

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
In 2018, approximately two million people worldwide were diagnosed with lung cancer, accounting for 11.6% of the total cancer incidence. The death toll from lung cancer was 1.76 million, accounting for 18.4% of all cancer deaths, and lung cancer remains the most common cause of cancer death to date1. Eighty-five percent of lung cancers are non-small cell lung cancer (NSCLC), more than 50% demonstrate distant metastasis at the time of diagnosis of lung cancer, and only 20% to 25% are identified at an operable stage.
In those who cannot be operated on, treatment options include chemotherapy, targeted therapy, and immunotherapy. Anti–programmed cell death protein 1 (PD-1) inhibitors (e.g., nivolumab and pembrolizumab) and anti–programmed death-ligand 1 (PD-L1) inhibitors (e.g., atezolimumab) are approved for the treatment of advanced unresectable melanoma and NSCLC. Objective response rate (ORR) with these options are 40% to 45% for first-line therapy in melanoma and 20% for second-line therapy in NSCLC patients who failed to show benefit with chemotherapy23456. Patients who relapsed after first- or second-generation epidermal growth factor receptor (EGFR)–tyrosine kinase inhibitor (TKI) treatment should perform T790M mutation test to confirm that third-generation EGFR-TKI is available 7. However, if the third-generation EGFR-TKI is not available, it is necessary to investigate whether it is applicable to the immune check point inhibitor.
Predictive biomarkers of immunosuppressive therapy have a method to identify tumor mutation burden (TMB), and there is a clinical benefit in the case of high mutational burden (≥178 nonsynonymous mutations) in whole-exome sequencing8. However, the measurement of TMB is expensive, and it has the disadvantage in representing intratumor heterogeneity, and is not standardized. So, PD-L1 expression measurement methods are widely used instead.
PD-L1 expression constitutes a potential predictive biomarker for the selection of PD-1/PD-L1 inhibitors. The correlation between PD-L1 expression level and the clinical efficacy of immunotherapy is well-known24910. In 2015, the Food and Drug Administration (FDA) approved a “companion diagnostic” method using the 22C3 clone for pembrolizumab and a “complementary diagnostic” method using the 28-8 clone for nivolumab. More recently, a “complementary diagnostic” test for atezolimumab was also approved. Because of this one drug/one diagnostic test co-development method, the cutoff values for significant results vary among the different tests and for different conditions. For example, the overall response rate of nivolumab is 16.7% in squamous cell carcinoma and 17.6% in nonsquamous NSCLC when a 5% cutoff is employed with the PD-L1 immunohistochemistry (IHC) SP263 assay10. Separately, in the case of pembrolizumab, a 50% cutoff in the PD-L1 IHC 22C3 pharmDx assay showed an ORR of 19.4%4. Regarding atezolimumab, 1% or more in tumor cell and 5% or more in tumor infiltrating immune cell staining in the PD-L1 IHC SP142 assay in the immune cells, and is established with an ORR of 15%11.
There have been recent efforts to match these three tests12. In the present research, the agreement between the PD-L1 IHC SP263 assay, the PD-L1 IHC 22C3 pharmDx assay, and the PD-L1 IHC SP142 assay were evaluated. We also analyzed the clinical significance of PD-L1 expression in EGFR mutant NSCLC.
Go to : 
Materials and Methods
1. Patients and materials
We analyzed the results of 230 patients who were (1) pathologically confirmed to have NSCLC; (2) tested using the PD-L1 IHC 22C3, SP263, and SP142 methods; (3) evaluated for peptide nucleic acid (PNA) clamping method to confirm EGFR mutation; and (4) provided informed consent to undergo PD-L1 and EGFR mutation testing. All data were gathered in accordance with the amended Declaration of Helsinki, following approval of the study by an independent hospital Institutional Review Board (approval no. 3-2018-0260). The need for written informed consent was waived because of the retrospective design of the study.
2. PD-L1 IHC
The PD-L1 assay when performed in Korea employs three test methods, as follows: the VENTANA PD-L1 (SP263) assay, the PD-L1 IHC 22C3 pharmDx assay, and the VENTANA PD-L1 (SP142) assay. Each test is used as a companion diagnosis for nivolumab (Opdivo, Bristol-Myers Squibb, New York, NY, USA), pembrolizumab (Keytruda, Merck, Kenilworth, NJ, USA), and atezolimumab (Tecentriq, Genentech, San Francisco, CA, USA), respectively. The combined use of these tests is challenging, increasing both social costs and efforts and impeding the interpretation of test results. In order to confirm consistency, correlation analysis was performed between the three PD-L1 test methods.
Detection and quantification of the proportion of immunoreactive tumor cells was performed according to the manufacturer's recommendations. Briefly, neoplastic cells were considered positive when cell membrane staining was present and negative when cytoplasmic immunoreaction was present13. PD-L1 expression was determined using the tumor proportion score (TPS), which is the percentage of viable tumor cells showing partial or complete membrane staining14. A specimen was considered PD-L1–positive with ≥50% of viable tumor cells exhibited membrane staining at any intensity (i.e., when TPS ≥50%); conversely, a weak PD-L1–positive result was when 1%≤ TPS<50%. In this study, we assigned two categories according to the TPS 1% cutoffs.
3. EGFR PNA clamping test
A PNA Clamp EGFR Mutation Detection Kit (PANAGENE, Inc., Daejeon, Korea) was employed to detect EGFR mutations by real-time polymerase chain reaction, as previously described15.
4. Statistical analyses
Clinical characteristics and associations with biomarkers were examined by comparing differences using Fisher exact test or an independent sample t-test. To evaluate the relationship between PD-L1 expression level ascertained with the 22C3, SP263, and SP142 assays, the Shapiro–Wilk test was applied to evaluate the distribution of variability, while the Pearson correlation test was used to test relationships between two variables. All tests were evaluated on two arms. A p-value of less than 0.05 was considered to be significant. Statistical analysis was performed using the Statistical Package for the Social Sciences version 23 software program (IBM Corp., Armonk, NY, USA).
Go to :
Results
1. Patient characteristics
To confirm the clinical features of overexpression of PD-L1 in Korean patients with NSCLC, we analyzed the results of 230 patients who were diagnosed with NSCLC and underwent both PD-L1 expression test and EGFR mutation test at two hospitals under the jurisdiction of the Yonsei Medical Center. The demographic characteristics of the patients are presented in Table 1. The median age of the patients was 64.5 (50.8–72.8) years, 138 (60.0%) were male, and 124 (53.9%) had a smoking history. Histologic types were 194 cases of adenocarcinoma (85.1%) and 32 cases of squamous cell carcinoma (14.0%). The pathologic stage was stage I in 23 (10.0%), stage II in nine (3.9%), stage III in 37 (16.1%), and stage IV in 161 (70.0%). EGFR tyrosine kinase domain was detected as wild type in 164 (71.3%) and EGFR mutant in 66 (28.7%) by PNA clamping method. The type of EGFR-TKI sensitizing mutation were E19del in 33 (50.0%), L858R in 23 (34.8%), and others in 10 (15.2%), respectively.
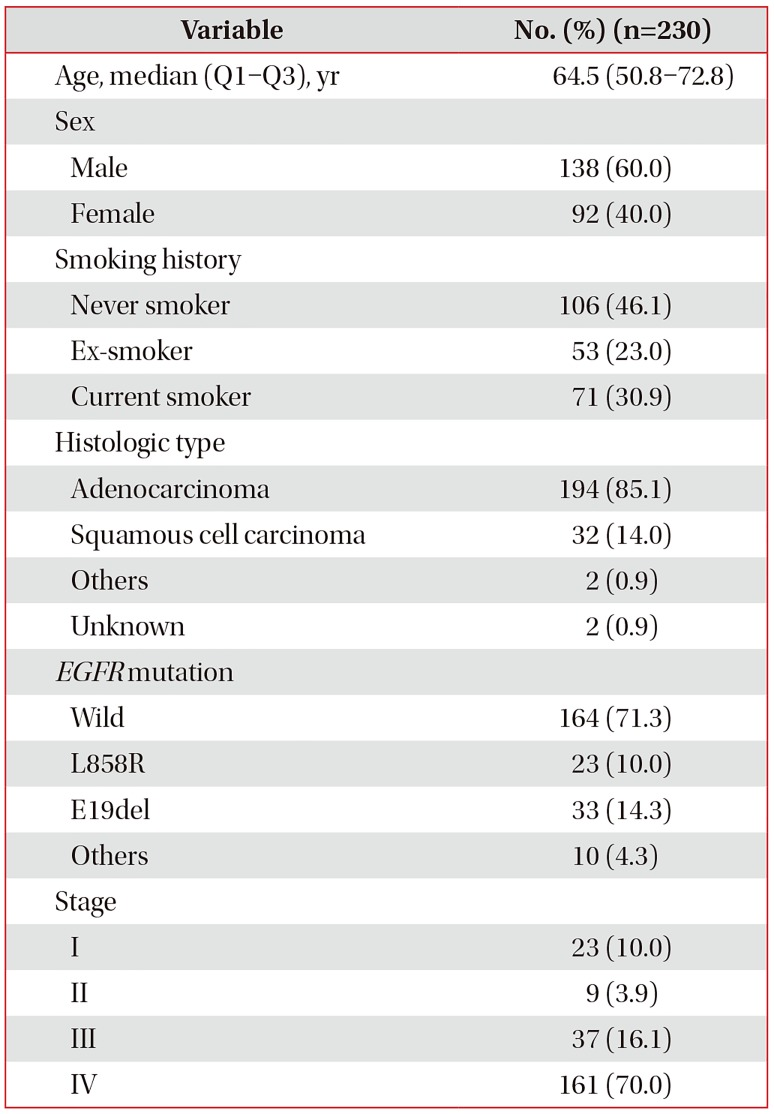
Table 1
Baseline characteristics
![]()
2. PD-L1 expressions in 22C3 and SP263 were significantly correlated
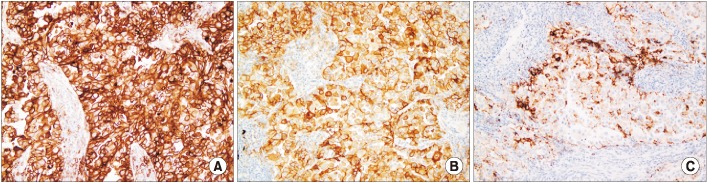
The VENTANA PD-L1 (SP263) assay was performed in 164 patients, the PD-L1 IHC 22C3 pharmDx assay was performed in 230 patients, and the VENTANA PD-L1 (SP142) assay was performed in 53 patients. Of these, 164 patients underwent both VENTANA PD-L1 (SP263) assay and PD-L1 IHC 22C3 pharmDx assay, and the scatter graphs of these two test's results are shown in Figure 1. The photographs of PD-L1 IHC staining by each method are shown in Figure 2.
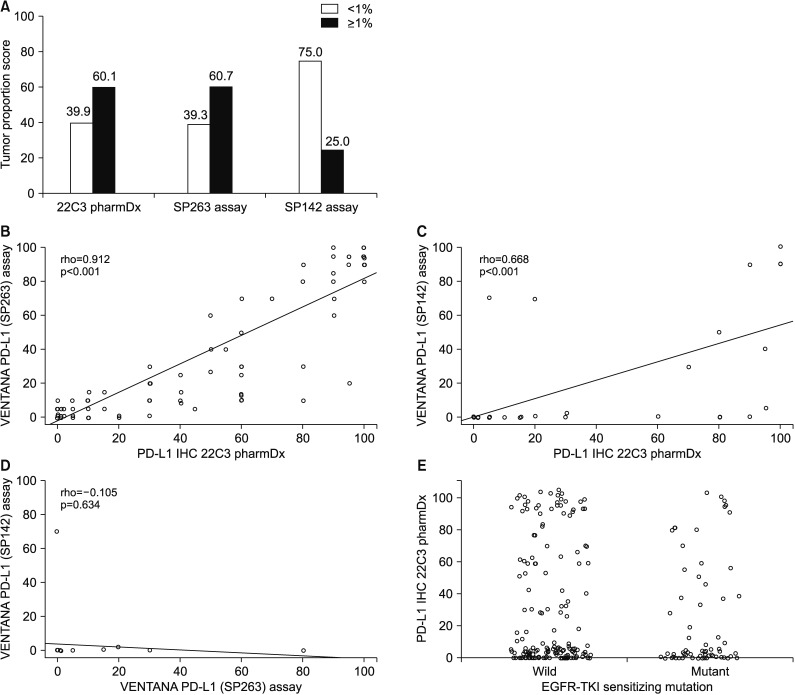 | Figure 1Prevalence and correlation of programmed death-ligand 1 (PD-L1) expression using the 22C3 pharmDx, SP263, and SP142 assays. (A) The rate of PD-L1 expression with cutoff tumor proportion score of 1% using the 22C3 pharmDx assay, SP263 assay, and SP142 assay. (B) Scatter diagrams illustrating the correlation between expression levels according to 22C3 pharmDx and SP263 assays, 22C3 pharmDx and SP142 assays (C), and SP263 and SP142 assays (D). (E) PD-L1 expression by 22C3 assay according to epidermal growth factor receptor (EGFR) mutation. IHC: immunohistochemistry; TKI: tyrosine kinase inhibitor.
|
Of note, there was a statistically significant higher correlation (rho=0.912; p<0.001, Spearman correlation) in the results of 164 patients who underwent both 22C3 and SP263 tests, and the derived regression equation was as follows: 22C3=5.578+1.009×SP263 (R=0.920, p<0.001). In our data, concordance rate between 22C3 and SP263 assays was 81.6%. The VENTANA PD-L1 (SP142) assay, a complement diagnosis method for atezolimumab, was approved by the FDA in October 2016 and has recently covered by insurance in Korea. Therefore, the number of subjects who underwent the SP142 test was relatively small in comparison. The correlation of PD-L1 expression values was analyzed in 52 patients who performed both 22C3 and SP142 assays. The correlation coefficient (R) was 0.668 (p<0.001) and concordance rate was 86.5% between SP142 and 22C3 assays. In addition, only 23 patients underwent both SP263 and SP142 tests, the correlation coefficient between SP142 and SP263 was −0.105 (p=0.634).
There was a significant correlation between 22C3 and SP263 assays and between 22C3 and SP263 assays. Therefore, it is desirable to integrate these test methods. However to integrate between SP263 and SP142 assays, it is necessary to require additional data to be accumulated.
3. Relationship between EGFR sensitizing mutation and PD-L1 expression in NSCLC
According to previous research, patients with NSCLC with EGFR-TKI sensitizing mutations are well-known to have characteristics of young age, no smoking history, and a lower mutation burden versus those with the EGFR wild type1617. These characteristics were predicted to affect PD-L1 expression, and we analyzed the effects of EGFR-TKI sensitizing mutation on PD-L1 expression using the 22C3 test. In our data, 230 patients with NSCLC who underwent PD-L1 IHC 22C3 pharmDx assay were divided into EGFR wild group and EGFR mutant group (Table 2). The clinical features of the EGFR mutant group were younger age (62.4±1.16 vs. 66.1±0.78) and higher percentage of never smoker (71.2% vs. 36.0%) than the EGFR wild group. These clinical characteristics were in good agreement with the characteristics of the commonly known EGFR mutant NSCLC. The expression of PD-L1 (22C3 pharmDx assay: TPS ≥1%) was 62.8% (103/164) in EGFR wild type and 54.5% (36/66) in EGFR mutant type and there was no difference in PD-L1 expression according to EGFR-TKI mutation (p=0.156).
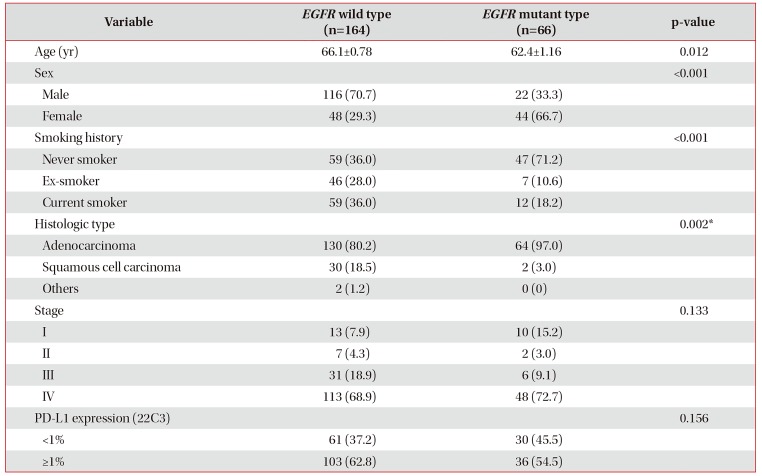
Table 2
Clinical characteristics of NSCLC patients with EGFR-TKI sensitizing mutation
![]()
The clinical features of the NSCLC patients who underwent 22C3 pharmDx assay divided by PD-L1–negative group (TPS<1%), PD-L1–positive group (TPS≥1%) were shown Table 3. There was no significant difference in the clinical characteristics (age, sex, smoking status, EGFR mutation) of patients according to PD-L1 expression. Therefore, in patients with EGFR-TKI sensitizing mutations, PD-L1 expression tests should be performed and immunotherapy should be considered as a treatment for NSCLC.
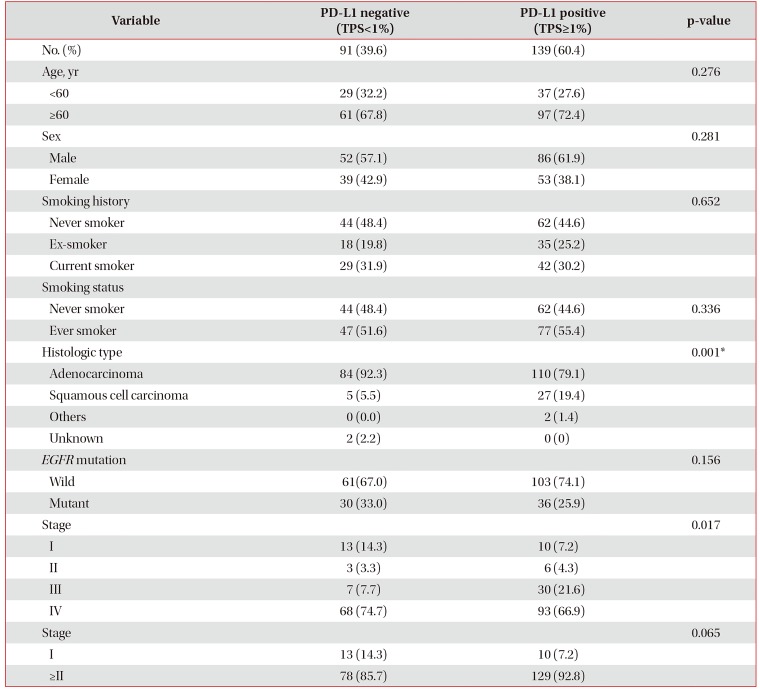
Table 3
Clinical characteristics of NSCLC patients with PD-L1 expression using 22C3 pharmDx assay
![]()
4. Effect of PD-L1 expression on EGFR-TKI response
The expression of PD-L1 in tumor cells is a defense mechanism against the host immune system and the overexpression of PD-L1 is well-known to be a poor prognostic factor18. To investigate whether this phenomenon is applicable in patients treated with EGFR-TKI, progression-free survival (PFS) and overall survival (OS) were analyzed in the context of PD-L1 expression in 69 patients taking EGFR-TKI. Forty-six of the patients (66.7%) received first-line treatment. EGFR-TKI types were gefitinib in 44 (63.8%), erlotinib in 15 (21.7%), and afatinib in 10 (14.5%). The mean OS of patients treated with EGFR-TKI was 60.5±6.8 months (95% confidence interval [CI], 47–74). Separately, the median PFS of patients taking EGFR-TKI was 10 months (95% CI, 7.7–12) in the PD-L1–negative group and 8 months (95% CI, 5.1–11) in the PD-L1–positive group (Figure 3C). The mean OS of EGFR-TKI treated patients was 69.2±7.8 months (95% CI, 54.0–84.5) in the PD-L1–negative group and 33.7±3.0 months (95% CI, 28.0–39.5) in the PD-L1–positive group (Figure 3D). Thus, PD-L1 expression showed poor prognosis and survival but no statistical significance (p=0.529 vs. p=0.150). Additionally, the OS was 81.3±8.1 months in the PD-L1–negative group and 57.2±8.8 months in the PD-L1–positive group (Figure 3B), but this was also not statistically significant (p=0.202). In conclusion, the expression of PD-L1 did not affect the EGFR-TKI response.
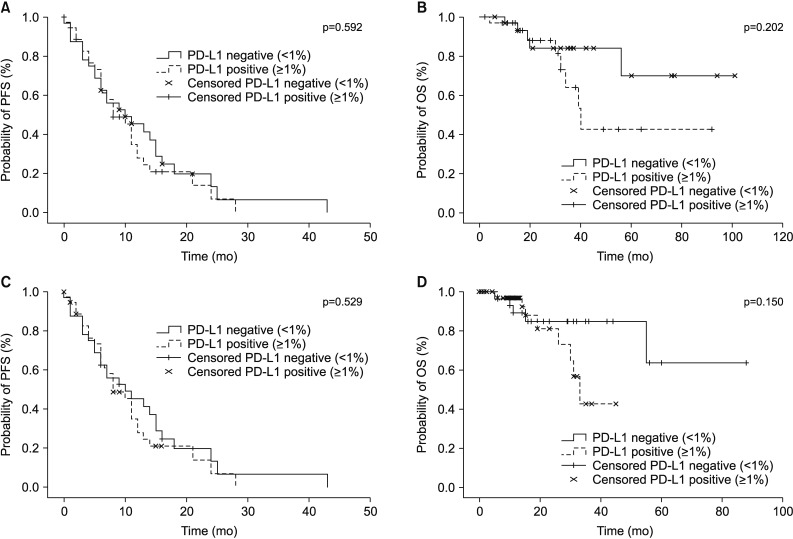 | Figure 3Kaplan-Meier curves of progression-free survival (PFS) and overall survival (OS) according to programmed death-ligand 1 (PD-L1) expression status in non-small cell lung cancer patients. The p-value for the difference between the two curves was determined using the log-rank test. (A) PFS for overall population. (B) OS for overall population. (C) PFS for patients treated with epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI). (D) OS for patients treated with EGFR-TKI.
|
Go to :
Discussion
In this study, we analyzed the PD-L1 expression and clinical characteristics of Korean patients with NSCLC. Of the 230 patients whose samples were evaluated for PD-L1 using the IHC 22C3 pharmDx assay, 67 (29.1%) had a PD-L1 TPS of 50% or greater and 139 (60.4%) had a PD-L1 TPS of 1% or greater. Herbst et al.9 reported that more than 50% of PD-L1 expression was seen in 28% and that of more than 1% was seen in 70% of patients, respectively. Reck et al.19 also reported a TPS expression of PD-L1 of 50% or more in 30.2% of patients. Thus, the prevalence of PD-L1 expression in Korean NSCLC was consistent with other findings from previous studies.
Result of PD-L1 IHC 22C3 pharmDx assay was significantly correlated with that of PD-L1 IHC SP263 assay. A blueprint project assessed the comparability between 22C3, 28-8, SP263, and SP142 and a correlation between three tests excepting SP142 was verified. The reason for excluding SP142 was that it showed weak staining on the tumor cell membrane and fewer positive tumor cells in comparison with the other assays12. This study showed a correlation between 22C3 and SP263 assays and between 22C3 and SP263 assays in the real world, so it is desirable to integrate PD-L1 tests. Therefore, if one of the three PD-L1 tests is negative, it is necessary to perform the other tests. However, to integrate between SP263 and SP142 assays, it is required to accumulate additional data.
Many previous studies have reported the association of PDL1 expression with EGFR mutation status. Experimental results have shown that EGFR mutation induces PD-L1 expression202122. Azuma et al.20 reported that PD-L1 expression was significantly higher in patients with clinical features of EGFR mutant NSCLC including female gender, no smoking history, and adenocarcinoma. Separately, Tang et al.23 indicated that PD-L1 expression was not correlated with sex, smoking history, or histopathological type, but was higher in EGFR mutants in advanced NSCLC. Zhang et al.24 found that PD-L1 expression was not correlated with sex, smoking status, or EGFR mutation in early-stage adenocarcinoma. Our results using tissue from NSCLC patients also showed PD-L1 expression had no association with sex, smoking status, or EGFR mutation.
Because EGFR mutant NSCLC is expected to have a low mutation burden, PD-L1 expression is expected to also be lower. However, there was no difference in PD-L1 expression in NSCLC according to EGFR mutation type in our study. There are several possible reasons for these different outcomes. First, Akbay et al.21 and Azuma et al.20 reported that PD-L1 expression was higher in the EGFR mutant NSCLC cell line and that EGFR-TKI inhibitors reduced PD-L1 expression. However, since the human NSCLC cell line has fewer mutation burdens than NSCLC patients, such may infer an inverse relationship between EGFR mutation and PD-L1 expression. Second, Azuma et al.20 enrolled early-stage NSCLC patients who underwent surgical resection; in contrast, most of our data included advanced-stage (77.4%) NSCLC patients. This difference in stage may have affected the outcome. Third, previous studies have employed different methods of IHC staining and applied different cutoff values. Tang et al.23 used a rabbit monoclonal anti-human antibody (1:200, E1L3N, Cell Signaling Technology, Danvers, MA, USA) and applied a cutoff value of more than 5% for the H-score. Separately, Ji et al.25 incorporated mouse polyclonal antibodies and reagents purchased from Abcam, Inc. (Cambridge, UK; i.e., CAT nos. ab137132 for anti-PD-1 antibody and ab174838 for anti-PD-L1 antibody) and their cutoff value was at least 5% of the H-score. In contrast, our study used PD-L1 expression as a standardized method for PD-L1 IHC 22C3 pharmDx assay and applied a more than 1% expression as a cutoff value.
There were many reports of conflicting results in relation to PD-L1 expression and prognosis in NSCLC. Azuma et al.20 determined that NSCLC patients with high PD-L1 expression showed significantly shorter OS than did those with low PD-L1 expression (median, 55.9 months vs. 72.6 months; p=0.039). Lin et al.26 found that PD-L1 expression was associated with a good prognosis in lung adenocarcinoma treated with EGFR-TKI in terms of both PFS and OS (post-TKI PFS: 16.5 months vs. 8.6 months; p=0.001 and OS: 35.3 months vs. 19.8 months; p=0.004). Although PD-L1 overexpression induces immune escape, which is presumed to have a poor prognosis, the results of this study did not reveal a significant correlation with PD-L1 expression and prognosis. In addition, the PD-L1 expression was not related to the post-TKI recurrence and post-TKI survival in patients treated with EGFR-TKI. The effect of EGFR-TKI on the EGFR signaling pathway might be a major factor in lung cancer treatment response. Therefore, the effect of PD-L1 expression on the target therapy response would be minimal.
The results of the IHC PD-L1 22C3 and SP263 assays are considered to be in good correlation with each other. Since PD-L1 expression does not affect the EGFR mutation, it is necessary to perform a PD-L1 test and set the treatment direction in patients with EGFR mutant NSCLC.
Go to :
 XML Download
XML Download