

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Erectile dysfunction (ED) and lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH) often occur in older males [1]. The association between ED and LUTS has been previously shown in various large-scale community-based studies [2345]. Approximately 70% males with LUTS/BPH have concurrent ED [6]. As the population ages, the number of males with all the three conditions is increasing, and these conditions can have a profound impact on quality of life [7].
While α-blockers and phosphodiesterase type 5 (PDE5) inhibitors are effective in alleviating LUTS and ED, respectively, polypharmacy (which is most commonly defined as taking ≥5 medications) is considered for patients with a high prevalence of medical comorbidities (e.g., hypertension, diabetes mellitus, and metabolic syndrome) that need multidrug therapy [8]. Polypharmacy can increase adverse drug reactions and medication noncompliance, especially in the elderly [9]. To improve compliance, a fixed-dose combination (FDC) medication that shows efficacy and safety needs to be developed.
A recent randomized controlled trial investigating the efficacy and safety of a once-daily FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) showed that the FDC of tadalafil (5 mg) and tamsulosin (0.4) mg was superior to that of tadalafil (5 mg) monotherapy for LUTS/BPH treatment and was similar to that of tadalafil (5 mg) monotherapy for ED treatment; no clinically significant safety issues were observed [10]. As a result, it was approved for use in Korea by the Korean Food and Drug Administration and released under the tradename “Gugutams 0.4/5 mg®” in 2016 [11].
Single-tablet administration is expected to improve treatment compliance; however, adherence to a once-daily single-tablet FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) has never been investigated. Furthermore, there are no published data regarding treatment patterns in males receiving an FDC of tadalafil (5 mg) and tamsulosin (0.4 mg), especially in real-world practice settings. Thus, the primary aim of this study was to assess treatment persistence with a once-daily single-tablet FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) in males with LUTS/BPH and ED over a 6-month period. The secondary aim was to identify the reasons for treatment discontinuation over a follow-up period of 6 months.
Go to : 
MATERIALS AND METHODS
1. Study design and subjects
This was a retrospective, observational, and single-center study (Korea University Guro Hospital, Seoul) of males with LUTS/BPH and ED who received a prescription for a once-daily single-tablet FDC of tadalafil (5 mg) and tamsulosin (0.4 mg). Adults aged ≥18 years who were first prescribed the target drug between July 2017 and February 2018 were eligible for inclusion. This period was based on the availability of an FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) and the need for at least 6 months of patient follow-up. The main exclusion criteria were as follows: episodic treatment, less than 6 months of treatment, and/or insufficient data for analysis. The first prescription date for an FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) was defined as the index date. One hundred and thirteen patients received their first prescription of an FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) during the study period. Of them, 16 patients were excluded because the follow-up period was less than 6 months. Therefore, only 97 patients were included in this study.
The patients' medical records were reviewed for demographic information, previous and concomitant medications, and symptom questionnaires, including International Prostate Symptom Score (IPSS) and International Index of Erectile Function-5 (IIEF-5) before the index date. The study protocol was reviewed and approved by the Institutional Review Board (IRB) of Korea University Guro Hospital (approval number: 2019GR0221). The need for informed consent was waived by the IRB based on the retrospective nature of the study.
2. Study outcomes
The primary outcome measures were treatment persistence and factors associated with treatment persistence with an FDC of tadalafil (5 mg) and tamsulosin (0.4 mg). Treatment persistence was measured from the index date to the discontinuation date of the target drug. Data on the mean time to discontinuation and the persistence rate at 6 months were obtained. Age, polypharmacy, baseline symptom severity, and previous treatment status were considered factors associated with treatment persistence. Previous treatment status was subdivided into a treatment-naive group, defined as having no experience with coadministration of α-blockers and PDE5 inhibitors before the index date, and a treatment-experienced group, defined as having experience with α-blockers and PDE5 inhibitors before the index date. The secondary outcome was the identification of the reasons for discontinuation. Causes of treatment discontinuation were classified as follows: side effects, inconvenience of daily administration, perceived poor efficacy, patient preference (i.e., seeking other treatment options), and drug cost.
3. Statistical analysis
The baseline characteristics of patients were analyzed descriptively. Categorical variables were reported as number and percentages, while continuous variables were reported as mean±standard deviation (range). Kaplan–Meier curves were used to present the cumulative discontinuation rate over 6 months. Differences in treatment persistence according to the demographics and clinical variables were assessed using a log-rank test. The bivariate Cox proportional hazard model was used to identify factors associated with treatment discontinuation. Factors associated with the dependent variable at a value of p<0.05 were included in the multivariate logistic regression model. The causes of discontinuation in the cohort were analyzed descriptively. All analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). All p-values <0.05 were considered significant.
Go to :
RESULTS
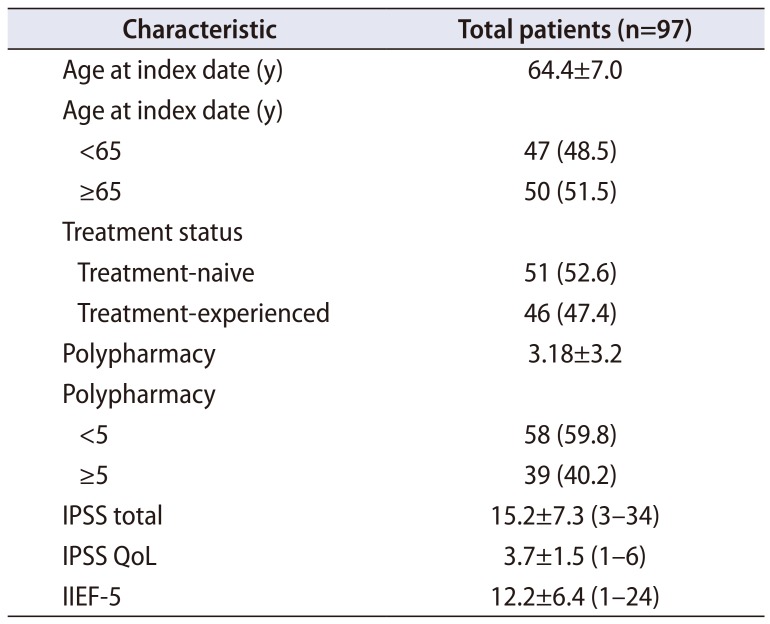
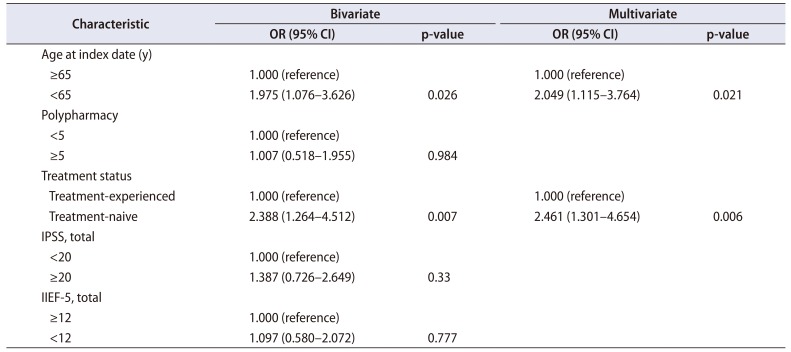
Baseline clinical characteristics of these patients are presented in Table 1. Overall, 44 of 97 patients (45.4%) discontinued their treatment within 6 months. The mean time to treatment discontinuation (95% confidence interval [CI]) was 125 days (112.6–138.4). The cumulative persistence rate at 30, 90, and 180 days was 88.7%, 66.0%, and 54.6%, respectively (Fig. 1). The cumulative persistence was significantly different after stratifying patients by previous treatment status (log-rank p=0.005) and age (log-rank p=0.024). However, no difference in cumulative persistence was found regarding polypharmacy (log rank p=0.984) and symptom severity, according to patient questionnaires, including IIEF-5 (log rank p=0.775) and IPSS (log rank p=0.315) (Fig. 2). Additionally, previous silodosin (8 mg) or tamsulosin (0.4 mg) medication history and concurrent hypertension medication status did not affect cumulative persistence (log rank p=0.112 and p=0.930, respectively). The results of bivariate and multivariate analysis revealed that younger patients (odds ratio [OR], 2.049; 95% CI, 1.115–3.764; p=0.021) and patients in the treatment-naive group (OR, 2.461; 95% CI, 1.301–4.654; p=0.006) were more likely to discontinue therapy within 6 months (Table 2).
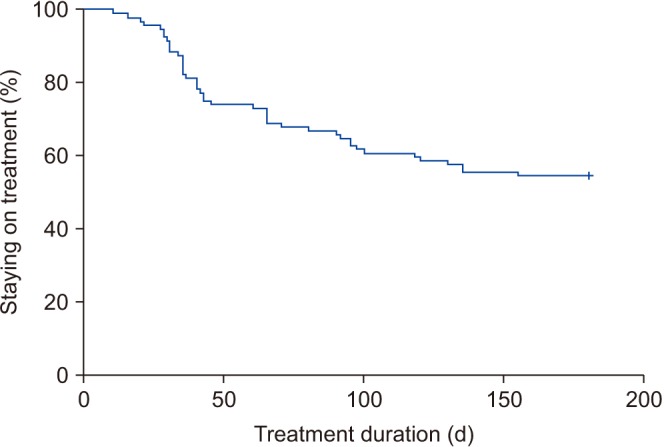 | Fig. 1Kaplan–Meier curves for treatment continuation over 6 months in patients who received a fixed-dose combination of tadalafil (5 mg) and tamsulosin (0.4 mg).
|
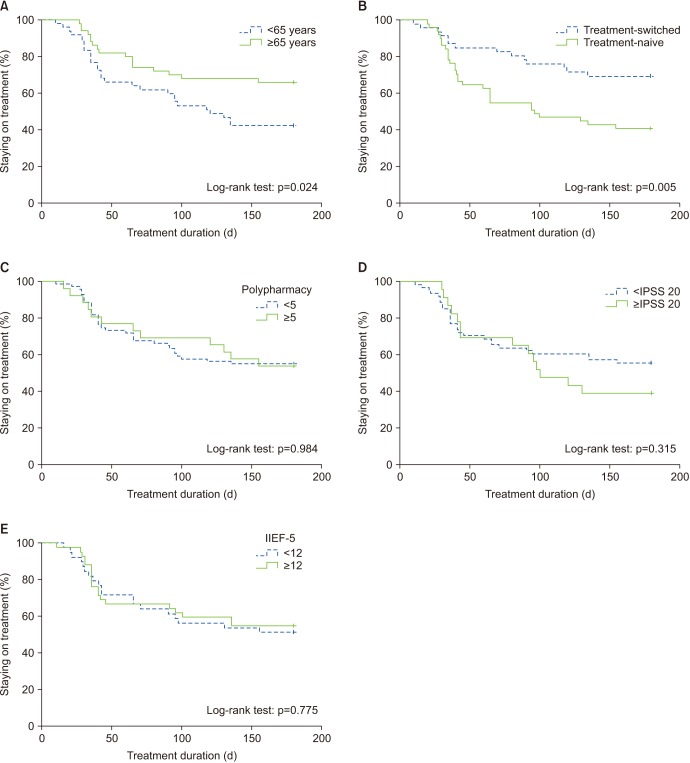 | Fig. 2Kaplan–Meier curves showing the cumulative persistence after stratifying patients by (A) age, (B) previous treatment status, (C) polypharmacy, (D) International Prostate Symptom Score (IPSS), and (E) International Index of Erectile Function-5 (IIEF-5).
|
Table 1
Baseline characteristics of patients
![]()
Table 2
Bivariate and multivariate Cox regression analysis for predicting factors associated with treatment persistence
![]()
The most common reasons for discontinuation were side effects (63.6%), perceived poor efficacy (22.7%), cost (9.1%), and inconvenience of daily usage (4.5%) (Table 3). Ejaculatory dysfunction and dizziness were the most commonly reported adverse events (Table 3).
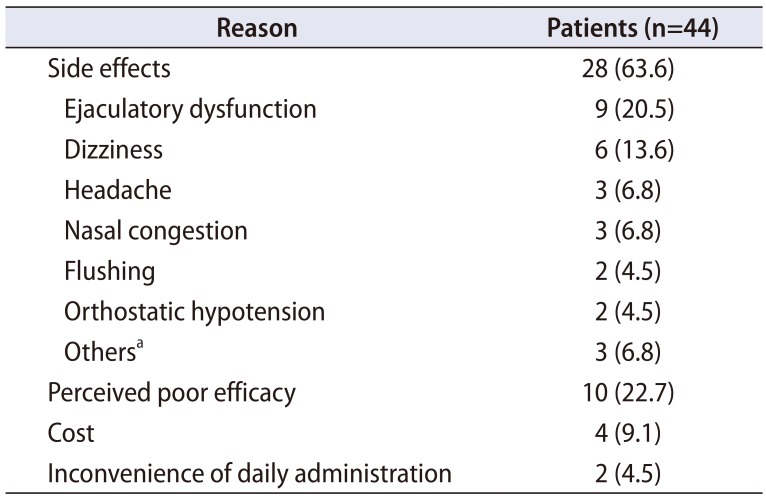
Table 3
Reasons for treatment discontinuation within 6 months
![]()
Go to :
DISCUSSION
As males age, ED symptoms and LUTS tend to increase in severity concurrently [12]. Both LUTS and ED worsen with aging; hence, long-term treatment is required. Therefore, as with other chronic diseases, persistence and compliance for LUTS and ED medications are important for improving the patient's symptoms and quality of life [1314]. Although it is expected that the use of an FDC will result in treatment persistence and compliance, this has never been investigated in a real-world practice setting. This study is the first retrospective, longitudinal observational study to evaluate the treatment persistence with a once-daily FDC of tadalafil (5 mg) and tamsulosin (0.4 mg).
In this study, we found that 45.4% patients discontinued the FDC medication within 6 months. This finding was similar to that in previous Korean studies evaluating treatments for other urologic conditions, including LUTS/BPH and overactive bladder [151617]. However, this finding was much lower than that in previous western studies evaluating treatment persistence with once-daily tadalafil for ED [18]. Unfortunately, no study has evaluated treatment persistence with once-daily tadalafil in Korea. Interestingly, the discontinuation rate in our study was much higher than that in a previous phase 3 clinical trial of an FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) [10]. The lower discontinuation rate in clinical practice was due to increased patient motivation and cooperation with prescribed recommendations in the clinical trial setting [10]. Moreover, in phase 3 clinical trials, patients are given their medication without cost and are intensively observed during the study period [19]. This may enhance the persistence rate. In contrast, in real-world clinical practice, patients pay for their medication, which might lead to higher expectations and increased vulnerability to side effects with their prescription. These factors allow more enlightening clinical studies to be carried out in real-world practice settings; therefore, actual treatment persistence rates may be more accurate.
The most common reason for treatment discontinuation in this study was adverse drug side effects. Although most side effects were self-limiting, they were directly related to the patient's satisfaction with treatment. The most common undesirable effect was ejaculatory dysfunction, a well-known side effect of selective α-blockers [20]. This has previously been shown to be the main factor related to low satisfaction with combination treatment using α-blockers and PDE5 inhibitors [21]. However, other adverse events related to tadalafil may have less impact on treatment persistence, based on previous studies with once-daily tadalafil that reported discontinuation rates due to the side effect as low as 1% to 6% [222324]. Therefore, it can be inferred that ejaculatory dysfunction was a major cause for discontinuation of a once-daily FDC of tadalafil (5 mg) and tamsulosin (0.4 mg). Interestingly, none of the 9 patients who discontinued due to ejaculatory dysfunction received silodosin or tamsulosin (0.4 mg) before taking a once-daily FDC of tadalafil (5 mg) and tamsulosin (0.4 mg).
In this study, patients who were treatment-naive for α-blockers and PDE5 inhibitors were more likely to discontinue treatment early. This is understandable when considering side effects were the main cause for withdrawal. It is also noteworthy that the persistence rates were high in the treatment-experienced group, who had previous coadministration of α-blockers and PDE5 inhibitors. The high persistence rate may be because treatment-experienced patients probably did not switch to an FDC when they had side effects. Another factor associated with treatment persistence was age. Patients aged <65 years were more likely to discontinue treatment at 6 months. Although reasons for this finding are unclear, we inferred that younger patients were more vulnerable to sexual side effects related to α-blockers.
Other potential factors associated with treatment persistence, including polypharmacy and subjective symptom severity, did not affect persistence rates. However, it is difficult to draw conclusions regarding the true effects of polypharmacy from these results as patients may have been receiving other treatments for various conditions. Further studies are needed to identify key factors associated with polypharmacy-related persistence.
In this study, the second most common reason for discontinuation treatment was the lack of response to treatment, regardless of symptom severity; treatment persistence and symptom severity were not correlated. The degree of symptom improvement had a more significant effect on treatment persistence than symptom severity.
This study has several limitations. First, patients who were excluded due to no recorded follow-up examinations could not be analyzed; it is unknown if they were receiving treatment from another hospital or discontinued treatment. Therefore, the persistence rate might be an overestimation. This is, however, an inevitable limitation due to the retrospective study design. Second, this study did not consider probable confounding factors of treatment persistence related to physicians. The doctor-patient relationship is well known to affect a patient's compliance with treatment [252627]. Therefore, further studies will need to evaluate whether satisfaction with the doctor affects treatment persistence. Third, the sample for this study was small and from one center. However, it has been less than 3 years since the drug was approved and prescribed. Moreover, this study was meaningful as an initial investigation of treatment persistence with a once-daily FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) and its related factors. A large scale, prospective trial considering these limitations should be performed to further investigate factors influencing FDC treatment persistence.
Go to :
CONCLUSIONS
In this study, 54.6% patients with LUTS and ED continued a once-daily FDC of tadalafil (5 mg) and tamsulosin (0.4 mg) for 6 months. Patients who had experience with coadministration of α-blockers and PDE5 inhibitors before the FDC prescription were likely to continue their treatment. The most common reason for discontinuation was adverse drug side effects. To improve patient compliance for a once-daily FDC of tadalafil (5 mg) and tamsulosin (0.4 mg), it is recommended to select patients who show adaptation to a combination of α-blockers and PDE5 inhibitors prior to FDC treatment.
Go to :
 XML Download
XML Download