

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pain management is requisite for successful dental treatment. Local anesthetics alone or in combination with other agents are often used during endodontic treatment of irreversible pulpitis [12]. Inflammatory mediators in pulpitis provoke pain responses and inflammation and successful anesthesia is achieved in less than 20% of cases under these circumstances [3]. Systematic reviews and meta-analysis have previously compared articaine and lignocaine [45], the effect of pre-operative analgesics and those of inferior alveolar nerve block (IANB) [67], IANB with different agents and techniques [8], and the effect of supplemental infiltration [9]. The diversity of these reviews does not identify any single best agent and technique for the maxilla and mandible, and anesthetic failure has been a recurring concern. Consequently, clinicians have little evidence by which to direct care, and may resort to trial and error. Such inadequate pain control can lead to avoidance of dental care and fear of dental treatment.
Unfortunately, results from different meta-analysis fail to point to the best amongst various tested agents. Lignocaine, which has been commercially available for more than 60 years and is commonly used, has been reported to be more successful when used with supplemental articaine infiltration [1011]. However, articaine infiltration alone also produced successful anesthesia in individual studies [111213]. Oral administration of non-steroidal anti-inflammatory drugs (NSAIDs) with lignocaine inferior alveolar block (IANB) has also been shown to improve anesthetic success [67]. Although patient-related factors, such as medical conditions, medications for systemic conditions, anatomical factors, and psychological factors, such as fear and anxiety [123] play an important role, the agent and the technique that was used successful in the majority of the population should be the first option adopted by clinicians, to produce more predictable results.
In comparison to traditional meta-analysis, network meta-analysis (NMA) may offer improved understanding of the best agents and techniques to use for anesthesia for irreversible pulpitis. The NMA principle is used for direct as well as indirect comparisons between multiple treatments from individual trials, using the common comparator principle [14]. The methodology of NMA provides a means to gain insight into relations and comparisons among randomized controlled trials [1415]. Hence, we performed an NMA to combine the available evidence on agents and techniques that produce successful pulpal anesthesia in the maxilla and mandible, in order to identify the best amongst these statistically, to form the basis for future clinical trials.
Go to : 
METHODS
1. Information sources and search strategy
The protocol for this review was registered with PROSPERO (registration number CRD42017057700). A literature search was conducted in Medline (through PubMed), Cochrane CENTRAL, and Google Scholar databases, up to April 1, 2017. The search strategy used was ((((irreversible pulpitis) AND (endodontic (treatment OR therapy) OR root canal OR pulp therapy)) AND pain) AND (local (anesthesia OR anesthesia))). Only studies published in English language were considered. The reference lists from the identified articles were manually screened to identify other eligible studies. Manual searches were also conducted to identify missed studies. Two authors carried out independent search and retrieved appropriate articles.
2. Eligibility criteria
The criteria for inclusion were randomized controlled trials conducted in adult patients of any age and sex, with any tooth/teeth diagnosed with symptomatic irreversible pulpitis, based on subjective methods such as a pain scale and/or objective testing, using heat, cold, or electric pulp testing, and requiring endodontic treatment. Studies comparing different local anesthetic agents; techniques of administration; combination of local anesthetics with other orally administered medications, such as analgesics, nitrous oxide, acupuncture, or others were included. Traditional subjective methods of testing success of anesthesia included testing lip numbness, responsiveness of the mucosa to needle sticks, or simply commencing with the treatment and looking for a pain response [1213]. Although objective methods, such as electric and heat/cold pulp testing are more reliable, they are more commonly used as diagnostic aids [1234]. The primary outcome in the present meta-analysis was “no” or “mild” pain during endodontic access or canal preparation, measured using a visual analog scale (VAS), which is also subjective, or objective negative testing, using a pulp tester. This outcome was adopted as this was the primary outcome in the majority of the included studies. Studies conducted in children, pregnant and lactating women, patients with medical conditions, anxious patients on anti-anxiety medications, patients on any other medications interfering with the action of local anesthetics or the drugs administered were excluded.
3. Study procedure and statistical considerations
After a thorough literature search by both investigators independently, a pre-tested data extraction form was created and the following data were extracted from each eligible study: trial site, year, trial methods, participants, interventions, and outcomes. Disagreement between the investigators was resolved through discussion to consensus. The present review and NMA is presented as per the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines [16]. Risk-of-bias of the included randomized trials was assessed using the Cochrane risk-of-bias tool [17]. Heterogeneity between directly compared studies was assessed using Chi-square and I2 tests. The inverse variance heterogeneity model was used, as it does not require any assumptions and is more robust than the random-effects model for both direct and indirect comparisons. Direct comparison estimates were derived by pooling the data from studies that compared the same intervention. Indirect comparison pooled estimates were derived by pooling the data between the studies through a common comparator. The entire NMA was carried out using MetaXL. Odds ratios and 95% confidence intervals were used to estimate effects, as the outcome is a categorical variable. Inconsistencies between the direct and indirect pooled estimates were evaluated by H-statistics, wherein a value of < 3 was considered as minimal, 3–6 as modest, and > 6 as gross inconsistency. The Gradings of Recommendation, Assessment, Development and Evaluation (GRADE) working group approach was used to assess the quality of evidence [17].
Go to :
RESULTS
1. Search results
Sixty-two studies were considered for inclusion [1819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364656667686970717273747576777879]; 53 studies involving 4465 patients investigated the mandible [1819202122232425262728293031323334353637383940414243444546474849505152535455565758596061626364656667686970], eight studies involving 442 patients investigated the maxilla [7172737475767778], and one study [79] involving 51 patients included both maxillary and mandibular teeth. One study [48] was excluded because of disconnected network (the treatments included in this study [48] did not form a connected network, such that there was a path from each treatment to every other treatment within the whole network), and hence 61 studies were included in the final meta-analysis. The detailed search results are presented in Figure 1. Key characteristics of the included studies are represented in Table 1. Risk-of-bias assessment demonstrated low risk in all domains for most of the studies (Fig. 2).

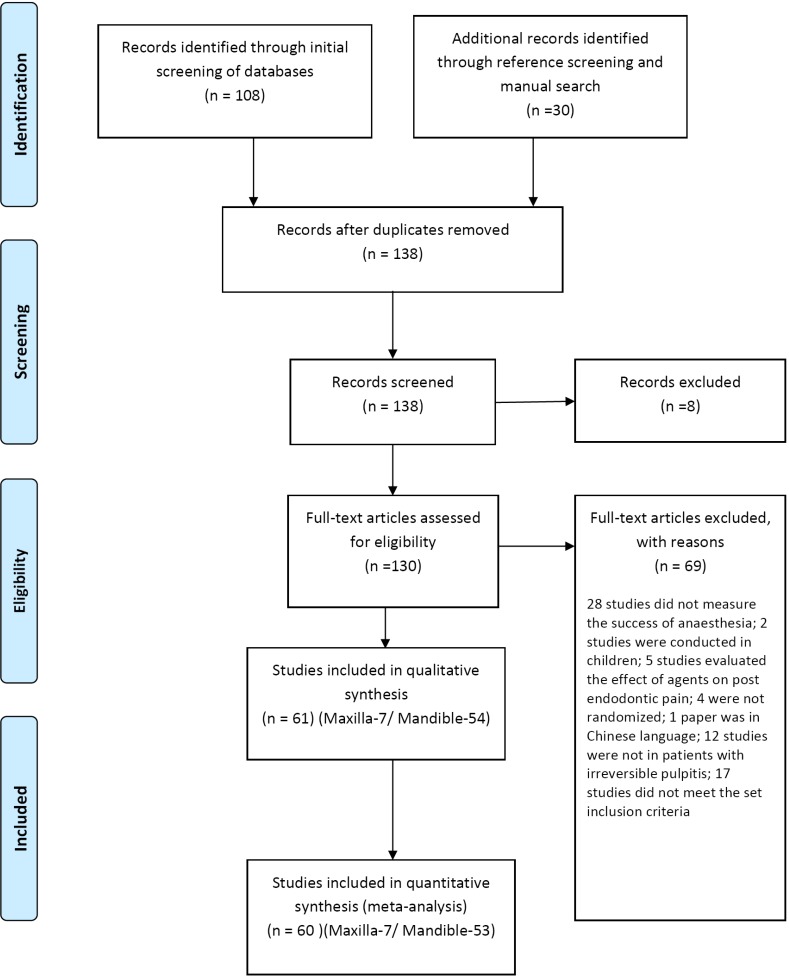
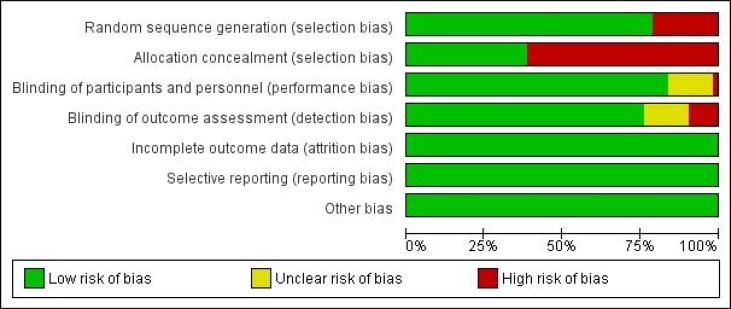
Table 1
Key characteristics of included studies
| Study NO | First author, year [reference] | Sample size/population | Area of anesthesia | Symptomatic/Asymptomatic | Intervention | Comparator | Anesthetic agent used | Definition for anesthetic success |
|---|---|---|---|---|---|---|---|---|
| Studies in the mandible | ||||||||
| 1 | Click V, 2015 [18] | 98 | Mandibular molar or premolar | Symptomatic | 60 patients received Gow–Gates and BNB | 38 patients received Akinosi Vazirani and BNB | 2% lignocaine with 1:100 000epinephrine | access and instrument the tooth with no or mild pain, using VAS scale |
| 2 | Aggarwal, 2010 [19] | 76 | Mandibular molar | Symptomatic | 27 patients received Gow-Gates, 25 received Vazirani-Akinosi | 24 patients received IANB | 4% articaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using |
| 3 | Matthews, 2009 [20] | 78 | Mandibular molar or premolar | Symptomatic | 55 patients received IAN and long buccal and supplemental BI | 23 patients received IANB and long buccal | 2% lignocaine with 1:100 000 epinephrine. | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| Supplemental BI with 4% articaine with 1:100 000 epinephrine | ||||||||
| 4 | Aggarwal, 2011 [21] | 98 | Mandibular molar | Symptomatic | 24 patients supplemental BI 4% articaine with 1:100 000 ephinephrine. | 24 patients did not receive any supplemental infiltrations | All patients received IANB with 2% lignocaine with 1:200 000 epinephrine | No pain or weak/mild pain during access and instrumentation using VAS scale |
| 26 patients with 1 mL/30 mg of ketorolac tromethamine | ||||||||
| 24 patients with 1 mL/4 mg of dexamethasone. | ||||||||
| 5 | Razavian, 2013 [22] | 40 | Mandibular posterior tooth | Symptomatic | 20 patients received X tip IO injection | 20 patients received IANB | 2% lignocaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 6 | Webster, 2016 [23] | 175 | Mandibular molar or premolar | Symptomatic | 75 patients received conventional IANB and intraseptal 1.4 mL 4% articaine with 1:100 000 epinephrine | 100 patients received IANB | 2% lignocaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 7 | Reisman, 1997 [24] | 86 | Mandibular molar or premolar | Symptomatic | 42 patients received IANB and IO of 1.8 ml of 3% mepivacaine | 44 patients received IANB | 2% lignocaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 8 | Parirokh, 2014 [25] | 69 | Mandibular molar | Mentioned as asymptomatic but included patients with prolonged response to cold test. Hence considered symptomatic | 33 patients received IANB followed by BI and intraligamentary | 36 patients received IANB | 2% lignocaine with 1/80 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 9 | Aggarwal, 2009 [26] | 87 | Mandibular molar | Symptomatic | 62 patients received IANB. | 25 patients received | 2% lignocaine with | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 31 patients received supplemental infiltrations of 2% articaine with 1:200 000 epinephrine, and 31 patients received infiltrations of 2% lignocaine with 1:200 000 epinephrine | IANB | 1:200 000 | ||||||
| 10 | Parirokh, 2010 [27] | 82 | Mandibular molar | Symptomatic | 55 patients received IANB and BI | 27 patients received IANB | 2% lignocaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 11 | Kanaa, 2012 [28] | 100 | Mandibular molar or premolar | Symptomatic | 25 patients received IANB and BI of 4% articaine with epinephrine 1:100 000 | 25 patients received IANB | 2.0 mL of 2% lignocaine with 1:80,000 epinephrine | No response to the maximum stimulation (reading of 80) with the pulp tester |
| 25 patients received IANB with periodontal ligament infiltration | ||||||||
| 25 patients received IANB with IO | ||||||||
| 12 | Aggarwal, 2014 [29] | 63 | Mandibular molar | Symptomatic | 31 patients received IANB 2% lignocaine with 1:80 000 epinephrine | 32 patients received IANB 2% lignocaine with 1:200 000 epinephrine | Lignocaine | Pulp access and canal instrumentation into the apical third with no or mild pain |
| 13 | Shadmehr, 2016 [30] | 100 | Mandibular molar | Symptomatic | 50 received 2% lignocaine with clonidine IANB | 50 received 2% lignocaine with epinephrine 1:80 000 IANB | 2% lignocaine | Ability to penetrate dentine, enter the pulp and advance instruments into the coronal part of the canal pulp without pain (VAS score of zero) or mild pain |
| 14 | Stanley, 2012 [31] | 100 | Mandibular molar or premolar | Symptomatic | 50 patients received nitrous oxide/oxygen 6 L/min flow rate of 100% oxygen and IANB | 50 patients received room air/oxygen and IANB | 3.6 ml of 2% lidocaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 15 | Jalali, 2015 [32] | 40 | Mandibular molar | Symptomatic | 20 patients received acupuncture and IANB | 20 patients received IANB only | 2% lignocaine with 1:80 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 16 | Shetty, 2015 [33] | 100 | Mandibular premolar or molar | Symptomatic | 50 patients received 1 mL magnesium sulfate USP 50% and IANB | 50 patients received 1 mL distilled water (placebo) and IANB | 2% lignocaine with 1/80000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 17 | Kreimer, 2012 [34] | 106 | Mandibular molar or premolar | Symptomatic | 56 patients received 5 mL, 63.6 mg of lignocaine with 31.8 mg epinephrine plus 1.82 mL of 0.5 mol/L mannitol or 3-mL containing 76.4 mg of lignocaine with 36 mg epinephrine plus 1.1 mL of 0.5 mol/L mannitol | 50 patients received the same without mannitol | Lignocaine with epinephrine | No pain or weak/mild pain during access and instrumentation,using VAS scale |
| 18 | Schellenberg, 2015 [35] | 100 | Mandibular molar or premolar | Symptomatic | 50 patients received IANB buffered with 0.18 mEq/mL sodium bicarbonate | 50 patients received IANB | 4% lignocaine with 1:100 000 | No pain or weak/mild pain during access and instrumentation using VAS scale |
| 19 | Saatchi, 2016 [36] | 100 | Mandibular first molar | Symptomatic | 50 patients received standard IANB and BI with sodium bicarbonate | 50 patients received IANB | 2% lignocaine with 1:80 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 20 | Saatchi, 2015 [37] | 80 | Mandibular posterior tooth | Symptomatic | 40 patients received 0.18 mL 8.4% sodium bicarbonate (8.4% weight/volume, 50 mEq/50 mL buffered IANB | 40 patients received 0.18 mL of sterile distilled water with IANB | 2% lidocaine with 1:80 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 21 | Dou L, 2013 [38] | 80 | Mandibular molar | Symptomatic | 40 patients received IANB and BI of 0.9 mL of 4% articaine with 1:100 000 epinephrine | 40 patients received IANB and BI and LI of 0.9 mL of 4% articaine with 1:100 000 epinephrine | 2% lignocaine containing 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 22 | Shahi, 2013 [39] | 165 | Mandibular molar | Mentioned as asymptomatic but included patients with prolonged response to cold test. Hence considered symptomatic | 55 patients received 0.5 mg dexamethasone and 55 patients received 400 mg ibuprofen and IANB and BI | 55 patients received placebo of lactose powder and IANB and BI | 2% lignocaine containing 1:80000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 23 | Shantiaee, 2016 [40] | 69 | Mandibular first molar | Symptomatic | 23 patients received 7.5 mg of meloxicam; 23 patients received 600 mg of ibuprofen and IANB | 23 patients received placebo and IANB | 2% lignocaine and 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS |
| 24 | Aggarwal, 2010 [41] | 69 | Mandibular molar | Symptomatic | 22 patients received 300 mg of ibuprofen, 23 patients received 10 mg of ketorolac and IANB | 24 patients received placebo starch capsules and IANB | 1.8 mL of 2% lignocaine with 1:200 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 25 | Jena, 2013 [42] | 100 | Mandibular posterior teeth | Symptomatic | 20 patients received ibuprofen (600 mg), 20 patients ketorolac (10 mg), 20 patients combination of etodolac with paracetamol (400 mg + 500 mg)and 20 patients combination of aceclofenac with paracetamol (100 mg + 500 mg) and IANB | 20 patients were administered placebo with sugar coated pills and IANB | IANB 2% lignocaine with 1:200 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 26 | Parirokh, 2010 [43] | 150 | Mandibular first and second molar | Symptomatic | 50 patients received 600 mg ibuprofen and 60 patients received 75 mg indomethacin And IANB | 50 patients received placebo of lactose powder and IANB | 2% lignocaine with 1/80000 IANB | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 27 | Simpson, 2011 [44] | 100 | Mandibular molar or premolar | Symptomatic | 50 patients received either 800 mg ibuprofen or 1000 mg acetaminophen and IANB and BI | 50 patients received Placebo, IANB and BI | 2% lignocaine with 1:100 000 | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 28 | Fullmer, 2014 [45] | 100 | Mandibular molar or premolar | Symptomatic | 50 patients received 1000 mg acetaminophen plus 10 mg hydrocodone and IANB | 50 patients received placebo an IANB | 2% lignocaine with 1:100 000 | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 29 | Ianiro, 2009 [46] | 40 | Mandibular molar | Symptomatic | 14 patients received 1,000 mg of acetaminophen only, 13 patientsreceived a combination of 1,000 mg of acetaminophen and 600 mg of ibuprofen and IANB | 13 patients received placebo and IANB | 2% lignocaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 30 | Lindemann, 2008 [47] | 58 | Mandibular molar or premolar | Symptomatic | 30 patients received sublingual triazolam 0.25 mg | 28 patients received Placebo | 2% lignocaine with 1:100 000 epinephrine IANB | No pain or weak/mild pain during access and instrumentation using VAS scale |
| 31 | Bigby, 2007 [48] | 50 | Mandibular posterior teeth | Symptomatic | 25 patients received 36 mg meperidine and IANB | 25 patients received IANB | 36 mg of lignocaine with 18 g of epinephrine | No pain or weak/mild pain during access and instrumentation using VAS scale |
| 32 | Akhlagi, 2016 [49] | 40 | Mandibular molar | Symptomatic | 20 received IANB and BI of 0.9 mL articaine. After 5 minutes, 20 patients received supplemental BI of 30 mg/mL ketorolac tromethamine | 20 received the same and BI with normal saline | 4% articaine 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 33 | Yadav, 2015 [50] | 150 | Mandibular first and/or second molar | Symptomatic | 75 patients received standard IANB using 1.8 mL 4% articaine with 1:100 000 epinephrine | 75 patients received standard IANB using 2% lignocaine with 1:80,000 epinephrine | Lignocaine and articaine | no pain or weak/mild pain during access and instrumentation using VAS scale |
| 34 | Saha, 2016 [51] | 126 | Mandibular posterior teeth | Symptomatic | Oral 10 mg ketorolac or 50 mg diclofenac, 84 patients received standard IANB | Oral placebo 42 patients received standard IANB injections | 2% lignocaine containing 1:200 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 35 | Khademi, 2012 [52] | 60 | Mandibular molar | Symptomatic | 30 patients 0.5 mg of alprazolam and IANB | 30 patients received placebo and IANB | 2% lignocaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 36 | Pedro-Munoz, 2016 [53] | 42 | Mandibular molar | Symptomatic | 21 received submucosal 50 mg tramadol and IANB | 21 received placebo and IANB | 4% articaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 37 | Rodrıguez Wong, 2016 [54] | 56 | Mandibular molar | Symptomatic | 28 patients received IANB with tramadol 50 mg | 28 patients received IANB | mepivacaine 2% 1 : 100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 38 | Prasanna, 2011 [55] | 114 | Mandibular molar | Symptomatic | 38 patients received Oral diclofenac and 38 received lornoxicam and IANB | 38 patients received placebo and IANB | 2% lignocaine epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 39 | Sood, 2014 [56] | 100 | Mandibular molar | Symptomatic | 50 patients received 4% Articaine with 1:100 000 epinephrine | 50 patients received 2% lignocaine with 1:80,000 epinephrine | Articaine and lignocaine IANB | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 40 | Tortamano,2009 [57] | 40 | Mandibular molar | Symptomatic | 20 patients received IANB of 4% articaine with 1:100 000 epinephrine | 20 patients received IANB of 2% lignocaine with 1:100 000 epinephrine | Articaine and lignocaine IANB | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 41 | Claffey, 2004 [58] | 72 | Mandibular molar or premolar | Symptomatic | 37 patients received 4% articaine with 1:100 000 epinephrine IANB | 35 patients received 2% lignocaine with 1:100 000 epinephrine IANB | Articaine and lignocaine IANB | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 42 | Allegretti, 2016 [59] | 66 | Mandibular posterior teeth | Symptomatic | 22 patients each received IANB of 4% or 2% mepivacaine with 1:100 000 epinephrine | 22 patients received IANB 2% lignocaine with 1:100 000 epinephrine | Articaine, lignocaine or mepivacaine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 43 | Ahmad, 2014 [60] | 45 | Mandibular posterior teeth | Symptomatic | 15 patients received 2% lignocaine with 1:80,000 epinephrine | 15 patients received 2% lignocaine with 1:200000 epinephrine | Articaine or lignocaine IANB on pain, supplementary BI with same | absence of pain after the administration of BI |
| 15 patients received 4% Articaine with 1:100000 epinephrine | ||||||||
| 44 | Poorni, 2011 [61] | 156 | Mandibular molar | Symptomatic | 52 patients received IANB with 4% articaine with 1:100 000 epinephrine | 52 patients received IANB with 2% lignocaine with 1:100 000epinephrine | Articaine and lignocaine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 52 patients received additional BI | ||||||||
| 45 | Sherman, 2008 [62] | 40 | Maxillary molar | Symptomatic | 20 patients received 1.7 mL of articaine by a Gow–Gates or maxillary infiltration | 20 patients received 1.8 mL of lignocaine by Gow–Gates block or maxillary infiltration | Articaine and lignocaine | No pain or weak/mild pain during access and instrumentation,using VAS scale |
| 46 | Rogers, 2014 [63] | 100 | Mandibular molar | Symptomatic | 74 patients received IANB and supplemental BI using articaine or lignocaine | 26 patients received IANB | 4% articaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 47 | Monteiro, 2014 [64] | 50 | Mandibular molar | Symptomatic | 30 patients received IANB and BI of 4% articaine with 1 : 100 000 | 20 patients received IANB. | 2% lignocaine with 1:100 000 epinephrine | Ability to access and instrument the tooth with no pain or no more than mild pain |
| 48 | Bigby, 2006 [65] | 49 | Mandibular posterior teeth | Symptomatic | 39 patients received IANB and long buccal injections | 10 patients received IANB | 4% articaine with 1:100 000 epinephrine | No or mild pain upon endodontic access or initial Instrumentation |
| 49 | Fan, 2009 [66] | 60 | Mandibular first molar | Symptomatic | 30 IANB and additional BI | 30 IANB and additional PDL injections | 4% articaine/HCl with epinephrine 1:100 000 | No pain or weak/mild pain during access and instrumentation using VAS scale |
| 50 | Visconti, 2016 [67] | 43 | Mandibular molar | Symptomatic | 21 patients received IANB 2% mepivacaine | 22 patients received IANB 2% lignocaine | Mepivacaine and lignocaine | Accessed the pulp chamber without the patient reporting pain |
| 51 | Sampaio, 2012 [68] | 70 | Mandibular molar | Symptomatic | 35 patients received 0.5% bupivacaine with 1:200 000 epinephrine IANB | 35 patients received 2% lignocaine with 1:100 000 epinephrine IANB | Bupivacaine and lignocaine | Accessed the pulp chamber without the patient reporting pain |
| 52 | Singla, 2015 [69] | 147 | Mandibular first or second molar | Symptomatic | 73 patients received standard IANB and 1.8 ML BI | 74 patients received standard IANB and 3.6 mL BI | 4% articaine with 1:100 000 epinephrine | No pain or weak/mild pain during access and instrumentation, using VAS scale |
| 53 | Abazarpoor,201 5 [70] | 80 | Mandibular first molar | Symptomatic | 40 patients received 3.6 mL articaine IANB | 40 patients received 1.8 mL articaine IANB | 4% articaine with 1:100 000 epinephrine | Ability to undertake pulp access and canal instrumentation into the apical third with no or mild pain |
| Studies in the maxilla | ||||||||
| 1 | Aggarwal, 2011 [71] | 61 | Maxillary first molar | Symptomatic | 28 patients received PSA | 33 patients received BI | 2% lignocaine with 1:200 000 epinephrine | No pain or weak/mild pain during access and instrumentation using VAS |
| 2 | Mehrvarzfar, 2014 [72] | 61 | Maxillary molars | Symptomatic | 31 patients received local infiltration and 0.8 mL of fentanyl (40 μg). | 30 patients received local infiltration and sterile normal saline solution | 2% lignocaine, containing 1:80000 epinephrine | 2 consecutive negative reading of EPT (maximum 80) |
| 3 | Elsharrawy, 2007 [73] | 40 | Maxillary molars | Symptomatic | 20 patients received infiltration and intraligamental 0.4 mL fentanyl 0.05 mg/ml | 20 patients received infiltration and intraligamental mepivacaine | 1.8 mL of 2% mepivacaine with 1:200 000 epinephrine | Success was recorded as “none” or “mild” pain. |
| 4 | Atasoy, 2014 [74] | 50 | Maxillary first molar | Symptomatic | 25 patients received 4% articaine HCl + 1:100 000 epinephrine infiltration | 20 patients received 4% articaine HCl + 1:100 000 Epinephrine bitartrate infiltration | Articaine | Successful pulpal anesthesia. |
| 5 | Srinivasan, 2009 [75] | 40 | Maxillary posterior tooth | Symptomatic | 20 patients received 4% articaine with epinephrine 1:100 000 infiltration | 20 patients received 2% lignocaine with epinephrine 1:100 000 infiltration | Articaine and lignocaine | No pain or weak/mild pain during access and instrumentation using VAS scale |
| 6 | Hosseini, 2016 [76] | 40 | Maxillary first molar | Symptomatic | 20 patients received BI of 1.8 mL of 4% articaine with 1:100000 epinephrine | 20patients received BI of 1.8 mL 2% lignocaine with 1:80000 epinephrine | Articaine | Absence of pain or mild discomfort |
| 7 | Ramachandran, 2012 [77] | 100 | Maxillary first molar | Symptomatic | Premedication with 1000 mg of paracetamol or 800 mg of ibuprofen, 100 mg aceclofenac and infiltration | Premedication with placebo and infiltration | 2% lignocaine with epinephrine 1:200 000 | Absence of pain during access preparation and root canal instrumentation |
| 8 | Kanna 2012 [78] | 50 | Maxillary teeth | Symptomatic | 2.0 mL 4% articaine with 1:100 000 epinephrine BI | 2% lidocaine with 1:80,000 epinephrine BI | Articaine and lignocaine | No response was obtained to the maximum stimulation (80 reading) of the pulp tester |
| Study of both maxillary and mandibular teeth | ||||||||
| 1 | Nusstein, 1998 [79] | 51 | Mandibular or maxillary molar or premolar | Symptomatic | 26 patients received IANB or BI in addition to IO | 25 received conventional IANB or BI | 2% lignocaine with 1:100 000 epinephrine. | No pain or weak/mild pain during access and instrumentation using VAS scale |
![]()
2. Direct comparison: Pooled results for mandibular anesthetic techniques
The pooled estimates (odds ratio) for comparison of different anesthetic techniques with 2% lignocaine IANB in the mandible are presented in Figure 3. The estimates are arranged in a forest plot from the top to bottom in decreasing order of outcome success. Increased likelihood of success was observed with
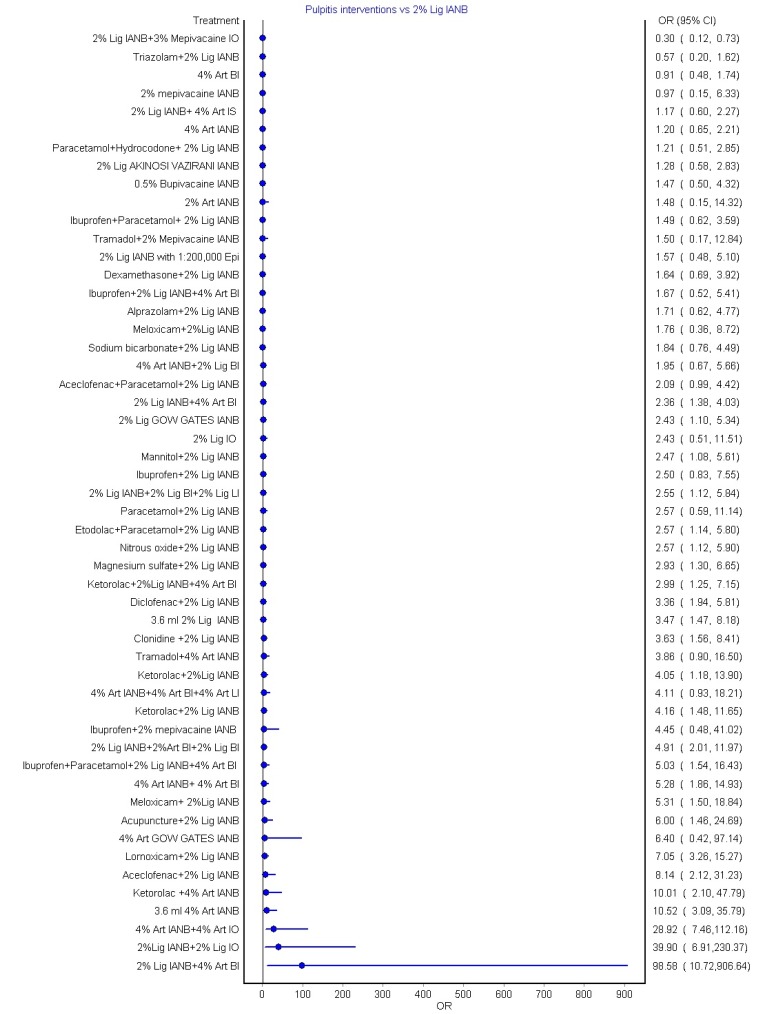
Other significant interventions that performed better than 2% lignocaine IANB alone include: 2% lignocaine Gow–Gates IANB (2.43 [1.10, 5.34]); mannitol + 2% lignocaine IANB (2.47 [1.08, 5.61]); 2% lignocaine IANB + BI + lingual infiltration (LI) (2.55 [1.12, 5.84]); etodolac + paracetamol before 2% lignocaine IANB (2.57 [1.14, 5.80]); nitrous oxide with 2% lignocaine IANB (2.57 [1.12, 5.90]). Other interventions (Fig. 3) also showed significant pooled estimates; however, they were considered less precise due to their wider confidence intervals.
3. Indirect comparison: Pooled results for mandibular anesthetic techniques
The indirect comparison pooled estimates were derived using common comparator principle and are shown in Figure 4. The chances of increased success of anesthesia were observed with:
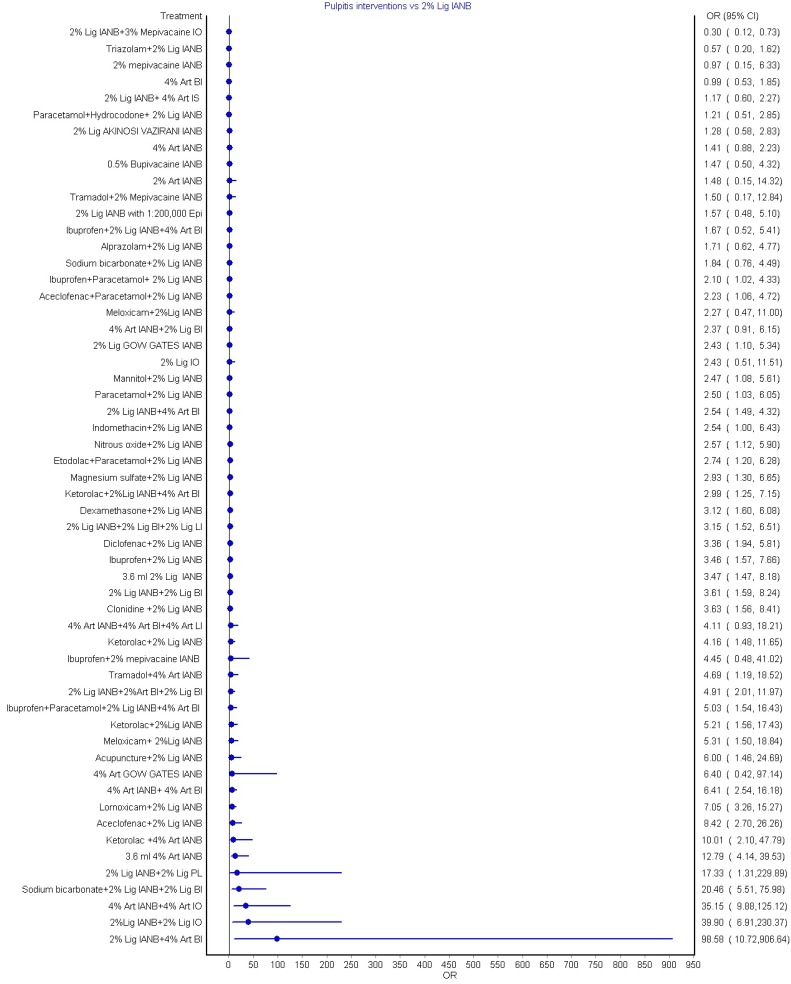
Other interventions that performed better than 2% lignocaine IANBalone were 2% lignocaine Gow–Gates IANB (2.43 [1.10, 5.34]); mannitol with 2% lignocaine IANB (2.47 [1.08, 5.61]); 4% articaine BI with 2% lignocaine IANB (2.54 [1.49, 4.32]); nitrous oxide with CIANB (2.57 [1.12, 5.9]). The estimates of other interventions are presented in Figure 4. Although significant, they were considered less precise given their wider confidence intervals. Mild inconsistencies were observed for the pooled estimates between direct and indirect comparisons, with H values ranging between 1 and 1.5. Similarly, mild-to-moderate heterogeneity was observed.
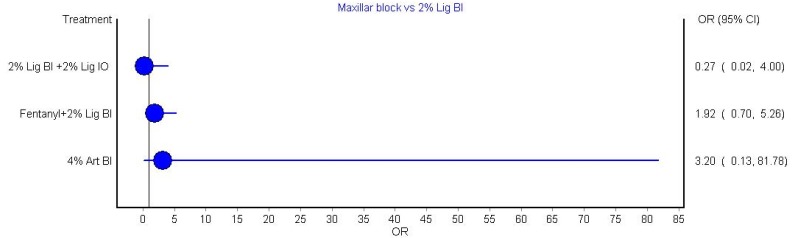
4. Indirect comparison: Pooled results for maxillary anesthetic techniques
The indirect pooled estimates for the following interventions in comparison with 2% lignocaine BI in the maxilla is shown in Figure 5: adjuvant intra-osseous 2% lignocaine; and 4% articaine BI and adjuvant fentanyl. No significant difference in the success rate of maxillary anesthesia was observed with any of the above-mentioned approaches. Direct comparison was not attempted because of the small number of available studies. Mild to moderate heterogeneity was observed between direct and indirect comparisons using H-statistics and I2 tests. This indicated that the results obtained were dependable.
5. Grading the evidence
Grading of the evidence for key comparisons was carried out based on the assessment of indirectness, inconsistency, publication bias, and imprecision of the estimates. Very low quality of evidence was observed due to serious limitations in the precision of the estimates and because publication bias could not be assessed (Table 2).
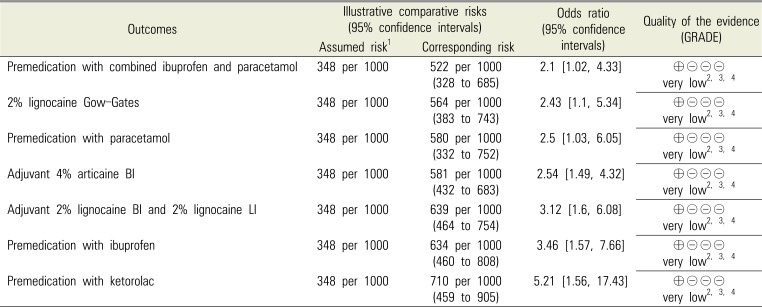
Table 2
Grading the quality of evidence for key comparisons using 2% lignocaine IANB for the success of anesthesia
1—Assumed risk was the median control group risk across the studies
2—Downgraded one level as publication bias could not be assessed
3—Downgraded one level for imprecision of the estimates, as evident by the wider confidence intervals
4—Downgraded one level for low sample size
Very low quality: Marked uncertain about the estimate.
![]()
Go to :
DISCUSSION
This NMA attempted to identify the best agent and technique for successful local anesthesia in the maxilla and mandible in adult patients with symptomatic irreversible pulpitis undergoing endodontic treatment. The results indicated that premedication with ibuprofen + paracetamol, or aceclofenac + paracetamol before IANB, or 2% lignocaine IANB + 4% articaine BI, produced the most successful anesthesia in the mandible. No significant difference in the success rate of maxillary anesthesia was noted with the approaches tested due to the low number of available studies.
Reports indicate that the most commonly used, conventional lignocaine IANB failed at a rate of 15–50% [13]. The most common cause of failure was poor injection technique, followed by technical errors and anatomical variability, infection and inflammation, pathological processes, and psychological causes, such as fear, apprehension, or anxiety [113].
Although Gow–Gates and Akinosi–Vazirani techniques showed varied anesthetic success compared with IANB in previous studies [808182], results from the present meta-analysis showed that the Gow–Gates approach performed better than the Akinosi technique or conventional IANB. This variability can be attributed to the experience of the dentist administering the nerve block. Most dentists do not adopt this technique due to inadequate training and experience [81]. Overall, the Gow–Gates technique has been proven to have a higher likelihood of success in patients with varied anatomy, when performed by a skilled dentist. A recent study also reported increased success with a combination of the Gow–Gates technique and conventional IANB [83]. Results from previous randomized trials did not indicate significant differences in pain during injection using these techniques [83]. Other reported advantages of the adjuvant techniques, such as the Gow–Gates and Akinosi techniques, include a lower incidence of positive aspiration and decreased problems related to accessory innervation [80818283].
The use of supplemental buccal, lingual, intraosseous, and intraligamentary infiltrations as a means to deal with collateral nerve supply have also been tested in various randomized controlled trials, and results from pooled estimates indicate higher success [84]. Pooled results from the present review also indicate that supplemental infiltration produced better success rates. Specifically, the most successful anesthesia was produced with supplemental 4% articaine BI, followed by 2% lignocaine BI and LI in the mandible. Infiltration alone has been recommended in the anterior mandibular region because of the particular disadvantages of bilateral administration of blocks [84858687]. There is a paucity of data from randomized controlled trials on the use of infiltration alone in the anterior mandible. Most dentists consider supplemental infiltration as a means to manage the collateral nerve supply, as well as in cases of block failure, according to the studies included in the present review [212232].
The commonly tested agents in the studies were articaine and lignocaine. Other agents, such as bupivacaine and mepivacaine, were tested in very few trials. Results from previous studies did not show significant differences between articaine and lignocaine IANB alone [45], although supplemental articaine infiltration was shown to produce significant success [45]. Similar results were obtained in the present NMA, probably because most trials concentrated on articaine and lignocaine only. The safety profile of these drugs was reported to be similar, although articaine caused greater injection pain scores [45]. Other local anesthetic agents need to be studied in detail in randomized controlled trials to warrant any conclusion.
A meta-analysis on the success of IANB for teeth with irreversible pulpitis concluded that premedication with NSAIDs before IANB increased the efficacy of anesthesia [7]. Results from the present NMA specifically indicate that the combination of ibuprofen + paracetamol and aceclofenac + paracetamol premedication before IANB produced the most successful anesthesia, as compared to the injection techniques alone. Other drugs that were used alone or in combination were piroxicam, naproxen, diclofenac, steroids, and benzodiazepines, prescribed 1 hour before the block. However, premedication with drugs has been tested mainly before IANB, and not in combination with any other techniques. The effect of premedication using oral drugs as a supplemental technique for pain control in irreversible pulpitis requires further investigation.
Most of the studies in the review used infiltration with or without an intraosseous injection technique. No conclusive evidence is available from the present review, mainly due to the limited number of available studies. Individual study results indicated that dentists preferred infiltration techniques in the maxilla, due to the cancellous nature of the bone, covered by a thin cortical plate, which allows easier penetration of the anesthetic solution. Furthermore, maxillary blocks were technique-sensitive [86]. This is probably the reason for fewer available clinical trials on block anesthesia in the maxilla [86]. There is a need for future studies on different anesthetic agents and techniques to allow a firm conclusion to be drawn.
The study was limited by the small sample sizes in the included studies for evaluation of each of the interventions tested, which is evident from the wider confidence intervals. Increased sample sizes in the individual trials would likely narrow the confidence interval and provide a more compelling conclusion. This NMA suggested that future clinical trials should make a strong effort to increase sample size. Given the quality of evidence and the limitations of the individual studies, the pooled data obtained via NMA does not provide confident, conclusive guidance for clinicians. Although the literature indicates that the efficacy of anesthesia differs between symptomatic and asymptomatic pulpitis [87], this was not tested in the present review. All included trials addressed symptomatic pulpitis cases only. Publication bias could not be assessed, and other variables, such as psychological profile and characteristics of healthcare facilities, which may impact the outcome measures, were not considered.
In conclusion, the use of premedication with ibuprofen and paracetamol, or aceclofenac and paracetamol, prior to conventional 2% lignocaine IANB, or supplemental 4% articaine BI may produce the most successful anesthesia for mandibular teeth with irreversible pulpitis. This meta-analysis could not identify the most favorable technique in the maxilla, because of limited number of available studies. NMA is a powerful tool that can help to identify the best possible technique by using mixed treatment comparisons in cases of limited clinical trials. This NMA suggested that IANB with lignocaine alone may be unlikely to produce effective anesthesia in symptomatic irreversible pulpitis in the mandible, and that supplemental injections or premedication may improve the anesthetic success. Future randomized control trials should focus on the overall quality of the study, with larger sample sizes, which will more likely produce definitive conclusions.
Go to :
 XML Download
XML Download