

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Over the past decades, scientific reports have consistently reported a significant increase in dental caries worldwide amongst adults and children [1]. Early childhood caries (ECC) remains one of the most prevalent chronic and transmissible diseases in children globally [2]. According to the first ever General Surgeon's report on Oral Health in America, ECC is five and seven times more frequent than asthma and hay fever, respectively [3]. Statistics from 2010 revealed that untreated caries in primary teeth was the 10th most prevalent condition, affecting 621 million children worldwide [4].
ECC continues to be, a major health concern and serious challenge despite the wide range of preventive measures and treatments available. This is mainly due to its multi factorial etiologies and their link with socioeconomical and educational parameters.
1. An overview of early childhood caries
The AAPD defines ECC as the presence of one or more decayed (non cavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces in any primary tooth in a child aged 71 months or younger. Any sign of smooth surface caries in children younger than 3 years of age is indicative of severe ECC [5].
ECC leads to pain, possible infection, destruction of dental surfaces, deterioration of life quality of children (difficulties in speaking, eating, sleeping, delayed physical growth), and school and social disruption for kids and their caregivers if left untreated [67].
The most commonly used preventive measures in managing ECC, in addition to awareness and educational programs, remains the topical application of antimicrobial agents (such as fluoride gels, fluoride varnishes, sealants, chlorhexidine, xylitol, povidone iodine, and silver compounds) [8].
Extensively cavitated ECC lesions pose a growing challenge in terms of treatment. Where possible, minimally invasive techniques are advantageous [9]. There is no consensus as to the best conventional restorative technique despite advancements in dental materials and techniques [8]. Following pulp therapy, it is generally advised to seal teeth with a stainless steel crown.
Despite the wide array of treatments available, one major aspect of child management remains their acceptance of the proposed procedures in the dental chair without anxiety or perceiving dental visits as a threat. Children exhibit different attitudes and temperaments, which are influenced by their differences in physical, emotional, and social development. To provide the best possible painless and stress-free care under a conventional dental setting, behavioral management approaches have shifted in the second half of the 20th century to an increased emphasis on communication and empathy [10]. Dental practitioners have a range of non-pharmacological techniques to choose from that are dependent on their clinical training, experience, communication skills, patient specificities, and parents' involvement (Table 1). Under certain circumstances, the health provider is faced with challenges in the dental chair that may lead to ineffective strategies to combat the disease. Therefore, there has been a shift to pharmacological management to provide a safer environment for children and parents. At the end of the sedation continuum is the use of general anesthesia (GA) [11]. This type of individualized dental treatment has been used more often in the last decades as a means to provide high quality preventive or restorative treatment in one appointment.
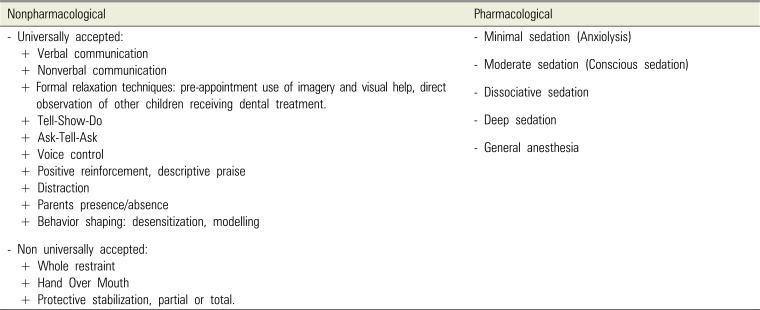
Table 1
Classification of behavioral management techniques in pediatric dentistry
![]()
2. General anesthesia in the management of ECC
2.1 Definition and indications of GA
GA is a medical procedure defined as a controlled state of drug induced loss of consciousness during which patients cannot be aroused, even by painful stimuli, and lose their protective reflexes. Independent ventilatory function is frequently inadequate and cardiovascular function may be impaired [1213].
The most recent UK national clinical guidelines in pediatric dentistry, issued by the Royal College of Surgeons in 2008, state only two indications for GA, which are not absolute [14]:
This might seem ambiguous; however, this rationale states that the use of GA should provide a safe, painless, anxiety-free, and humane environment for effective dental care. The dental provider and child's care giver should consider the following points before a decision is made [11]:
• The degree of non-cooperation of the child due to a lack of psychological or emotional maturity and/or mental, physical, or medical disability.
• The degree of anxiety exhibited, which can lead to an uncommunicative child.
• The presence of complex medical conditions.
• The very young age of the patient, which might contra-indicate the use of other sedation strategies in the anesthesia continuum.
• The failure of other behavioral guidance modalities.
• The duration of the intervention and need for immediate pain relief or significant surgical procedures.
• The presence of allergies that absolutely contraindicate local anesthesia, the presence of an acute infection, or anatomic variations that render local anesthesia ineffective.
GA should not be considered for healthy cooperative children, very young children with minimal dental needs, or in the presence of any general condition with contraindications [11].
2.2 Mortality and morbidity risks of pediatric GA
GA is not a benign procedure nor is it without an element of risk. There is no consensus in the literature regarding the definition of anesthesia related mortality due to subjective interpretations; however, the survival rates of children and infants under GA have significantly improved. This improvement can be credited to the use of antibiotics, a better understanding of physiopathology, and advancements in anesthetic drugs and support equipment [15].
Previous studies have sought to quantify pediatric anesthesia-related mortality risks. Most reported fatalities occur in neonates and infants and this risk does not increase in teenagers and young adults. Limiting the mortality risk in dentistry related cases reduces the risk further because these cases feature less complicated interventions at a more advanced age [16].
Few publications have exclusively focused on risks associated to dental patients [17]. Keenan in 1994 [18] conducted an earlier reviews specifically examining GA in dental cases. He determined a mortality rate 1 per 162,000 cases over a five-year period. Interestingly, a ten-year review of medical records from regional hospitals from the American Hospital Association reported no deaths in 22,615 cases involving dental care under GA [16].
Morbidity risks in pediatric anesthesia can be divided into minor vs. major, with major morbidity being rare and both occurring mainly in the first year of life and severe associated co-morbidities [19]. Post-operative morbidity in dental settings is common; however, its severity is typically mild and limited to the first day. The most common complaints are an inability to eat, sleepiness, and pain. Less common are drowsiness, dental bleeding, vomiting, sore throat, psychological changes, nausea, coughing, and fever [2021].
2.3 The increasing use of GA in pediatric dentistry
The American Dental Association recognizes dental treatment under GA as a viable option to provide optimum care to children because of its low rates of post-operative complications, provided the indications for use are met [11]. Public acceptance of GA has also evolved in recent years, with an increase in preference for its use in parents when compared with negative behavioral management [22]. Therefore, the demand for GA in Western countries has been growing. In 2012, a North American online survey of the directors of dentist anesthesiologist and pediatric dentistry residencies revealed an 88% increase in requests for dentist anesthesiologist services by pediatric dentists in the past ten years [23]. Between 2004 and 2014 in New Zealand, a 65% increase of children receiving dental treatment under GA [24]. In 2015-16 in England, approximately 43,700 children aged 16 years and under were admitted to hospital with a primary diagnosis of dental caries [25]. In addition, the use of dental-related GA has increased in many other European countries, Asia, and the Middle East [26].
Does the use of general anesthesia for ECC management lead to better results?
ECC treatment approaches under GA fall under two main categories: extractions only, or an approach that combines all treatments, which may be restorative, preventive, or exodontia. The choice is influenced by many factors, including the restorability of the teeth, caries risk for the child, ability of the child to maintain a satisfactory level of hygiene, parents' wishes and socioeconomical status, the possibility of a follow up, and the resources available. For example, GA is used mostly for extractions in the UK [25].
GA usually allows treatment to be performed under optimal conditions; therefore, the expectations for an ideal outcome, especially in restorative treatments, are high. Over the past decade, multiple studies have been published that highlight the success of ECC treatment strategies under GA.
For this review, we conducted a broad search of the PubMed database was conducted from 2009 through 2019 using the index terms “early childhood caries” and “dental general anesthesia”. Only relevant studies published in English were included after a review of their abstracts. Papers were selected if they reported studies restricted to a healthy preschool child population and relevant to dental treatment of ECC under GA and/or the children's subsequent Oral Health Related Quality of Life (OHRQoL) post-GA.
The initial search revealed 94 papers, of which 21 met the inclusion criteria. These studies are compiled in Table 2.
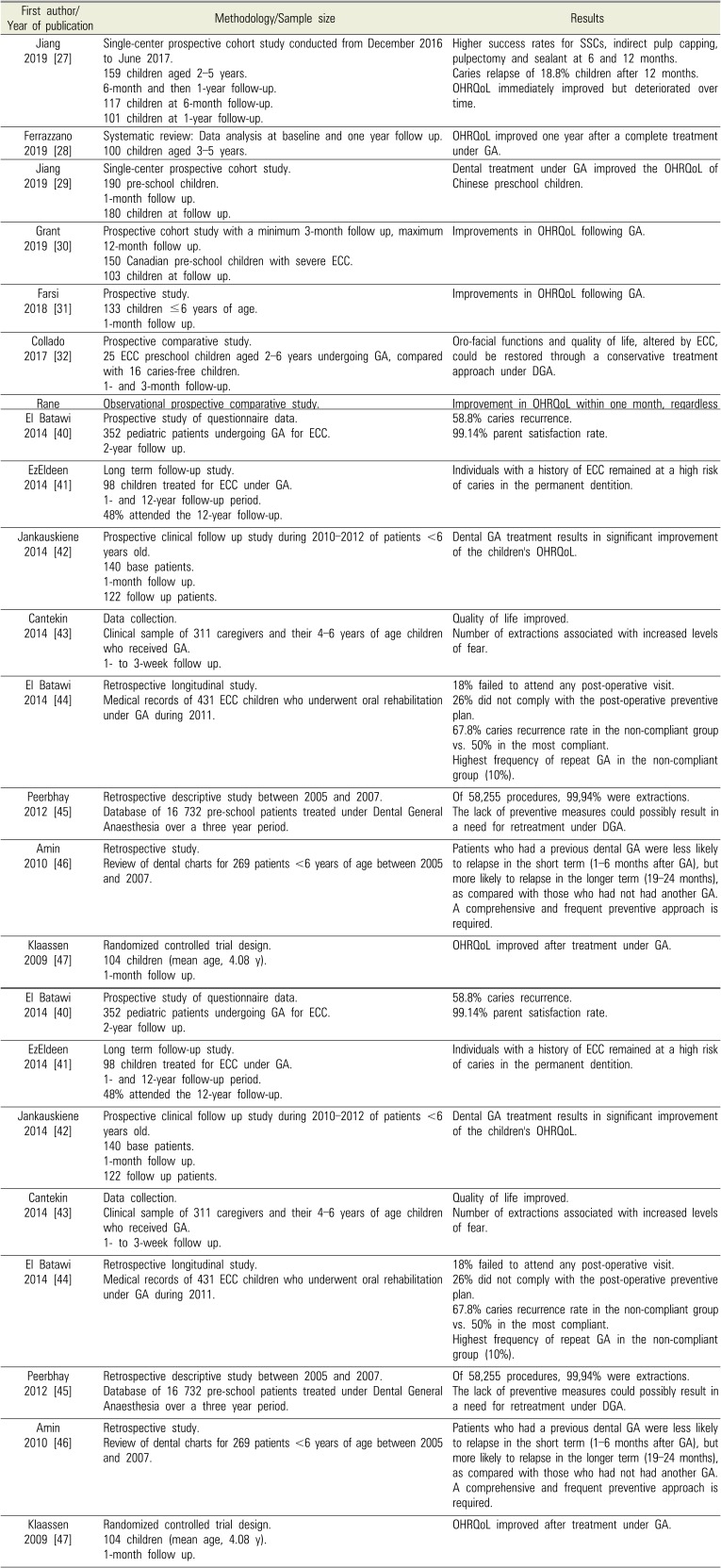
Table 2
ECC dental rehabilitation under GA around the world
| First author/Year of publication | Methodology/Sample size | Results |
|---|---|---|
| Jiang 2019 [27] | Single-center prospective cohort study conducted from December 2016 to June 2017. | Higher success rates for SSCs, indirect pulp capping, pulpectomy and sealant at 6 and 12 months. |
| 159 children aged 2–5 years. | Caries relapse of 18.8% children after 12 months. | |
| 6-month and then 1-year follow-up. | OHRQoL immediately improved but deteriorated over time. | |
| 117 children at 6-month follow-up. | ||
| 101 children at 1-year follow-up. | ||
| Ferrazzano 2019 [28] | Systematic review: Data analysis at baseline and one year follow up. | OHRQoL improved one year after a complete treatment under GA. |
| 100 children aged 3–5 years. | ||
| Jiang 2019 [29] | Single-center prospective cohort study. | Dental treatment under GA improved the OHRQoL of Chinese preschool children. |
| 190 pre-school children. | ||
| 1-month follow up. | ||
| 180 children at follow up. | ||
| Grant 2019 [30] | Prospective cohort study with a minimum 3-month follow up, maximum 12-month follow up. | Improvements in OHRQoL following GA. |
| 150 Canadian pre-school children with severe ECC. | ||
| 103 children at follow up. | ||
| Farsi 2018 [31] | Prospective study. | Improvements in OHRQoL following GA. |
| 133 children ≤6 years of age. | ||
| 1-month follow up. | ||
| Collado 2017 [32] | Prospective comparative study. | Oro-facial functions and quality of life, altered by ECC, could be restored through a conservative treatment approach under DGA. |
| 25 ECC preschool children aged 2–6 years undergoing GA, compared with 16 caries-free children. | ||
| 1- and 3-month follow-up. | ||
| Rane 2017 [33] | Observational prospective comparative study. | Improvement in OHRQoL within one month, regardless of GA or LA. |
| 50 parents of children aged 2–6 years old with ECC divided into 2 groups: 25 parents of children treated under GA, 25 parents of children treated under LA. | ||
| 1-month follow up. | ||
| Chao 2017 [34] | Retrospective study of data collection. | Children OHRQoL improved significantly. |
| 659 pediatric patients treated for ECC under GA from 2013–2014. One month follow up. | 82.8% of families reported a high degree of satisfaction. | |
| Amin 2016 [35] | Retrospective cohort study. | Amalgam restorations and SSCs showed longer survival rates than composite restorations. |
| 818 ECC children, ≤72 months at the time of treatment. | Higher survival rate of pulpectomies compared to indirect pulp capping and pulpotomies. | |
| 3-year follow up. | 32.9% required retreatment over the 3 year follow up. | |
| Wong 2016 [36] | Data collection. | Emergency dental extraction under GA significantly improved the OHRQoL of preschool children who presented to the emergency department with the consequences of untreated dental caries. |
| 221 preschool children who underwent emergency extractions under GA over a 12-month period. | ||
| 2-week follow up. | ||
| 126 children at follow up. | ||
| De Souza 2016 [37] | Cohort study. | Substantial improvements in parents' ratings of their children's OHRQoL. |
| 126 children at follow up. | ||
| 78 parents of 2–6 year old children with ECC undergoing GA. | ||
| A minimum of 1-month follow-up. | ||
| 72 parents follow-up. | ||
| Yawary 2016 [38] | Data collection, parents' questionnaire. | OHRQoL of children less than 6 years of age was improved after comprehensive oral rehabilitation under GA, improvement sustained over a three month period. |
| 70 parents of preschool children under age 6 undergoing oral rehabilitation under GA. | ||
| Two weeks and then 3-month follow-up. | ||
| 39 parents at follow up. | ||
| Amin 2015 [39] | Single center retrospective cohort study. | Caries relapse rate of 21.6%. |
| 278 children <6 years of age at the time of GA. | ASA-2 children and those with less than full primary dentition during GA were twice as likely to experience caries relapse. | |
| 36-month follow up period over 5 recall visits. | ||
| 45.3% children returned for all recall visits. | ||
| El Batawi 2014 [40] | Prospective study of questionnaire data. | 58.8% caries recurrence. |
| 352 pediatric patients undergoing GA for ECC. | 99.14% parent satisfaction rate. | |
| 2-year follow up. | ||
| EzEldeen 2014 [41] | Long term follow-up study. | Individuals with a history of ECC remained at a high risk of caries in the permanent dentition. |
| 98 children treated for ECC under GA. | ||
| 1- and 12-year follow-up period. | ||
| 48% attended the 12-year follow-up. | ||
| Jankauskiene 2014 [42] | Prospective clinical follow up study during 2010–2012 of patients <6 years old. | Dental GA treatment results in significant improvement of the children's OHRQoL. |
| 140 base patients. | ||
| 1-month follow up. | ||
| 122 follow up patients. | ||
| Cantekin 2014 [43] | Data collection. | Quality of life improved. |
| Clinical sample of 311 caregivers and their 4–6 years of age children who received GA. | Number of extractions associated with increased levels of fear. | |
| 1- to 3-week follow up. | ||
| El Batawi 2014 [44] | Retrospective longitudinal study. | 18% failed to attend any post-operative visit. |
| Medical records of 431 ECC children who underwent oral rehabilitation under GA during 2011. | 26% did not comply with the post-operative preventive plan. | |
| 67.8% caries recurrence rate in the non-compliant group vs. 50% in the most compliant. | ||
| Highest frequency of repeat GA in the non-compliant group (10%). | ||
| Peerbhay 2012 [45] | Retrospective descriptive study between 2005 and 2007. | Of 58,255 procedures, 99,94% were extractions. |
| Database of 16 732 pre-school patients treated under Dental General Anaesthesia over a three year period. | The lack of preventive measures could possibly result in a need for retreatment under DGA. | |
| Amin 2010 [46] | Retrospective study. | Patients who had a previous dental GA were less likely to relapse in the short term (1–6 months after GA), but more likely to relapse in the longer term (19–24 months), as compared with those who had not had another GA. A comprehensive and frequent preventive approach is required. |
| Review of dental charts for 269 patients <6 years of age between 2005 and 2007. | ||
| Klaassen 2009 [47] | Randomized controlled trial design. | OHRQoL improved after treatment under GA. |
| 104 children (mean age, 4.08 y). | ||
| 1-month follow up. |
![]()
Go to : 
RESULTS
1. Impact of ECC rehabilitation under GA on OHRQoL
When evaluating the outcome of a treatment, both the clinical impact and incidence on quality of life should be taken into account. OHRQoL is an emerging multidimensional construct recognized by the World Health Organization as an important segment of the Global Oral Health Program (2003) [48]. OHRQoL assessments are particularly important in survey research to examine trends, highlight population needs, and measure treatment efficacy to improve care through potential policies and protocols. But most importantly, OHRQoL allows a shift from a traditional clinical approach to the integration of the patient as an active participant by taking into account the impact of oral disease and care on their daily emotional, social, and physical experiences [49].
Studies with short-term follow up periods have indicated a significant improvement in the OHRQoL of children. Interestingly, one long-term study highlighted that it has deteriorated over time after an immediate improvement. This indicates that GA is a positive addition to ECC management; however, it is important to discuss the limitations of these measures. A loss of contact with participants post treatment might justify the short follow up periods in most studies; however long term assessment is necessary to judge the sustainability of results because an early follow up might not yet show the full quality of life gains from the treatment. Evaluating patient satisfaction through questionnaires might be affected by response bias or misinformation because most preschool children lack the linguistic and cognitive maturity required to answer the questions. This means that most responses rely on a proxy perspective via parents or caregivers. This might lead to a different perspective depending on family dynamics and personality traits. In addition, high parental satisfaction does not always match the post-operative outcome. Treatment choices (restorative, exodontia, and preventive) might also influence the scores. While these represent a positive overall effect, further studies are required to assess different treatment types and the application of age appropriate scores.
2. Impact of ECC rehabilitation under GA on restorative outcomes and caries relapse
Most recent studies do not report different treatment choices, the restorative failure rate, or the caries relapse rate. These studies rely on parental satisfaction and overall quality of life as outcome measurements. Jang and Shen (2019) and Amin (2016) did report these factors and show similar findings to previous studies.
As early as 1991, O'Sullivan et al. [50] reported that the use of stainless steel crowns (SSCs) in the treatment of ECC under GA yielded better results than conventional restorations with amalgam and composite (3% vs. 29% failure rate). They reported a failure rate of 2% for vital pulpotomies. In line with this, El Eheideb et al. [51] reported that SSCs were more successful (95.5%) when compared with amalgam and composite restorations (50%) and pulpotomies showed a 97.1% success rate. In anterior teeth, strip crowns had a similar success rate when compared with composite resin materials and sealants had an increased average retention rate (68.3%). Further, Tate concluded that SSCs showed the most reliable results and blamed the failure of composite restorations on follow up length [52]. Eidelman et al. [53] compared the quality of restorations performed in young children with ECC under GA to those treated under sedation. They concluded that the frequent use of SSCs in the GA group is motivated by the extensive destruction of teeth and a reduced possibility for the requirement of further retreatment. Similarly, the absence of movement from the child allows for the use of sensitive strip crowns that provide better results in the GA group. Therefore, only 59% of patients under GA required a follow up, which is compared with 74% of patients under sedation.
Nonetheless, ECC is an aggressive and multifactorial disease with a high relapse rate and higher chance of developing caries in permanent dentition [212241]. Therefore, many children with ECC that are treated under GA exhibit high caries relapse rates. Almeida et al. [54] reported a 79% caries recurrence rate in children who underwent ECC treatment under GA; 17% of these patients required a repeat GA intervention within two years. Similar results were revealed by Kakaounaki et al. [55]: 8.9% of 484 children required a re-intervention under GA during a 6-year follow up period. Further, Berkowitz et al. [56] reported that over half the children in their study exhibited new smooth surface caries lesions after 6 months and most parents were unresponsive to later appointments. Similarly, Foster reported that half their patients had new caries within two years and this relapse was more likely when parents failed to attend follow up care [57]. Amin et al. (2010) reported a 22% relapse rate in patients attending a recall appointment within 1 year following surgery compared with a 51% relapse rate in the group attending their first recalls at 13–24 months post-surgery. Correspondingly, an increased relapse rate from 51% in the high attendance patients to 68% in patients with lower attendance rates was reported by El Batawi (2014). The aggressive dental approach of ECC under GA (extractions, pulp therapy, and SSCs) did not decrease caries relapse, which might indicate that this is better explained by a lack of follow up care and persistence of cariogenic habits post rehabilitation [5859].
Therefore, it is clear that GA might be a preferable option in certain cases for dealing with extensive ECC damage in uncooperative children; however, a strict compliance with post-operative plans is crucial to avoid the loss of any positive rehabilitation outcomes. Poor follow up compliance or loss of participants might indicate unreported caries recurrence. This highlights that the caregiver should be the primary recipient of information regarding the importance of follow up care and hygiene. An approach that treats the clinical outcome of caries alone without addressing or correcting the underlying risk factors of ECC will fail. Therefore, the role of the pediatric dentist goes beyond the surgical intervention because they are required to provide appropriate guidance and insist on regular follow up visits. Future research should focus on the tooth-based and patient-related factors of relapse. Procedure focused studies will have clinical significance in determining the preferred protocols for the restorations of specific teeth or surfaces and the success rate of each procedure. Taking into consideration patient related factors is important because it affects equally the choice and success of specific treatments.
Go to :
CONCLUSION
The aim of using GA is to restore optimal oral health in a single visit and prevent any anxiety associated with several dental chair visits for patients with ECC that require extensive dental work. It should be viewed as a behavioral control technique and not a miraculous solve-it-all approach; however, its success relies heavily on subsequent follow up visits. Therefore, the education and motivation of caregivers are vital for the maintenance of good results and prevent any relapse. This includes attending follow up appointments and regularly monitoring and/or modifying dietary plans and hygiene habits.
Go to :
 XML Download
XML Download