

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pelvic fracture urethral injuries (PFUI) in men are challenging clinical problem for urologists. In particular, pelvic bone fractures accompanying urethral injuries after traumatic accident are not easily accessible due to the distorted anatomy [12]. Furthermore, many studies show a high recurrence rate for urethral stenosis after bulbomembranous anastomotic urethroplasty, which makes the treatment of posterior urethral injuries a reconstructive dilemma for urologic surgeons [234]. Even when proper preparation for bulbomembranous anastomotic urethroplasty, such as thorough preoperative evaluation, appropriate surgical planning, and adherence to basic surgical principles, is carried out, many studies still show unfavorable outcomes after bulbomembranous anastomotic urethroplasty in men with urethral injuries that are associated with pelvic bone injury [567]. In general, the recurrent rate of posterior urethral stenosis after bulbomembranous anastomotic urethroplasty is 14% to 25% [478]. More recently, Breyer et al. [9] reported that the overall primary stenosis-free survival rates at 1, 3, and 5 years were 88%, 82%, and 79%, respectively. In the case of posterior urethral injuries with pelvic bone fractures, the recurrence rate is 13.1% in Italy and 21.4% in India [6]; however, this study is not a pure representation of the recurrence rate bulbomembranous anastomotic urethroplasty because the data included other surgical methods such as urethrotomy and urethrostomy. Thus, the recurrence rate of urethral stenosis associated with pelvic bone injury after bulbomembranous anastomotic urethroplasty has not been well established.
As previous studies have emphasized, the outcomes after bulbomembranous anastomotic urethroplasty are influenced not only by defect length but also by several other factors, such as the cause of injuries [910]. In addition, PFUI was produced most commonly as a consequence of pelvic bone fracture, which may occur in up to 25% of cases [1112]. If not managed properly, this can lead to a lifelong condition with deleterious consequences that may compromise not only the ability to urinate and maintain urinary continence but also fertility [1314]. Until now, the surgical outcomes of urethral injuries in the setting of pelvic bone fractures are not well known. This study focuses on and analyzes the impact of pelvic bone fractures in urethral injury by evaluating and comparing the outcomes and differences in stenosis recurrence rate after bulbomembranous anastomotic urethroplasty in two groups divided based on the presence of pelvic bone fractures.
Go to : 
MATERIALS AND METHODS
1. Patients
This study was approved retrospectively by the Institutional Review Board of CHA Medical Center (approval number: CHAIRB013). The requirement for written consent was waived because of the retrospective study. We retrospectively analyzed the medical charts of patients evaluated and treated for posterior urethral injuries at a single institution by a single surgeon from December 2001 to May 2017. All patients underwent simultaneous retrograde urethrography (RUG) and combined cystourethrography (CCUG), and only men with posterior urethral injury were included in this study. These patients had received bulbomembranous anastomotic urethroplasty for posterior urethral injury. In total, 197 male patients with posterior urethral injury were included in the study. We excluded patients with less than a 1-year follow-up period or an anterior urethral stenosis. We also excluded patients who had an atonic bladder on the preoperative urodynamic study or who had missing relevant data. The 197 eligible patients were stratified into two groups according to the co-existence of pelvic bone fracture. There were 92 patients who had posterior urethral stenosis with pelvic bone fracture, and the other 105 patients had no accompanying pelvic bone fracture.
2. Surgical technique
All bulbomembranous anastomotic urethroplasty were performed by a single surgeon. All patients were placed in a lithotomy position and made an inverted Y-shaped perineal incision. The distal urethral end was identified by retrograde passage of a metallic urethral sound and the proximal urethral end was identified by antegrade passage of a metallic urethral sound through the suprapubic cystostomy tract. After measuring the extent of the urethral stenosis, all fibrotic tissues of the urethral stenosis including any peri-urethral scar tissue were excised completely. To avoid tension on the suture site, urethral anastomosis was performed by using a progressive perineal approach for mid-line separation of the proximal corporal bodies, inferior pubectomy, and supracorporal urethral rerouting. If scar tissue extended above the supra-montanal prostate, combined abdominal perineal exposure was created through a midline infra-umbilical incision. The proximal and distal ends of the urethra were spatulated and an anastomosis between the two ends was performed over a 16-Fr silicon urethral catheter using 4-0 or 5-0 Vicryl sutures. We sometimes used gracilis muscle flap (GMF) to reduce dead space after posterior urethral anastomosis. The skin incision was made parallel to the long axis of the gracilis muscle of the left thigh. The gracilis muscle was dissected from the medial aspect of the left thigh and released from its insertion. The GMF was rotated, and its distal end was brought to the perineal anastomotic urethra, and the perineal defect was filled with the rotated GMF. In most cases, suprapubic cystostomy was performed simultaneously. At 3 weeks after the bulbomembranous anastomotic urethroplasty, pericatheter RUG was performed. If there was no leakage of contrast media, the urethral Foley catheter was removed. Otherwise, the Foley catheter was left in place, and the pericatheter RUG was repeated 1 to 2 weeks later. The suprapubic tube was clamped and removed only when the patient showed a reasonably good ability to void through the urethra.
3. Outcomes analysis
The patient variables that were collected preoperatively included age, cause of injuries, previous operation history and body mass index (BMI). The operation duration, the amount of blood loss estimated by calculating the blood amount collected in the suction container as well as the difference in the weights of dry and blood soaked sponges, and any perioperative complications described in the medical records were thoroughly reviewed. Urethral defect length (cm), which was defined as the injured longitudinal length to repair, was measured using a CCUG. Recurrence was defined as the need for any postoperative intervention such as urethrotomy or repeat urethroplasty. Additional postoperative interventions, which were mainly endoscopic internal urethrotomies, were conducted in the patients complaining of voiding discomfort and who had Qmax less than 15 mL per second, greater than 150 mL post-voiding residual urine, or a narrowed urethral caliber on follow-up RUG. We also defined postoperative incontinence as the need for pads and intermittent leakage of urine during abdominal straining. In addition, impotence was defined as being unable to perform sexual intercourse. We investigated outcomes after bulbomembranous anastomotic urethroplasty and the recurrence of urethral stenosis according to the presence of pelvic bone fractures. Secondly, we investigated the functional outcomes of incontinence and impotence after bulbomembranous anastomotic urethroplasty according to the presence of pelvic bone fracture. Postoperative surgical complications were defined according to the Clavien classification system [14].
The data are presented as means±standard deviation. Student t-test or the Mann–Whitney U-test was used for continuous data to evaluate comparisons between the groups. The chi-squared test was used for categorical data. Recurrence-free duration of urethral stenosis was evaluated using the Kaplan–Meier method. Cox proportional hazards regression analysis was performed to identify multivariable predictors of recurrence rate of urethral stenosis. Hazard ratios (HRs) were calculated to provide a relative risk between variables. All p-values were set at 0.05 to define statistical significance. Statistical analyses were performed using IBM SPSS Statistics for Windows version 19.0 (IBM Corp. Armonk, NY, USA).
Go to :
RESULTS
Among the 197 patients, 92 had pelvic bone fracture and 105 did not have pelvic bone fracture. The mean age was 41.0±15.1 years, the mean urethral defect size was 2.6±1.5 cm, and 77 patients (39.1%) had a history of previous urethral surgeries at another hospital.
As shown in Table 1, urethral defect length was not significantly different between the two groups (2.68 vs. 2.69 cm, p=0.956). Most patients in the pelvic bone fracture group had mechanical traumatic events, including car accidents and crushing accidents, but most of the patients in non-pelvic bone fracture group had straddle trauma accidents (p<0.001). The patients with pelvic bone fracture were more likely to have involvement of the prostatic urethra compared to the intact pelvic bone group (3.8% vs. 17.4%). There was no significant difference in previous urethral manipulation between the pelvic bone fracture group (33/92, 35.9%) and the intact pelvic bone group (44/105, 41.9%). Furthermore, when considering methods of urethral lengthening, the patients with pelvic bone fracture underwent inferior pubectomy and rerouting of the urethra more often (28.6% vs. 41.3%, p=0.046; 18.1% vs. 29.3%, p=0.048).
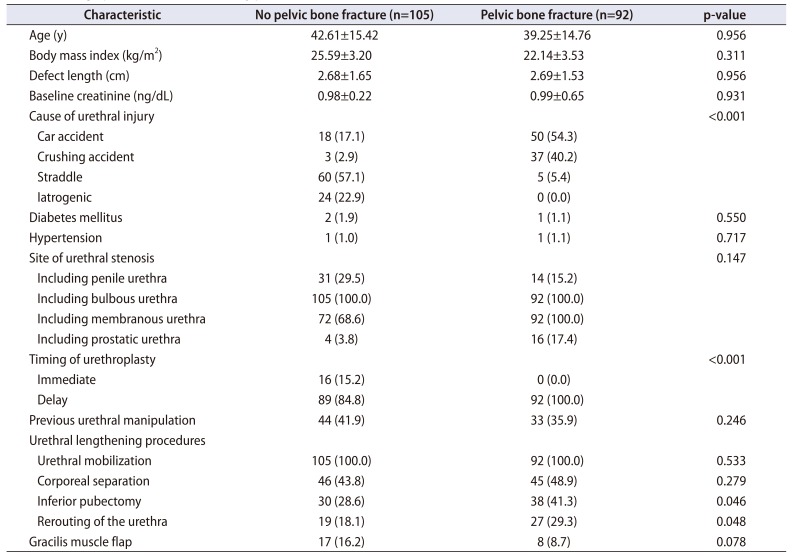
Table 1
Demographic characteristics of study patients
![]()
Intra-operative and post-operative outcomes are summarized in Table 2. Estimated blood loss and operation duration were not significantly different between the two groups. Although the mean Qmax was not significantly different between the two groups, (23.14 mL/s vs. 24.76 mL/s, p=0.364) the urethral stenosis recurrence rate was higher in the pelvic bone fracture group (42/92, 45.7%) than in the intact pelvic bone group (27/105, 25.7%). The incidence rate of grade III–IV complications after bulbomembranous anastomotic urethroplasty was 1.9% in the intact pelvic bone group and 5.4% in the pelvic bone fracture group, depending on the definition of Clavien classification (p=0.154).
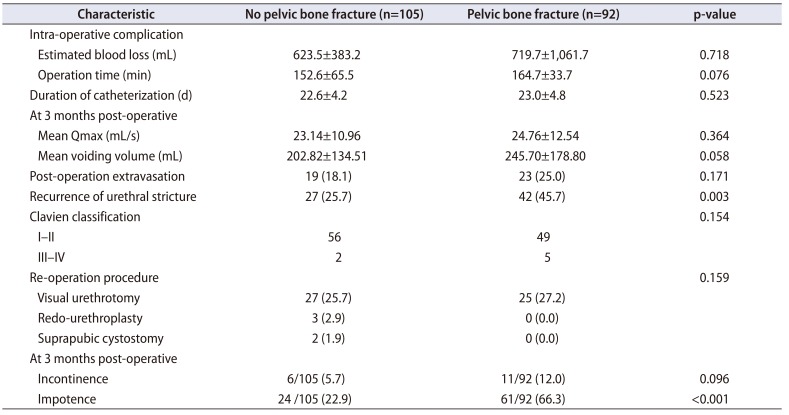
Table 2
Perioperative outcomes according to presence of pelvic bone fracture
![]()
There was no significant difference in the ability to maintain urinary continence as measured 3 months after bulbomembranous anastomotic urethroplasty between the two patient groups (5.7% vs. 12.0%, p=0.096), but a significantly higher rate of impotence was shown in the pelvic bone fracture group compared to the intact pelvic bone group (22.9% vs. 66.3%, p<0.001).
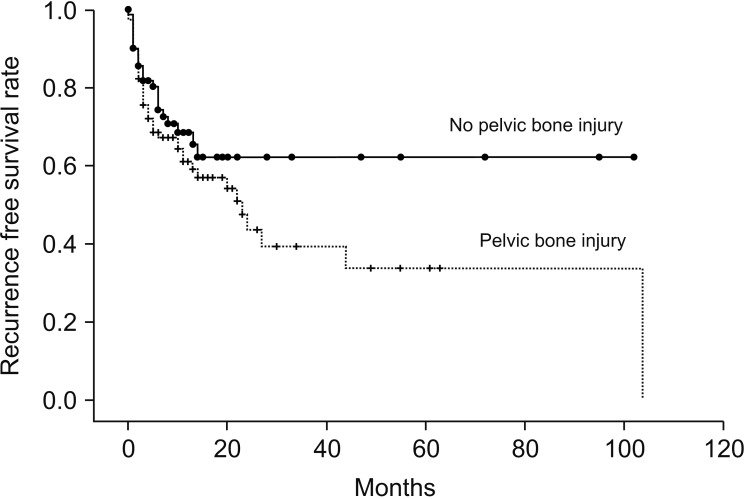
The recurrence rate of urethral stenosis according to the presence of a pelvic bone fracture was compared by Kaplan–Meier analysis (Fig. 1). During a median follow-up duration of 23.6 months, the recurrence rate at 5 years was significantly lower in the pelvic bone fracture group than in the intact pelvic bone group (40.9% vs. 27.4%, p=0.003).
To investigate the predictors for recurrence of urethral stenosis after bulbomembranous anastomotic urethroplasty, a Cox proportional hazard analysis was conducted and showed that the presence of pelvic bone injury was a significant predictor for the outcome of bulbomembranous anastomotic urethroplasty after adjusting for several factors, such as age, BMI, urethral defect length, urethral defect site, and previous urethral manipulation. Table 3 shows to identify predictive factor for recurrence of urethral stenosis. Pelvic bone injury is a significant risk factor for recurrence of urethral stenosis (HR, 2.155; 95% confidence interval [CI], 1.145–4.057; p=0.017). Furthermore, urethral defect length (HR, 1.339; 95% CI, 1.097–1.636; p=0.004) and previous urethral manipulation (HR, 2.159; 95% CI, 1.184–3.938; p=0.012) were also significant risk factors for recurrence of urethral stenosis after bulbomembranous anastomotic urethroplasty.

Table 3
Cox proportional hazard model predicting recurrence of urethral stenosis after bulbomembranous anastomotic urethroplasty
![]()
Go to :
DISCUSSION
Although there have been many studies investigating the etiology of posterior urethral injuries, few studies have focused on the results of bulbomembranous anastomotic urethroplasty according to the presence of pelvic bone injury [31516]. In this study, bulbomembranous anastomotic urethroplasty in men with pelvic bone injuries had fewer successful outcomes than in men without pelvic bone injuries. Even after adjusting for factors that influenced the recurrence rate, such as age, urethral defect length, defect site and history of previous urethral manipulation, the presence of pelvic bone fractures was still a significant factor that predicted the recurrence of urethral stenosis in patients who underwent bulbomembranous anastomotic urethroplasty.
Bulbomembranous anastomotic urethroplasty still remains the gold standard therapeutic method for posterior urethral injuries because of its low rates of stricture recurrence [17]. In a systematic review, the overall posterior urethral stenosis recurrence rate after bulbomembranous anastomotic urethroplasty was 17.5% between 2000 and 2008 [18]. In meta-analysis results, surgical treatment of bulbomembranous anastomotic urethroplasty was accompanied by a success rate of 82% to 95% [19]. In some nations, bulbomembranous anastomotic urethroplasty is the most cost-effective therapeutic modality for repeat endourological intervention [20]. In this study, the overall recurrence rate after bulbomembranous anastomotic urethroplasty was approximately 35.0%, but in cases with pelvic bone fracture, the urethral stenosis recurrence rate was 45.7%, which was higher than the rate for all patients in this study. This higher urethral stenosis recurrence rate was likely due to the fact that many patients had already received previous urethroplasties or endoscopic urethral surgeries at other institutions (77/197, 39.1%). In addition, the strict definition used for recurrence of urethral stenosis in our study might have resulted in a higher rate of recurrence.
Factors that can predict the success of bulbomembranous anastomotic urethroplasty are not still well established. Roehrborn and McConnell [21] attempted to identify factors that may predict failure of urethroplasty, and they found that the factor with the greatest impact on urethroplasty outcome was previous manipulation of the urethra. Similarly, Breyer et al. [9] argued that prior urethroplasty (HR, 1.8; 95% CI, 1.1–3.1; p=0.03) and failed endoscopic therapy (HR, 1.7; 95% CI, 1.0–3.0; p=0.04) were predictive of treatment failure. Scarberry et al. [2] argued that previous intervention in the form of endoscopic realignment or urethroplasty had adverse effects on the success rate of anastomotic urethroplasty (p<0.05). They also argued that stenosis length and patient age did not influence the outcome of urethroplasty. In our study, previous urethral manipulation was also a significant predictor for recurrence of urethral stenosis. These results indicate that healthy tissue adjacent to the urethra is an important factor for maintaining urethral patency. However, the aforementioned study did not evaluate pelvic bone injury, so, to our knowledge, our study is the first study to investigate the effect of pelvic bone injury in men undergoing of bulbomembranous anastomotic urethroplasty.
Surgical technique is also an important factor in the success of urethroplasty. Koraitim [22] asserted that incomplete excision of scar tissue, inadequate fixation of the prostatic mucosa, and anastomotic tension were predictive of surgical failure. In our study, urethral defect length (HR, 1.339; 95% CI, 1.097–1.636; p=0.004), prostatic urethra injury (HR, 1.041; 95% CI, 1.01–1.06), and pelvic bone injury (HR, 2.155; 95% CI, 1.145–4.057; p=0.017) were predictive of urethral stenosis recurrence. Unlike other studies, we showed that urethral defect length and the presence of pelvic bone fracture are important factors and significant predictors for urethral stenosis recurrence.
Pelvic bone fractures causing disruption at the bulbomembranous junction remain the main cause of posterior urethral injury. The optimal timing of surgery (emergency or delayed) and methods of surgical intervention (open or endoscopic) are still unclear. The debate revolves around the risk of late complications, which may occur as a direct consequence of injury or because of initial treatment. Moreover, the impact of pelvic bone fractures on bulbomembranous anastomotic urethroplasty is not clear. To that regard, this study has shown that pelvic bone fractures are closely related to recurrence of urethral stricture.
Vascularity and the degree of injury are the most important factors for success of urethroplasty [23]. Generally, the normal urethra and spongiosum tissue must have sufficient innervation and microvasculature to maintain their elastic and compliant properties [24]. However, an injured urethra loses its relationship between the smooth muscle, extracellular matrix, and vascular sinusoid [25]. After a urethral injury with a pelvic bone fracture, the urethra and surrounding pelvic tissues are injured by trauma, which leads to a decrease in vascularity; thus, the periurethral tissues are no longer supplied with vascularity. The initial injury recovers by forming a surrounding hematoma and fibrosis, and these factors make accurate identification of the anatomical planes difficult, requiring meticulous dissection. As a result, impaired vascularity and persistent inflammation prevent continuous healing of the urethra [26]. Furthermore, a study on microvascular damage caused by smoking in men who underwent urethroplasty also revealed environmental factors affecting the surrounding urethra tissue, which were important factors affecting success [9].
For post-operative complications, the patients with pelvic bone fracture had a higher rate of impotence than those without pelvic bone fracture at 3 months postoperatively (22.9% vs. 66.3%, p<0.001). Although our study differed in its time at evaluation, the impotence rate was similar to other papers [272829], which reported that the incidence of impotence ranged from 60% to 72% when assessment was performed 3 to 15 months after pelvic bone injury. Still, Koraitim [30] argued that spontaneous recovery of sexual function could occur up to 2 years after injury as a result of neuropraxis and the rehabilitation of accessory penile arterial supply. So far, several risk factors for impotence after pelvic bone injury have been identified. Malavaud et al. [14] presented significant potential factors, including pubic diastasis. Anger et al. [27] suggested that posterior urethral disruption and/or other injuries associated with urethral disruption have a significant impact on cavernous nerves.
Our study has several limitations. First, its retrospective nature may have caused selection bias. Although we adjusted for several factors that influenced the outcomes, there were still unconfirmed factors that might have influenced the outcomes of the study. This could be addressed by conducting a prospective, large-scale, cohort study. Secondly, this study has as its limitation the presence of significant numbers of cases with straddle or iatrogenic injury in the posterior urethral stenosis group without pelvic bone fracture. This group consisted mostly of patients with stenosis extending from the distal membranous urethra to the bladder neck secondary to repeated endourologic procedures and previous bulbomembranous anastomotic urethroplasty's as the primary etiology, although these are less likely to cause posterior urethral stenosis. This limitation is due to an extremely lack of experienced physicians in Korea who can perform appropriate procedures once posterior urethral stenosis occurs and the position of this medical center as a referral hospital. Another limitation is the difference between the baseline characteristics of the two groups, including etiology, time of bulbomembranous anastomotic urethroplasty, and the type of procedures used for urethral lengthening. Since these differences may affect functional outcomes, the corresponding differences make assessment of the results difficult and may deteriorate the credibility of the results. Lastly, among the complications, we could not use validated questionnaires to assess erectile function and continence preoperatively and postoperatively. The recording of urinary and sexual function was not based on qualitative or semiquantitative measurement. It also should be validated by well-designed prospective studies.
Go to :
CONCLUSIONS
The patients with posterior urethral injuries associated with pelvic bone fracture had a higher rate of urethral stenosis recurrence after perineal bulbomembranous anastomotic urethroplasty than patients without pelvic bone fracture. We postulated that the higher recurrence rate of urethral injury in the group with pelvic bone fractures was associated with micro-environmental factors, which included the inflammatory response and microvascular vulnerability. These results should be validated by a prospective, large-scale, cohort study.
Go to :
 XML Download
XML Download