented by checklist based assessment TB laboratory infrastructures related to same-day sputum smear microscopy services quality.
Addis Ababa has a total of 540 km2 having 10 sub-cities, 116 districts, and an estimated total population of 3,384,569, with annual growth rate of 3.8%5. It encompasses more 896 public and private HFs, of which 101 public and 52 private were being providing acid-fast bacilli (AFB) microscopy and Directly Observed Treatment Short Course (DOTS) services6.
2. Sample size determination and sampling procedure
Blinded–rechecked EQA results of 153 HFs participating in collected according to lot quality assurance techniques78 were reviewed from the archived data in EQA centers and Addis Ababa Public Health Research and Emergency Management (AAPHREM). New presumptive TB patients' data registered in 12 public and one private HFs providing TB diagnostics and DOTS services were purposively selected to determine diagnostic drop-out rate same-day sputum smear microscopy.
3. Data collection tools and collection procedures
Ethical clearance was obtained from Addis Ababa Health Bureau Ethical Review Committee (#AAHB/2058/321) and letter of support were obtained from AAPHREM and HFs participated in the study were informed that all data collected would remain anonymous treated statistically and remain confidential. Written informed consents were obtained. Checklists were adapted from the national TB-EQA guidelines to assess TB laboratory infrastructures related to same-day smear microscopy services quality. TB laboratory results records books were reviewed since same-day sputum smear microscopy implementation to determine the diagnostic drop-out rate.
4. Data management and analysis
The collected data were checked for completeness, consistency and code number were assigned, entered to micro soft Excel (Microsoft Inc., Redmond, WA, USA). Before analysis, it was cleaned and edited by simple frequencies, cross-tabulation and transferred to SPSS version 20.0 (IBM Corp., Armonk, NY, USA) for analysis. Descriptive statistics, numerical summaries, and tables were used to describe relevant variables.
5. Data quality assurances
One-day training was given for data collectors and appropriate supervision was made throughout data collection. Before submission, data collectors were instructed to check the completeness of each data. The principal investigator rechecked the completeness of the data while receiving from data collectors.
6. Operational definitions
- Good labeling: Sputum smear slides contain the initials name of HFs from which smear slides were collected for blinded rechecking, date smears prepared, serials numbers of slides on registration book and sequences of smear slides.
- Good smear size: When the sputum smears prepared is 1 by 2 or 2 by 3 cm from the center of microscopic slides covered.
- Cleanness: Sputum smear slides with no artifacts during the microscopic examination and clear background with no remnant staining reagents left on the smear.
- Evenness: Sputum smear with even distribution from the center of microscopic slides to the border with appropriate sizes and good coiling.
- Thickness: Good smearing thickness when smear is not too thick and not too thin with partially translucent that enable to read any of written words on the paper through the smear.
- Staining quality: Sputum smear with no remnants of reagents (well decolorized) on the smears when examined microscopically.
- Diagnostic drop-out: New presumptive TB patients registered for same-day sputum smear microscopy who do not submitted any of the two or one sputum specimen.
- Specimens quality: Sputum smears containing more than 10 white blood cells when examined microscopically.
- External quality assessment: A system of objectively checking the laboratory's performance using an external agencies or facilities (EQA centers, regional, or central laboratories) through on-site evaluation of the laboratory, panel testing and blinded rechecking.
Go to :
Results
1. Blinded–rechecked results of same-day sputum smear microscopy
Since same-day sputum smear microscopy implementation in Addis Ababa over 1 year, a total of 7,551 Ziehl-Neelsen (ZN)–stained sputum smear slides were collected for blinded rechecking from HFs participating in REQAS. Sputum smear reading agreement between peripheral laboratories and EQA centers that performed blinded rechecking were 99.6% for negative and 98.8% for positive with overall concordant rates 99.4%, From the total discordant: 44 (0.6%), of which 18 (0.2%) were false-negative and 26 (0.4%) were false-positive. Among false-negatives, 14 (77.8%) were high false-negative and among false-positives, 22 (84.6%) were low false-positive, as the detailed illustrated in Table 1.

Table 1
Sputum smear reading agreement between peripheral HFs laboratories and EQA center lead hospitals or regional laboratory, Addis Ababa, Ethiopia, September 2016 to July 2017
![]()
The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of peripheral laboratories in diagnosing TB against the results of EQA centers as reference standard were 97.4% (95% confidence interval [CI], 95.9–98.5), 99.6% (95% CI, 99.4–99.7), 96.3% (95% CI, 94.6–97.4), and 99.7% (95% CI, 99.6–99.8), respectively.
Specimens, smearing, and staining qualities of same-day sputum smears of HFs participated in REQAS were reviewed. From the total of 7,524 ZN-stained sputum smear results evaluated and documented 2,523 (33.5%) had poor specimen quality as the detailed depicted in Table 2.

Table 2
Quality of same-day sputum smears rechecked in Addis Ababa, Ethiopia
![]()
2. Smear positivity rate and bacillary loads of same-day sputum smears examined in HFs of Addis Ababa
Sputum smear positivity rate and the bacillary loads of smears positive registered in selected HFs for the study were calculated to evaluate the impacts same-day sputum smear microscopy implementation on the bacillary of smears positives. From the total of 6,397 new sputum smear slides examined in HFs included in the study, 249 (3.9%) were positive (129 first spot and 120 second spot). Of 129 first spot sputum smear positive, seven did not submit second spot; two were negative for the second spot smear. Of 3,361 new presumptive TB patients registered in laboratories of selected HFs, 120 (3.8%) were positive for both first and second spot sputum smears. The bacillary loads of sputum smear microscopy were determined using international sputum smear microscopy grading scale6. The majorities of smear positive 106 (42.6%) were 1+ as the detailed illustrated in Table 3.
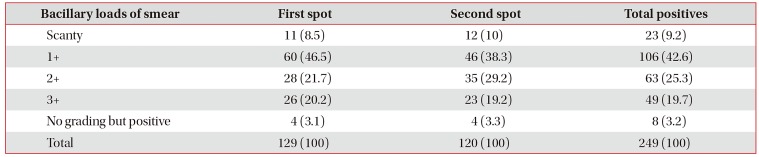
Table 3
Bacillary loads of sputum smear positive examined in HFs of Addis Ababa, Ethiopia, September 2016 to July 2017
![]()
3. Laboratory infrastructures and service quality related to same-day sputum smear microscopy
The infrastructures of HFs laboratories performing sputum smear microscopy was assessed using checklists adapted from national sputum smear microscopy guidelines as variable indicating quality of same-day sputum smear microscopy. Nearly 46.4% of HFs performing sputum smear microscopy had no separate area for TB smear microscopy as the detailed showed in Table 4.
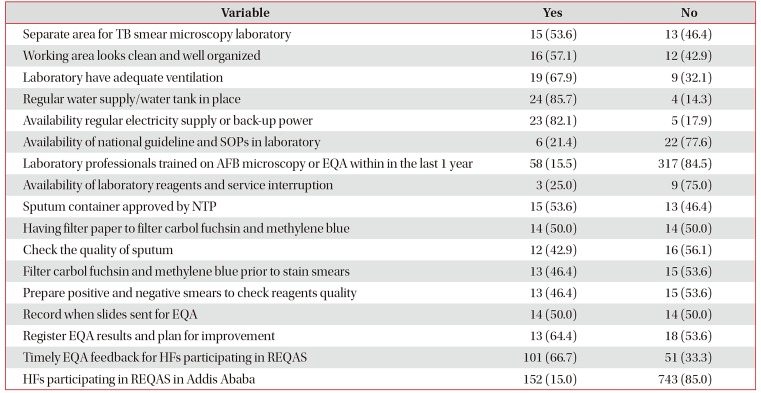
Table 4
Laboratory services quality same-day sputum smear microscopy, Addis Ababa, Ethiopia, September 2016 to July 2017
![]()
4. Diagnostic drop-out of same-day sputum smear microscopy in Addis Ababa, Ethiopia
From the total of 3,361 new presumptive TB patients registered in selected HFs after implementations of same-day sputum smear microscopy, 93 (2.7%) had submitted the first spot but did not submit second spot sputum specimen. One hundred sixteen (3.4%) did not submit any of the two spot sputum specimens. The overall diagnostic drop-out rate of same-day sputum smear microscopy among the newly diagnosed presumptive TB patients was 209 (6.2%).
The diagnostic drop-out rate was highest in private HFs. From the total of 691 new presumptive TB patients registered in private HFs 50 (7.2%) were dropped-out from diagnostic paths in contrast to 159 (5.9%) in public HFs. Among the total 209, diagnostic defaulter male and female accounted 44.9% and were 47.4% respectively as the detailed depicted in Table 5.
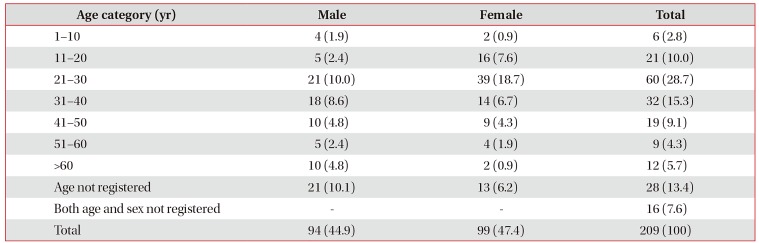
Table 5
Drop-out rate among sex and age category of the study participants, Addis Ababa, Ethiopia, September 2016 to July 2017
![]()
Go to :
Discussion
In this study, the diagnostic drop-out rate of the same-day sputum smear microscopy was 5.9% in public and 7.4% in private HFs with overall drop-out rate of 6.2%. It was much lower than study conducted in Pakistan with overall default rate of 12.9%9. The difference might be due to the difference in diagnostic approach. In the present study, the drop-out of same-day smear microscopy were reviewed in the study of Pakistan, the 2-day sputum smear microscopy approach was reviewed.
The finding of the present study was higher than the drop-out (2%) of the WHO same-day policy implementation1. The difference might be due to methodologies: in the present study, secondary data were reviewed from records in contrast to WHO randomized control trial study. The overall sputum smear microscopy reading agreement between peripheral laboratories and EQA centers 99.4% was concordant with the study conducted in west Amhara, Ethiopia, and Argentina with smear reading agreement 99.4% and 98%, respectively101112. However, it was higher than the study conducted in Eastern Ethiopia with smear reading agreement 94.5%13.
The agreement between peripheral laboratories and EQA centers for negative smear reading in the present study was 99.6%, was higher compared to, 42.9% of the study conducted in Tanzania and 95% of the previous study conducted in Addis Ababa1415. The difference could be attributed to training of laboratory professionals on AFB microscopy. Prior to implementation of same-day sputum microscopy, many training sections have been conducted to laboratory professionals by the region that might increase the performances. In Ethiopia, laboratory quality management was implemented after the previous study which might be contributed to the difference. However, the positive smear reading agreement 98.8% in the present study was in line with 100% of study in Tanzania and 99% of study in Addis Ababa1415.
The discrepancy might result from sample size, training laboratory professionals on microscopy. In the present study, a total of 7,551 sputum smear slides were collected for blinded rechecking whilst 578 ZN-stained sputum smear slides were rechecked in conducted study Eastern Ethiopia.
In the present study, the sensitivity, specificity, PPV and NPV of same-day sputum smear microscopy 97.4%, 99.6%, 96.3%, and 99.7%, respectively. It was higher than the study conducted in Eastern Ethiopia with sensitivity, specificity, PPV, and NPV of 83.5%, 97.8%, 91.7%, and 95.7%, respectively15. The difference could be due to laboratory professionals training on sputum smear microscopy which might vary from region to region, the work loads of smear microscopy and hired laboratory professionals might differ from region to region. Besides proper collection of sputum samples from suspected PTB patients, the preparation of good, uniform, thin smears, and staining of smears with high-quality staining reagents is imperative in precise reporting on microscopy16.
In this study, 7,524 of smears slides collected for EQA blinded rechecking, 2,523 (33.5%) had poor specimens quality which might result from specimen collected at any time of presumptive TB patient arrival (spot-spot) to HFs. Mucociliary clearance is high overnight hence spot-spot is less concentrated than morning specimens which might lead to poor specimens quality.
Timely feedback on supportive supervision and EQA coverage of the present study were 66.6% and 15%, respectively. It was comparable to the finding of the study conducted in west Amhara and Mekelle, Ethiopia indicating supportive supervision and timely feedback, internal and external quality assurance practices, equity in training and resource distribution were issues given less attention in these areas1718.
In this study lack of training on same-day approach, stock-outs of reagents and supplies and lack of sufficient human power as per workloads of laboratory professionals, motivation, risk allowance, inadequate space infrastructures were some of the challenges identified. Similar findings were reported from study conducted in Uganda on identified key health system barriers hindering TB service quality: stock-outs of drugs/supplies, inadequate space and infrastructure, lack of training, high workload, low staff motivation, and poor coordination of health center services1920.
In conclusion, in Addis Ababa, the diagnostic drop-out rate of same-day sputum smear microscopy was high. Strengthening EQA, sputum smear microscopy services quality in HFs, health education and promotion for presumptive TB patients on sputum provision, training of laboratory professionals on sputum smear microscopy reduces errors in sputum smear reading, increases case detection and plays a great role in the fight against TB.
Go to :
 XML Download
XML Download