

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The non-cooperative attitude in children during dental care is mainly attributed to anxiety over the treatment. This attitude is not outwardly manifested as behavior when the anxiety is mild but can vary from passive refusal to treatment to anger attacks, when the anxiety is severe [1]. Anxiety-induced non-cooperative attitude can persist even in adulthood, hence leading to medical avoidance that is caused by extreme dental fears, and in turn leading to secondary problems, such as worsening oral health. Therefore, successful treatment during childhood using appropriate measures is necessary to alleviate lasting anxiety.
Since 2011, the present research team has been using Kleinknecht's 20-item Dental Fear Survey questionnaire [2] for adolescent dental anxiety. A previous study focused on children, which revealed the fears of the youth. The results showed that male middle school students in Gyeonggi-do showed higher levels of dental fear compared with female students (P < 0.05). In addition, dental professions have been shown to elicit dental fears even in areas that are not generally thought of as being related directly to treatment in dental offices [3]. However, as the previous study was confined to Gyeonggi-do students, it was limited in terms of representing the youth nationwide. Therefore, in subsequent studies, the study area was expanded. The results similarly showed a difference between men and women in the category of “Currently Induced Dentistry” (P < 0.05) [4]. The team also questioned the application of the existing Kleinknecht's 20-item Dental Fear Survey. A literature review showed that the validity and reliability of the questionnaire translated into Korean were unverified. Based on the high validity of the study, the newly created survey model was named Korean Dental Fear Survey (K-DFS) [5]. Studies have focused on the dental profession, but the factors of the dental profession with validated questionnaires still needed to be identified. Especially, a higher level of interpretation should be applied to dental clinics compared with the general dentistry field. Toward this end, the Kim et al. research was conducted in 2017 [6].
The present study aimed to evaluate the dental fear experienced by Korean adolescents and to identify the factors relevant thereto. Dental fear is likely formed during visits to the dentist's office or through previous experience of dental treatment. Therefore, to reduce the fear associated with dental treatment in adolescents, a proper environment in dental clinics and patient management programs need to be established. Thus, this study applied the K-DFS developed in a previous study to the national youth to draw conclusions the dental fear of Korean adolescents.
Go to : 
MATERIALS AND METHODS
1. Participants
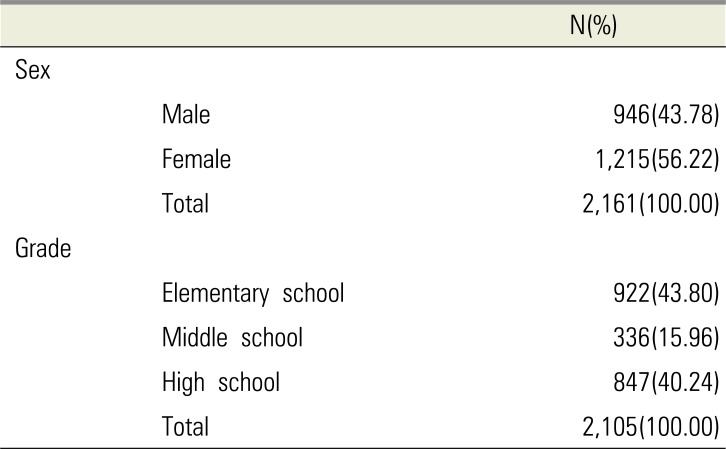
This study was carried out across Korea and focused on students aged 11 to 17 years (fifth and sixth grades in elementary school, middle school, and high school). The survey had been conducted since 2011. This study was approved by the Institutional Review Board of Wonkwang University (W-1411-003-001). The survey was conducted in advance through direct facilitation by the researchers, and the completed questionnaires were collected directly on site. The survey used data from 946 male students (43.78%) and 1,215 female students (56.22%) for a total of 2,161 students (Table 1).
2. Methods and Materials
2.1. Measuring Tool
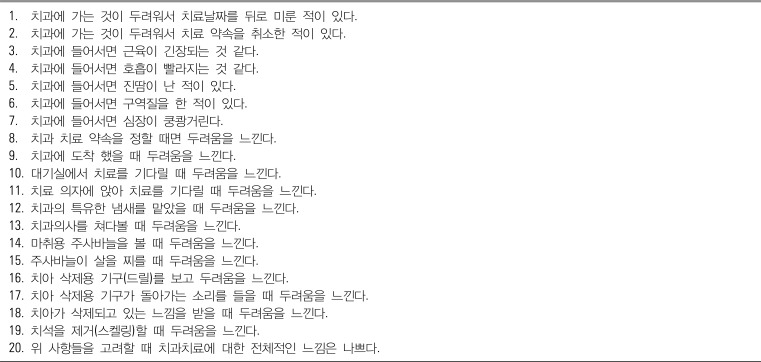
The K-DFS [5] is a translation of the dental fear survey scale developed by Kleinknecht et al. [2]. The questionnaire has 20 questions distributed under three categories. Each question is scored using a five-point Likert scale depending on the degree of dental fear: Not at all (one point); Almost not (two points); Normal (three points); Mostly yes (four points); and Always (five points). In the present study, the weight of each question was assumed to be equal in calculating the fear score.
2.2. Statistical Analysis
Regarding dental fear, the mean and standard deviation from descriptive statistical analyses were calculated. Cross-sectional analysis was performed to determine the distribution of dental visits and dental fear. Factor analysis was conducted to identify the underlying components of dental fear. VARIMAX was selected among orthogonal factor rotations. Reliability analysis of the lower components was performed as well. Independent t-test and one-way ANOVA were performed to analyze the differences in the lower components according to sex and grade. Logistic regression was used to analyze the factors affecting the fear of dental visits. All statistical analyses were performed using Stata 14.0 (StataCorp, College Station, TX, USA).
Go to :
RESULTS
The distribution of dental visits and dental fears indicated that 93.94% (2,030) of the participants had visited dentists and 57.09% (1,159) had fears associated with dentistry (Table 2). Through factor analysis, dental fear was divided into three subcomponents: (1) Avoidance behavior; (2) Association with dental treatment; and (3) Fear of dental stimuli. The corresponding reliability scores were 0.847, 0.933, and 0.880, respectively (Table 3). Differences in fear levels according to sex were higher in boys' fear behavior scores than in girls' regarding dental treatment (P < 0.05). Participants with dental fear had higher scores for items associated with dental treatment and fear of dental stimuli compared with participants without dental fear (P < 0.05). Differences were observed among the three groups (P < 0.05) (Table 4). However, logistic regression analysis showed that the results were not statistically significant for dental visits based on sex, grade level, and other subcomponents (P > 0.05)(Table 5).
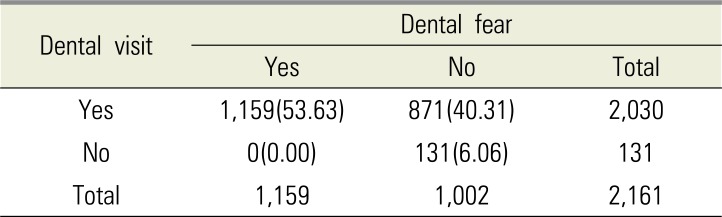
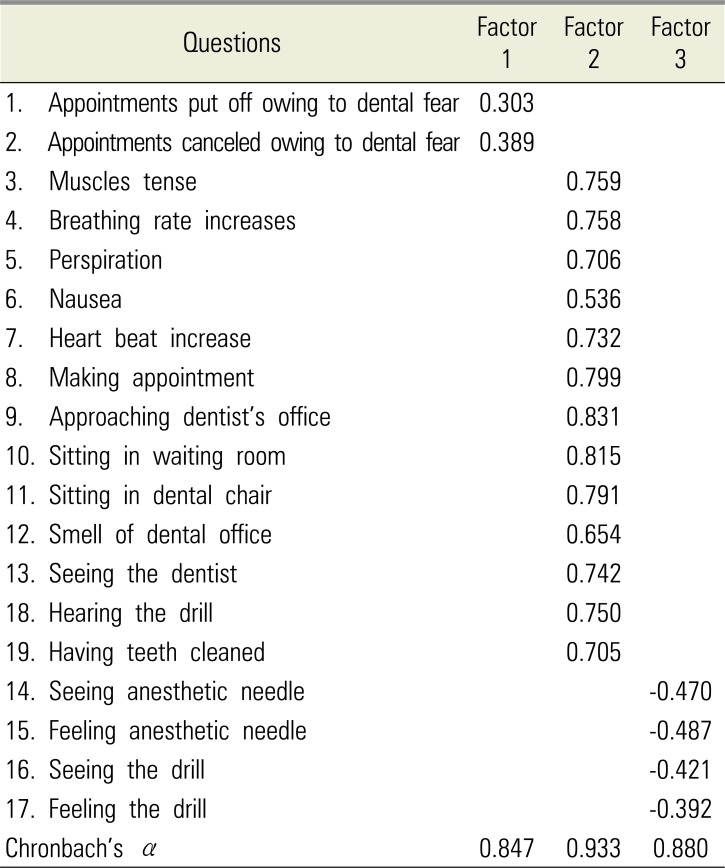
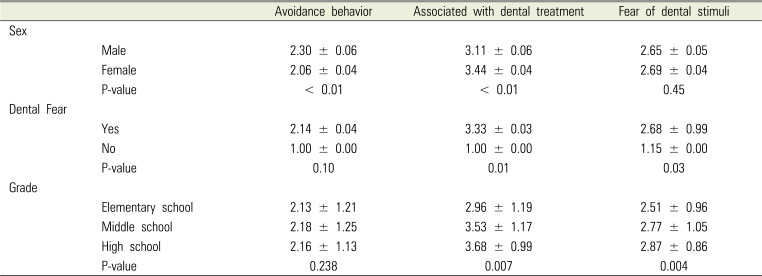
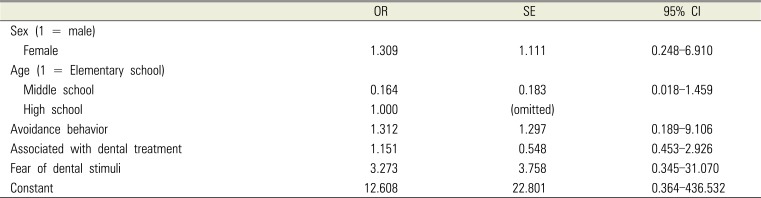
Table 2
Dental visit and dental fear of participants
| Dental visit | Dental fear | ||
|---|---|---|---|
| Yes | No | Total | |
| Yes | 1,159 (53.63) | 871 (40.31) | 2,030 |
| No | 0 (0.00) | 131 (6.06) | 131 |
| Total | 1,159 | 1,002 | 2,161 |
![]()
Table 3
Exploratory factor analysis results and reliability
![]()
Table 4
Mean dental fear survey scale (DFS) item scores by demographic feature and factor
![]()
Table 5
Factors affecting dental fear
![]()
Go to :
DISCUSSION
Individuals who have symptoms of phobia associated with dental care and dentistry are often referred to as dentists [7]. Locker et al. [8] found that more than half of the phobias are expressed before adolescence, whereas the rest are expressed during adolescence and adulthood, with about 16% of adults suffering from phobias. Klingberg et al. [9] reported that 17% of school-aged children have a severe fear of dental treatment. In the present study, more than 50% of the youth nationwide had dental fears—higher than the rate for preschool children and adults. This finding may be attributed to adolescents not yet maturing psychologically and physically. An issue of concern is that adolescents have a higher frequency of emergency visits [10] compared with X. Another is that tooth extraction and filling treatment experience rates are higher in those with low fear levels [11]. Meanwhile, dental phobia is more common in women than in men [12], and in general, younger people are more likely to be susceptible compared to older people [13]. The present results showed that differences in dental fear based on the subcomponents were unfounded.
However, the result of dental fear in accordance with the lower components was due to the K-DFS's structural limitations. The items in Kleinknecht's 20-item Dental Fear Survey [2], the predecessor of the K-DFS, can be categorized into three subgroups. The first is related to patterns and anticipated anxiety in avoiding dental treatment. The second considers psychological anxiety and agitation during dental treatment. The third pertains to fear associated with specific dental treatment stimuli (e.g., smelling, seeing needles, and feeling the vibration of a dental drill). In general, the reason patients have dental phobia is the traumatic dental experience felt directly during dental treatment, such as tooth loss. Indirectly, auditory stimulation [14], visual stimulation [1516], low level of dental education [1718], indirect experience [19], and anxiety owing to loss of situational control [20] are influenced by the patient's distrust of doctors [16] and concern about health [16]. Therefore, the K-DFS is limited in terms of elucidating the factors of dental fear.
This study selected 2,161 adolescents of various ages as participants and increased the validity of the research results by expanding the scope of the study area nationally. By verifying the validity of the newly developed K-DFS, the present study confirmed the scale's significance as a dental fear questionnaire. Therefore, there can be no objection that the grounds for criticism have been established according to conventional wisdom. In future, however, developing and studying the content-related limits of K-DFS to overcome those for the factors of dental fear, especially pain, will help reduce dental fear in adolescents.
Go to :
 XML Download
XML Download