

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Benign prostatic hyperplasia (BPH) is routinely treated using photoselective vaporization of prostate (PVP), and holmium laser enucleation of the prostate (HoLEP) laser prostatectomy, in addition to transurethral resection of the prostate (TURP) [12]. Thulium laser surgery has also proven to be a useful tool for managing lower urinary tract symptoms (LUTS) caused by BPH [34]. However, many patients with BPH have been taking 5α-reductase inhibitors (5ARIs) before surgery, and the preoperative use of 5ARIs is known to affect surgical efficiency. Furthermore, long-term use of 5ARIs usually increases the risk of prostate tissue fibrosis [5]. This effect can reduce the risk of intraoperative bleeding by decreasing the microvessel density in prostate tissue [6], although substantial fibrosis may also cause anatomical changes in the prostate capsule, which could ultimately complicate surgical treatment [7].
The usage of 5ARIs before TURP can reduce intra-operative bleeding, improve visibility, and reduce the risk of TUR syndromes [891011]. However, 5ARI use was thought to reduce the effectiveness of PVP laser surgery, which work by vaporizing prostate tissue. This is because PVP lasers vaporize the prostate gland based on their high affinity for hemoglobin, which is decreased because the 5ARI treatment reduces the microvessel density. Nevertheless, previous studies have demonstrated that 5ARI use did not influence the efficiency of PVP surgery [121314]. It is also possible that 5ARI use may increase the difficulty and decrease the effectiveness of HoLEP surgery, which requires precise identification of the prostate capsule or the interface between the transition and peripheral zones, although conflicting results have been reported regarding the effect of 5ARI use in this setting [7151617].
Thulium laser surgery is different from PVP and Ho-LEP prostatectomy in that the thulium laser can be used to selectively perform resection or enucleation while simultaneously vaporizing the prostate tissue [31819]. However, while various studies have examined the effects of preoperative 5ARI use on TURP, PVP, and HoLEP prostatectomy, we are not aware of any studies that have examined the effects of 5ARI use on thulium laser surgery. Therefore, this study examined the effects of preoperative 5ARI use on the efficacy and perioperative outcomes of thulium laser vaporesection for BPH.
MATERIALS AND METHODS
1. Study design
This study evaluated 184 patients who underwent thulium laser prostatectomy for BPH during 2012–2017. The exclusion criteria were a preoperative diagnosis of prostate cancer, neurogenic bladder, or having undergone prostate and urethral surgery. However, patients were not excluded if they received alpha blockers for LUTS caused by BPH. All patients with high prostate-specific antigen (PSA) before surgery underwent prostate biopsy. Only patients whose biopsy results were confirmed as ‘cancer negative’ underwent thulium laser surgery. Informed consent was obtained from all individual participants included in the study. The study's retrospective protocol was approved by our Institutional Review Board of Inje University Haeundae Paik Hospital (IRB no. 2012-030).
2. Study parameters
The patients had been assessed at various postoperative time points (6 weeks, 3 months, 6 months, and 12 months) to determine their International Prostate Symptom Score (IPSS), quality of life (QoL) score, maximum flow rate (Qmax), and postvoid residual urine volume (PVR). Each patient's prostate volume was measured preoperatively and at 6 weeks after surgery. Surgical efficiency was evaluated based on the total operative time, vaporesection time, laser activation time, and vaporesected tissue volume. The total operation time was defined as the time from the start of the anesthesia to the time the patient leaves the operating room. The laser activation time was defined as the time when the laser was being used.
The vaporesection time was defined as the time from the thulium laser resectoscope's insertion into the bladder until its removal from the bladder (i.e., including the laser activation time). The vaporesection efficiency was calculated as the vaporesection volume divided by the vaporesection time [(preoperative prostate size-postoperative prostate size)/vaporesection time]. The patients' preoperative 5ARI usage was classified as positive (5ARI+) or negative (5ARI−).
3. Thulium laser vaporesection
The thulium:yttrium-aluminium-garnet (YAG) vaporesection of prostate (Revolix®; LISA Laser Products OHG, Katlenburg, Germany) was performed similar to a TURP-like technique. The laser energy was transferred to the prostate through a 550-µm end-firing fiber using an energy setting of 60 W. The surgical procedure was performed using normal saline as an irrigation fluid and under spinal anesthesia. The first step involved an incision around the verumontanum at the 5 to 7 o'clock position to remove the median lobe. The lateral prostate lobes were then divided into several large lumps, which were vaporesected until the prostate capsule was near at hand. At the end of the operation, a 22-Fr 3-way Foley catheter was inserted to maintain bladder irrigation.
4. Statistical analysis
The patients' characteristics were reported using descriptive statistics, and differences between the 5ARI+ and 5ARI− groups were evaluated using the independent t-test or χ2 test, as appropriate. All statistical analyses were performed using IBM SPSS software (version 24; IBM Corp., Armonk, NY, USA). Differences were considered statistically significant at a two-tailed p-value of <0.05.
RESULTS
Table 1 shows the patients' baseline characteristics. The 184 eligible patients included 83 patients who had received 5ARIs (45.1%) and 101 patients who had not received 5ARIs (54.9%). A comparison of the two groups failed to detect significant differences in preoperative age, prostate volume, hemoglobin level, QoL score, Qmax, or PVR. Preoperative PSA level (3.4 ng/mL vs. 5.4 ng/mL) and IPSS score (20.0 vs. 24.0) showed a difference between the two groups.
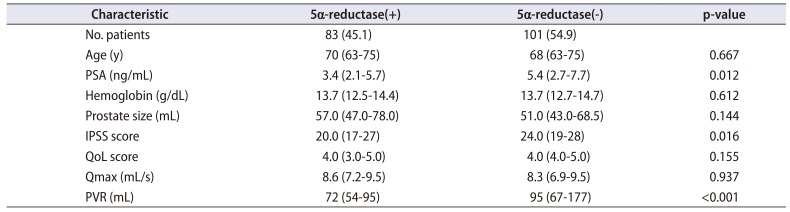
Table 1
Patients baseline characteristics
![]()
1. Surgical efficiency
Table 2 summarizes the patients' perioperative and postoperative characteristics. No significant inter-group differences were observed in the values for the postoperative prostate volume (27.0 mL vs. 25.0 mL), weight of the resected prostate tissue (11.0 mL vs. 9.0 mL), thulium energy used 68,363 J vs. 76,376 J). However, relative to the 5ARI− group, the 5ARI+ group had a significantly shorter operative time (65.0 min vs. 70.0 min, p=0.013), laser activation time (23.0 min vs. 24.0 min, p=0.024), and a significantly shorter vaporesection time (48.0 min vs. 54.0 min, p=0.014), which resulted in significantly higher vaporesection efficiency in the 5ARI+ group (0.66 mL/min vs. 0.51 mL/min, p<0.001) (Table 2). To observe how the surgical efficiency changes depending on the learning curve, we classified the year of surgery into 3 categories (Fig. 1). Although there was a difference in the surgical efficiency at the beginning according to the usage of 5ARI, as the experience of thulium laser surgery has accumulated, the difference in surgical efficiency between the two groups has disappeared. Fig. 2 shows that the 5ARI+ and 5ARI− groups both experienced improvements in their IPSS, QoL score, Qmax, and PVR during the 1-year followup. Supplementary Table 1 shows the previously reported effects of 5ARI use on the surgical efficiency of TURP or multiple alternative laser prostatectomy approaches [7891011121314151620].
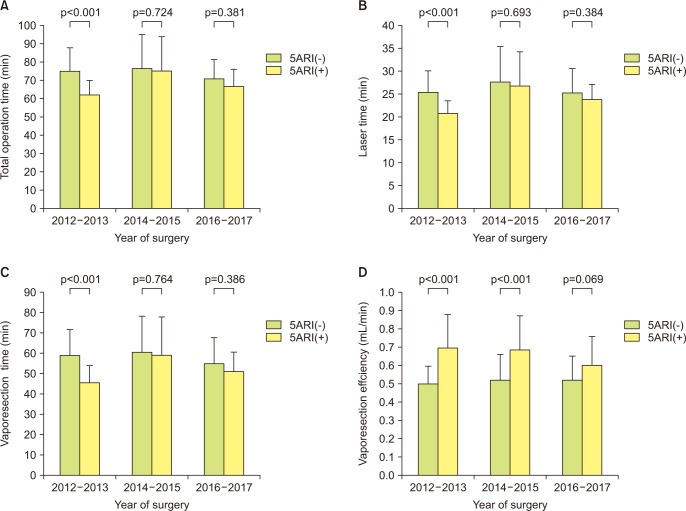
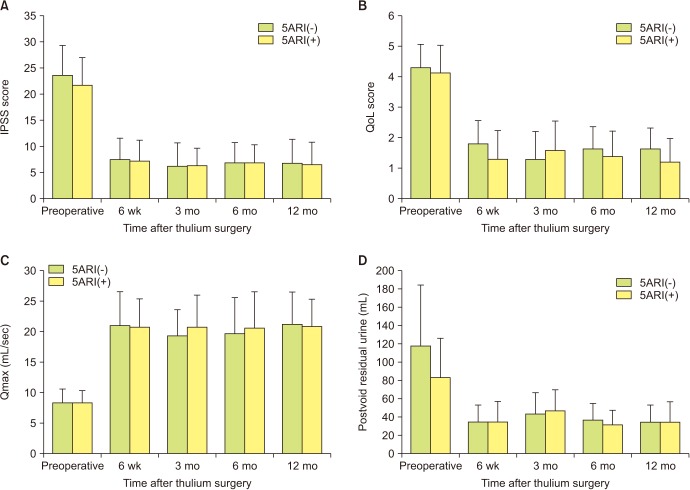
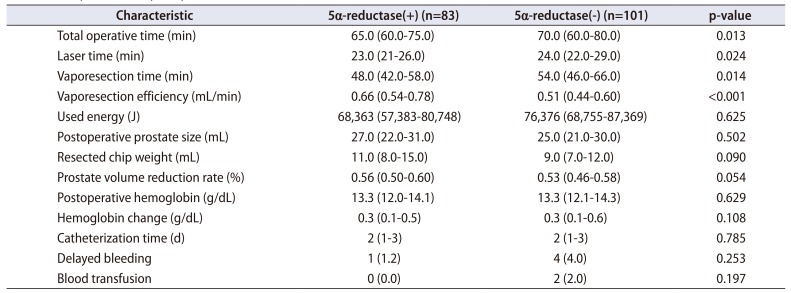
Fig. 1
The changes in surgical efficiency depending on the learning curve between the 5ARI(−) and 5ARI(+) groups. (A) Total operation time, (B) laser time, (C) vaporesection time, and (D) vaporesection efficiency. 5ARI, 5α-reductase inhibitor.
![]()
Fig. 2
Preoperative and follow-up urinary symptom and functional outcomes. (A) International Prostate Symptom Score (IPSS), (B) quality of life (QoL) score, (C) maximum flow rate (Qmax), (D) postvoid residual urine volume. 5ARI, 5α-reductase inhibitor.
![]()
Table 2
Perioperative and postoperative data
![]()
2. Complications
Only two patients in the 5ARI− group required blood transfusions. The 5ARI+ group had a non-significantly smaller reduction in hemoglobin (0.3 g/dL vs. 0.3 g/dL). Blood transfusion was observed for 0 of the 5ARI+ patients (0.0%) and 2 of the 5ARI− patients (1.5%), with similar results for delayed bleeding (Table 2). The remaining postoperative clinical outcomes, including the catheter insertion time, were comparable between the two groups (Table 2).
DISCUSSION
Use of 5ARIs effectively reduces the risk of BPH-associated hematuria by promoting prostate degeneration and inhibiting neovascularization. This approach is also very effective in treating LUTS that is induced by BPH, especially when it is used in combination with alpha blockers [212223]. Finasteride (a 5ARI) induces apoptosis of the prostate glandular epithelium cells and reduces the microvessel density of the prostate by remarkably decreasing the expression of suburethral VEGF [2324]. Dutasteride is another 5ARI that is known to cause fibrosis and reduce the prostate's size by reducing the thickness of prostate epithelial cells [25]. Interestingly, a magnetic resonance imaging-based study revealed that the prostate surgical capsule was clearly visible before starting 5ARI treatment, although the surgical plane became unclear after 18 months of this treatment [7]. Thus, although long-term 5ARI use may help address LUTS, it may also influence the efficiency of surgery for BPH by deforming the normal capsular structure and leading to inflammation and adhesion.
We speculated that preoperative 5ARI use would reduce the risk of perioperative bleeding, which could improve surgical efficiency by improving visibility in the operative field. However, we also hypothesized that 5ARI−related deformation of the normal prostate structure would ultimately complicate the thulium laser procedure, as the increased fibrosis would make it difficult to identify the interface between the adenoma and the surgical capsule. However, the present study revealed that the vaporesection efficiency of thulium laser prostatectomy was significantly better in the 5ARI+ group, which suggests that it may not be necessary to discontinue 5ARI use before thulium laser prostatectomy. Furthermore, the 5ARI+ group appeared to have better visibility in the operative field, based on the shorter operative time and increased surgical efficiency. There are several potential mechanisms that may explain this phenomenon. First, the 5ARI+ group had a smaller hemoglobin change after surgery, which would likely help improve visibility in the surgical field and the resulting surgical efficiency. Second, thulium laser vaporesection technique does not necessarily require the surgeon to identify the plane of the prostate adenoma and surgical capsule, and vaporesection of the prostate can be performed arbitrarily at the desired point. Thus, surgical capsule confirmation may not affect surgical difficulty, as the median and lateral lobes can be excised into several large lumps. Third, the patients in our study had typically been using 5ARIs for <6 months, which might had resulted in fairly limited prostate tissue fibrosis, as previous studies have indicated that the fibrosis was substantially greater at >2 years of 5ARI use relative to at <1 year of use [12]. Moreover, 5ARI treatment for only 2 to 4 weeks may help reduce perioperative bleeding [26], which might suggest that any decrease in surgical efficiency caused by prostate tissue fibrosis would occur after prolonged 5ARI use (e.g., ≥12 months). In this study, the unique finding was that there was a difference in the surgical efficiency between the two groups at the beginning. However, as the experience of thulium laser surgery has accumulated, the effect of 5ARI on the efficiency of thulium laser vaporesection gradually diminished over time. This requires further study with more patients.
Many studies have investigated the generally positive effects of preoperative 5ARI use on the outcomes of TURP, which include reduced perioperative bleeding, improved operative performance, shorter operative times, and a lower incidence of TUR syndrome [81120]. Although 5ARI use was thought to extend the operative time and reduce the efficiency of potassium-titanylphosphate (KTP)/PVP procedures, which rely on a high affinity for hemoglobin, reported results indicate that 5ARI use actually reduced the risk of perioperative bleeding while maintaining surgical efficacy [121314]. Furthermore, no reports have definitively described negative effects of 5ARI use on KTP/PVP laser surgery. However, there is controversy regarding whether 5ARI use influences HoLEP outcomes, as studies have revealed improvements in the enucleation efficiency, no notable outcomes, or even an increased surgical difficulty [71516]. Warner et al. [15] reported that preoperative 5ARI use appeared to improve the enucleation rate without altering the surgical outcomes, relative to in patients who did not preoperatively use 5ARIs. Monn et al. [16] also reported a trend towards faster enucleation and morcellation times in patients with 5ARI treatment, although those trends did not reach statistical significance. In contrast, Sato et al. [7] suggested that preoperative 5ARI use might increase the difficulty of the HoLEP procedure, as patients who were taking 5ARIs had a lower enucleation rate and greater objectively assessed surgical difficulty.
This study has several important limitations. First, the retrospective design and small sample size are associated with risks of bias. Second, the surgical outcomes could not be classified according to the duration of 5ARI use, because of a lack of data, and it is possible that the effect of 5ARI use on the efficiency of thulium laser surgery could be influenced by both prostate size and the duration of 5ARI use. Third, all patients underwent thulium laser surgery with the same energy setting 60 W. However, it is difficult to completely exclude the possibility that the results will vary depending on the energy power. Therefore, larger prospective studies are needed to address these issues and validate our findings.

 XML Download
XML Download